
Abstract
Background:
Dengue is a febrile illness that is most common in tropical areas but is recognized worldwide as one of the most important arbovirus diseases of humans. This febrile illness generally has a course with mild alterations in white blood cell count, but there are also rare cases of severe neutropenia or agranulocytosis during dengue infection. Clozapine (CLZ) remains the most effective treatment for schizophrenia, but because of its poor side effect profile, in particular due to the increased risk of neutropenia and agranulocytosis, it is generally used for patients whose condition responds poorly to other antipsychotics.
Methods:
We report three cases of dengue infection in patients with refractory schizophrenia who were using CLZ, and we discuss the implications of this infection on the continuation of CLZ treatment in these patients.
Results:
Of these three cases with dengue infection and co-occurence of CLZ use, the first would be classified as severe neutropenia and the second as moderate leucopenia; the last case had a white blood cell (WBC) count inside the normal range, and had no need to change his antipsychotic. The first and the second patient presented a worsening in their schizophrenic psychopathologies, after CLZ withdrawal, evolving into catatonic states, that were reverted after the careful reintroduction of CLZ.
Discussion:
It is very likely that during dengue epidemics many patients with schizophrenia and using CLZ have their treatment permanently discontinued given WBC count concerns, causing relapse of symptoms of schizophrenia and impairment of quality of life of these patients.This is the first report of neutropenia cases among CLZ-treated patients during dengue infection that describes the withdrawal of CLZ and its successful readministration.
Introduction
Dengue has become a major international health concern, with some countries, such as Brazil, experiencing annual epidemics [McBride and Bielefeldt-Ohmann, 2000; Schmidt, 2010; Barreto et al. 2011]. There are different forms and clinical manifestations of the disease, with the most severe being the life-threatening dengue hemorrhagic fever (DHF)/dengue shock syndrome [Onlamoon et al. 2010]. The most common manifestation of this disease, classic dengue fever, is a mild febrile illness that is characterized by fever, musculoskeletal pain, severe headache, pain behind the eyes, nausea and vomiting, maculopapular rash, leucopenia and thrombocytopenia [WHO, 1997]. Severe thrombocytopenia is often present in DHF cases, but not in classic dengue fever, when just mild thrombocytopenia generally occurs. Leucopenia, generally a consequence of neutropenia, is typical and generally found among patients with dengue as a mild reduction of white blood cell (WBC) count. However, there are also rare cases of severe neutropenia or life-threatening agranulocytosis [Insiripong, 2010]. The exact pathogenic mechanisms that lead to WBC alterations are not fully understood, but bone marrow suppression in dengue infection is well documented and probably has a major role in the hematologic alterations present among patients with dengue [Srichaikul and Nimmannitya, 2000].
Clozapine (CLZ) remains the most effective treatment for schizophrenia, but because of its poor side-effect profile, is generally used for patients who respond poorly to other antipsychotics [Tandon et al. 2007]. The side effects of CLZ, in particular neutropenia and agranulocytosis, continue to be a focus of concern during treatment with this antipsychotic, with an incidence of agranulocytosis of around 1% and of neutropenia of about 3%, with the highest risk within the first 6–18 weeks of treatment [Atkin et al. 1996]. Such a risk demands guarantees of safety during treatment with CLZ through close clinical followup and mandatory scheduled hematologic screening [Novartis Pharmaceuticals Canada Inc., 2010] (Table 1). The occurrence of such complications during the treatment of patients whose condition has usually failed to respond to all other pharmacological alternatives may leave their psychiatrists without viable options for an effective treatment. Therefore, it is critical to understand the relevance of WBC alterations during dengue infection in patients with schizophrenia who are taking CLZ.
Clozapine hematological monitoring and appropriate management based on CBC results [Novartis Pharmaceuticals Canada Inc., 2010].

ANC, absolute neutrophil count; WBC, white blood cell.
Materials and methods
We are addressing this concern by presenting three cases of dengue infection in CLZ-treated patients with schizophrenia (Table 2). The three patients were regularly followed in our outpatient schizophrenia clinics at the Clinic Hospital of Ribeirão Preto Medical School, in the city of Ribeirão Preto, São Paulo, Brazil. These cases were studied during the 2010 dengue epidemic in Ribeirão Preto, when around 30,000 dengue cases were identified [DATASUS, 2011]. During dengue infection, these three refractory patients with schizophrenia were admitted to our psychiatric ward, where close clinical and laboratory monitoring was implemented. The patients presented different outcomes with regard to hematological alterations, with two of them requiring CLZ suspension due to neutropenia. We describe the successful rechallenge with CLZ subsequently implemented.
Data on the three patients described in this report.
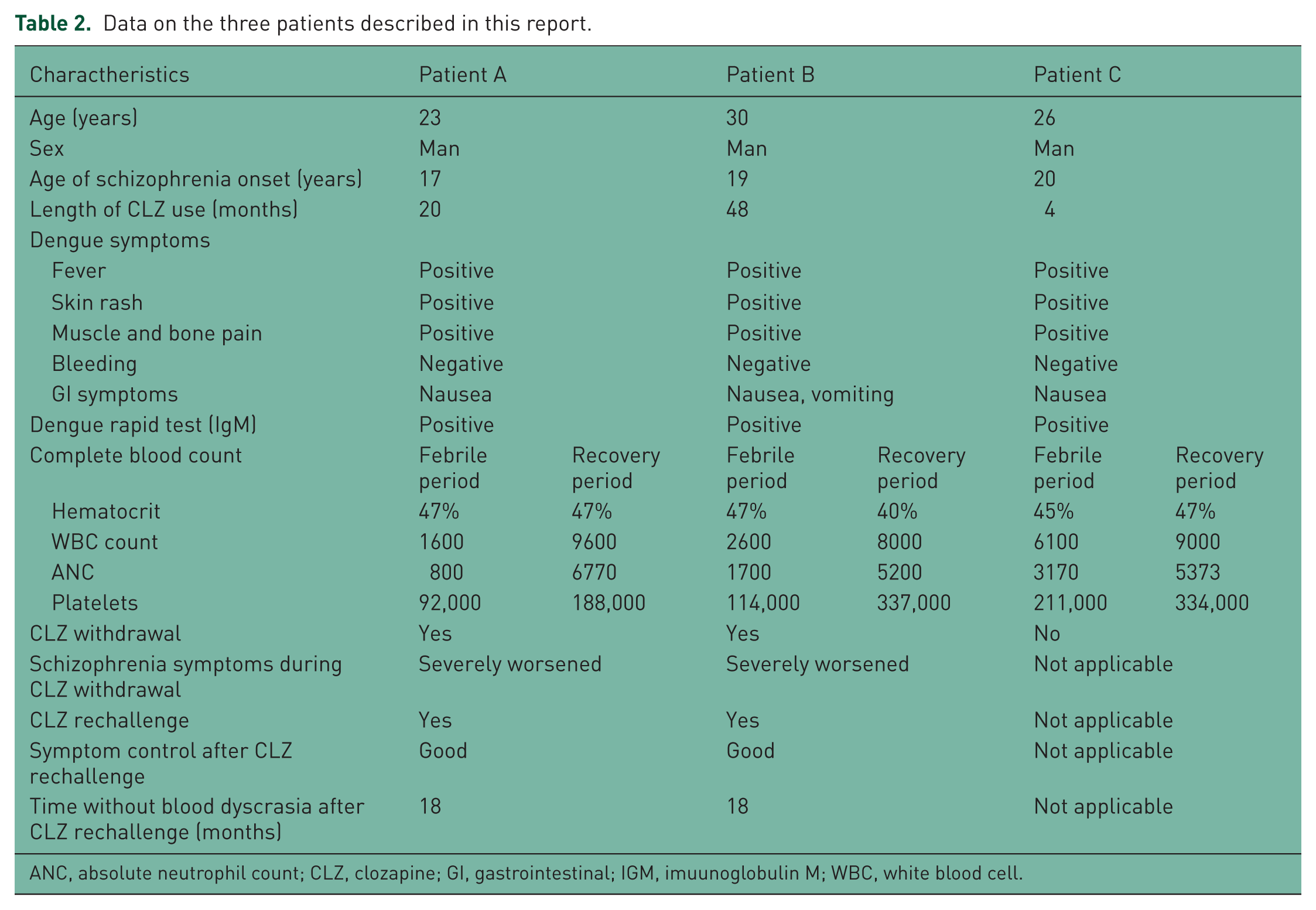
ANC, absolute neutrophil count; CLZ, clozapine; GI, gastrointestinal; IGM, imuunoglobulin M; WBC, white blood cell.
Results
Patient A
A 23-year-old white man, diagnosed with schizophrenia 6 years previously, had been treated with CLZ as a refractory patient for 20 months without major complications. After 1 month of in-house treatment using daily CLZ 500 mg and clomipramine 75 mg (to treat obsessive compulsive symptoms) and following considerable symptom improvement, the patient returned from a weekend discharge reporting 2 days of high fever, nausea, and bone and muscle pain. A physical exam revealed a body temperature (BT) of 38ºC, blood pressure (BP) of 110 × 70 mmHg, pulse rate (PR) of 90/min, no signs of dehydration and a maculopapular rash around his face and trunk. Complete blood count (CBC) during readmission showed a hematocrit (Hct) of 47%, WBC count of 1600 [absolute neutrophil count (ANC) 800 and leucocytes (L) 600], and a platelet (plt) count of 92,000. Dengue infection was suspected, and due to the symptoms, CLZ was immediately discontinued. On the third day after readmission, a dengue rapid test [Immunoglobulin M (IgM)] came back positive. Clinical improvement with regard to hematologic normalization was apparent 3 days later. However, a critical worsening of the schizophrenic psychopathology was observed, with the patient in a catatonic state most of the time and muttering during some periods of the day. Because of the previous complete lack of response to a wide variety of antipsychotics other than CLZ, before a reintroduction of any other medication, a course of electroconvulsive therapy was implemented. However, after eight sessions without improvement, the staff decided to try a rechallenge with CLZ, believing that the major cause of the hematologic alteration was the dengue infection. His WBC count had been normal during the past 50 days, so CLZ was carefully reintroduced until the previous dosage of 500 mg/day was reached after 2 months. Four months later, with that dosage of CLZ, along with sertraline 50 mg/day and lamotrigine 100 mg/day, the patient was discharged with an acceptable improvement in the psychopathology and without hematologic alterations. At 18 months after CLZ reintroduction, the patient has been treated in our outpatient clinic with the same prescription, with no need for hospital readmission; no hematologic alterations were observed.
Patient B
A 30-year-old white man, diagnosed with schizophrenia 11 years previously, had been treated as a refractory patient for 10 years, initially with CLZ during the first 5 years, with good response. However, due to syncope that was attributed to the irregular use of CLZ, this medication was discontinued and olanzapine and then quetiapine were both tried without good results, which led to the reintroduction of CLZ 4 years ago, with the patient showing acceptable symptom control without any noticeable major side effects with regular use of CLZ 500 mg/day and citalopram 20 mg/day. During one of his evaluations in our outpatient clinic, he complained of 7 days of headache and bone pain, with high fever in the last 2 days, associated with skin rash and nausea during the last 24 h. A physical exam revealed a BT of 38.5ºC, BP of 100 × 60 mmHg, PR of 80/min, no signs of dehydration and a disseminated maculopapular rash. A CBC showed a Hct of 47%, WBC count of 2600 (ANC 1700 and L 500) and a plt count of 114,000. He was rehospitalized to receive supportive care and all medications were immediately discontinued due to fever and neutropenia onset. A day 1 dengue rapid test (IgM) came back positive, confirming the suspicion of classic dengue fever. The third CBC 48 h later came back with better results, namely an Hct of 38%, a WBC count of 3700 and a plt count of 119,000. However, the patient had a worsening of gastric symptoms, presenting with continuous nausea and episodes of vomiting. At day 5, the CBC was normalized (Hct 40%, WBC count 8000 and plt count 337,000) and the physical complaints were gone, but the psychopathology was much worse, with the patient evolving into a catatonic state. Aripiprazole 15 mg/day was introduced, along with lorazepam 2 mg three times a day. There was an improvement in the symptoms after 8 days, but this was not sustained, despite increasing the aripiprazole dose to 30 mg. After 1 month, aripiprazole was substituted by ziprasidone, but after 40 days there was not an acceptable response; the patient developed catatonia associated with tremors due to the antipsychotic. Because of this poor treatment response, rechallenge with CLZ was carefully tried. Three months later, with a complete improvement of positive symptoms and no hematologic alterations, the patient was discharged on CLZ 500 mg/day, the same dosage used before dengue infection. At 18 months after CLZ reintroduction, the patient maintained the psychopathology improvement without any new hematologic alterations.
Patient C
A 26-year-old white man, diagnosed with schizophrenia 6 years previously, was treated as a refractory patient for 10 months after treatment failures with risperidone, olanzapine and ziprasidone. CLZ had been introduced 4 months earlier, and after reaching a dose of 300 mg, with partial improvement (without hallucinations, but still delusional), the patient was transferred to our day hospital to continue his treatment. Four days after he had been transferred, he complained about muscle and bone pain, headache, high fever and nausea. On the third day of symptoms, his CBC showed an Hct of 45%, a WBC count of 6100 (ANC of 3170) and a plt count of 211,000, and a rapid dengue test (IgM) came back positive. His antipsychotic continued to be offered as usual, that is, CLZ 300 mg per day. He presented progressive improvement of physical symptoms during the next 4 days. No clinical or laboratory test abnormalities were noticed at his discharge from day hospital 2 months later, at which time there had been a satisfactory psychopathological improvement.
Discussion
Despite mild leucopenia usually found among patients with dengue, severe cases are not often observed, with only one previous reported case of agranulocytosis due to dengue infection [Insiripong, 2010]. The hematological alterations in dengue infection are probably the result of bone marrow suppression with a minor contribution of blood cell destruction by the hemophagocytosis in peripheral blood. This bone marrow suppression probably results from direct infection of hemopoietic progenitor and bone marrow stroma cells; these latter cells cause release of hematodepressive cytokines, which contribute to the downregulation of hematopoiesis, acting as a protective mechanism limiting injury to bone marrow during infection [La Russa and Innis, 1995; Srichaikul and Nimmannitya, 2000].
It is postulated that the activation of metabolites of CLZ to electrophilic nitrenium ions may cause idiosyncratic neutropenia/agranulocytosis events through direct binding of these ions to neutrophils, causing cell death by oxidative stress-induced apoptosis, and finally by directly targeting the bone marrow stroma cells [Pirmohamed and Park, 1997; Husain et al. 2006; Pereira and Dean, 2006; Flanagan and Dunk, 2008]. However, the precise mechanisms of CLZ-induced leucopenia/agranulocytosis are still unclear [Guest et al. 1998; Coleman, 2001; Rajagopal, 2005]. Nevertheless, it is well recognized that the overlap of risk factors for blood dyscrasias may increase their occurrence (e.g. concomitant use of carbamazepine and CLZ, two drugs recognized to induce neutropenia). Patients on CLZ treatment are often on this drug as the last therapeutic option, providing them with a pharmacological lifeline. Any reason to discontinue CLZ treatment must be judged very carefully.
What should be considered when analyzing our reported cases, therefore, is the probable increased likelihood of blood dyscrasias among CLZ-treated patients during dengue infection, due to the occurrence of an overlap of risk for developing neutropenia. It seems plausible that the main cause of dyscrasias in these patients is the dengue infection, considering the benign characteristics of the events, with rapid normalization of CBC and tolerance to CLZ rechallenge.
Our first case described above would be classified as severe neutropenia and the second as moderate leucopenia; the last case had a WBC count within the normal range. Data about CLZ rechallenge after an episode of neutropenia due to its use show that both the risk of a new blood dyscrasia as well as its severity are higher, with a second neutropenia with CLZ generally lasting longer and more often evolving into cases of agranulocytosis [Dunk et al. 2006]. Thus, in the presence of blood dyscrasias, CLZ must be discontinued, and if the WBC count reaches less than 2000/mm3 or the ANC less than 1500/mm3, a rechallenge with this antipsychotic is contraindicated [Novartis Pharmaceuticals Canada Inc., 2010] (Table 1).
The belief that the neutropenia was not related to CLZ use but mainly linked to dengue infection contributed to our rechallenge decisions. Furthermore, the fact that these patients with refractory disease responded only to CLZ and not to the other antipsychotics reinforced our decisions to reintroduce it. These patients submitted to CLZ rechallenge have done well after 12 months of continuous use of CLZ, without any WBC count alteration. This tolerance to CLZ rechallenge appears to reinforce the hypothesis that dengue infection was the main cause of these neutropenia cases. Furthermore, the apparently higher incidence of significant blood dyscrasias during dengue infection among patients on CLZ could suggest a possible correlation between their neutropenia induction mechanisms. Future studies targeting the mechanisms involved in dengue neutropenia observed in patients taking CLZ and also having dengue fever are warranted.
To our knowledge, this is the first report of neutropenia cases among CLZ-treated patients during dengue infection that describes the withdrawal of CLZ and its successful readministration. It is very likely that during dengue epidemics many patients with schizophrenia and using CLZ have their treatment permanently discontinued given WBC count concerns, causing relapse of symptoms of schizophrenia and impairment of quality of life of these patients. Our observations could help to avoid unnecessary CLZ withdrawals in patients with refractory schizophrenia who rely on this medication to control their symptoms. Our descriptions may help clinicians to manage these particular neutropenia cases among patients on CLZ with concurrent dengue infection, a disease so prevalent and with annual outbreaks in so many regions of the world.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.