
Abstract
Introduction
Schizophrenia is a psychotic disorder characterized by a range of debilitating symptoms. Relapses in the disorder have a prolonged adverse impact on the quality of life for the patient [Briggs et al. 2008]. There are considerable economic costs associated with crisis intervention and hospital admission. Importantly, patients that receive prompt treatment have been found to recover more effectively than those that do not [Drake et al. 2000].
Known causes of psychotic relapse include nonadherence to treatment, substance misuse and life events. However, some patients relapse in the absence of these factors. Chouinard proposed that antipsychotic drugs may themselves in some cases cause relapse because their action in blocking dopamine D2 receptors can induce a compensatory state of dopamine supersensitivity resulting in a breakthrough of psychotic symptoms [Chouinard, 1990]. Clinical manifestations of dopamine supersensitivity psychosis were suggested to include the development of abnormal involuntary movements (AIMs) and tardive dyskinesia, the requirement for increasing doses to prevent breakthrough of symptoms and sensitivity to life events. In testing this idea in clinical practice, we previously reported that relapses in non-substance-misusing patients were indeed associated with prevalent tardive dyskinesia [Fallon and Dursun, 2011]. These patients compared with those without AIMs had been treated with greater doses of antipsychotic drugs, had more psychotic and depressive symptoms, experienced more minor life events, and tended to have more residual symptoms after remission. In contrast, patients relapsing without AIMs had experienced more marked life events.
In the previous study, structured interview schedules were used to collect data on life events, that is, the Life Events and Difficulties Schedule (LEDS) [Brown and Harris, 1978] and symptomatology at relapse, that is, Schedules for Clinical Assessment in Neuropsychiatry (SCAN) [WHO, 1999]. However, due to the length of these schedules, they are not easy to administer in clinical settings. Chouinard proposed diagnostic criteria for supersensitivity psychosis and these criteria and the findings of Fallon and Dursun were used to devise a diagnostic checklist of supersensitivity psychosis (see Appendix 1) [Chouinard, 1990; Fallon and Dursun, 2011]. This paper reports the use of this checklist with a group of individuals with schizophrenia or schizoaffective psychosis experiencing a relapse whilst compliant with antipsychotics. The overall objectives were: to gather a larger sample to replicate the associations of AIMs in relapses in treatment-compliant patients comparing the clinical features of supersensitivity psychosis found in this study with those of the previous study [Fallon and Dursun, 2011]; to validate the abbreviated checklist for supersensitivity psychosis, which could be integrated into clinical practice.
Supersensitivity psychosis is an important consideration for mental health professionals. Compliance with antipsychotics is often assumed to be a protective factor. However, if certain antipsychotics can increase adequately treated patients’ biological vulnerability to psychosis, this means less reliance should be placed on compliance as a protective factor. In addition, it is often assumed by clinicians that patients who relapse for no identifiable reason are noncompliant with medication when this may not be the case. Furthermore, the iatrogenic nature of the untoward effects of antipsychotics, including antipsychotic-induced dopamine supersensitivity, has led some to call for a much more cautious and selective approach towards their use. A better understanding of the extent of antipsychotic-induced supersensitivity psychosis will inform the debate on how best to use antipsychotics to treat psychosis whilst minimizing potential adverse effects [Bentall and Morrison, 2002; Whittaker 2004].
This study had five objectives: (a) in a sample of 41 patients with no obvious cause of relapse to determine whether the checklist and review of case notes could determine potential causes of relapse; (b) to determine if any exhibited features of dopamine supersensitivity; (c) to determine if this group differed clinically from the patients not experiencing supersensitivity psychosis; (d) to compare the clinical features of supersensitivity psychosis found in this study to those of the previous study [Fallon and Dursun, 2011]; (e) to use the results of this study to develop further the diagnostic criteria for supersensitivity psychosis.
Methods
Study design
The study consisted of a brief clinical interview with 41 recently relapsed individuals with a diagnosis of schizophrenia or schizoaffective psychosis and at least 2 years of treatment with antipsychotic medication. This consisted of questions about the presence of positive symptoms of psychosis in the domains of hallucinations, delusions and thought disorder, life events, compliance with antipsychotic medication and abstinence from the use of illegal drugs or significant alcohol misuse. It also assessed the presence of abnormal movements in the three main body areas, that is, facial and oral, trunk and extremities. A review of clinical records provided further clinical data at relapse and 1 year follow up. The presence or absence of AIMs was the main independent (grouping) variable and the clinical variables were the dependent variables.
Data collection
The researcher conducted semi-structured interviews using the checklist. Experience with LEDS and SCAN allowed the interview to be conducted in the style of a naturalistic conversation. Psychotic symptoms at relapse were explored in the three domains of hallucinations, delusions and thought disorder. Questions such as ‘do you ever hear voices when there is no one around’ that are commonly used in clinical practice were used to assess the presence or absence of psychotic symptoms.
Questions that concerned life events focused on events that had happened either to the participant or those close to them. They were asked questions related to the 10 LEDS domains of education, work, reproduction, housing, money/possessions, crime/legal, health, marital/partner relationships, other relationships and miscellaneous, including death. Importantly, positive as well as adverse events arising in these domains were considered to be of aetiological significance and so patients were asked to identify positive events as well. The date of relapse was established at interview and later corroborated by care co-ordinators and clinical records. This ensured that events that occurred after relapse were not included as, in the LEDS tradition, only events independent or possibly independent of illness can be of aetiological significance. Questions were asked about the 3-month period prior to relapse. For example, under the domain of money, a starting probe was ‘have you or anyone close to you had any money worries recently?’. This enabled a discussion that could then move on to debts, loans, benefits, problems paying bills, etc. This is a LEDS method but is also a common approach used by clinicians when assessing new patients. Therefore, the skills of everyday clinical interviewing are transferable to the checklist. During the interview an assessment of the presence or absence of AIMs was made.
A detailed review of each patient’s clinical notes provided information on the number of relapses in the 2 years before the study, duration of relapse, number of relapses in the following 12 months, recovery at 6 months, time to next relapse (if there was one), changes made to medication at relapse, and social and psychotherapeutic responses to relapse.
Data analysis
Data from the checklist and review of clinical notes were analysed using SPSS version 15. The group was subdivided according to whether they had abnormal movements (AIM +ve) or not (AIM -ve) and the groups were compared by background variables, life events, symptoms at relapse, treatment at relapse and outcome variables. From the previous study it was found that as well as differences due to the presence or absence of abnormal movements, there were differences in the type of life event experienced; more marked events tended to occur in those without AIMs. The larger sample in this study made it possible to control for any possible confounding effects of life events by comparing AIM +ve with AIM -ve in patients without life events.
Categorical data were analysed using nonparametric tests, cross-tabulations were performed and Fishers exact two-tailed test was used to test for group differences. Differences at the 5% level of significance were reported, one-tailed if the result was predicted from the previous study [Fallon and Dursun, 2011]. For other data, means and independent Student’s t-tests were performed to assess significance. Chlorpromazine equivalents of the patient’s current medication were calculated using estimates that have become standard [Foster, 1989; Atkins, 1997; Woods, 2003].
Inclusion criteria
Patients were selected if they had a diagnosis of schizophrenia or schizoaffective psychosis presenting with a relapse whilst compliant with high-potency antipsychotic medication. These include typical antipsychotics and atypicals with a high affinity for dopamine D2 receptors such as olanzapine and risperidone. Relapse was defined as the re-emergence or exacerbation of positive psychotic symptoms after a period of remission or very stable psychopathology as identified by the patient’s care co-ordinator and corroborated by their consultant psychiatrist. The minimum duration of symptom increase was 2 weeks for it to count as a relapse. Admission to hospital was not considered an adequate proxy for relapse as service provision now means many people remain in the community despite experiencing considerable symptomatology [Bebbington et al. 2006]. The patients were recruited through their consultant psychiatrist. The exclusion criteria were: patients that had chronic symptomatology, or insidious onsets where the dating of relapse would be impossible to pinpoint to within 1 week; first and early onset cases with less than 2 years treatment with antipsychotics; patients prescribed the low-potency D2 antagonists clozapine or quetiapine; patients prescribed the D2 partial agonist aripiprazole; the existence of organic brain disorder; patients noncompliant with, or not prescribed antipsychotics prior to relapse; those abusing illicit drugs and alcohol.
Ethical considerations
The study was conducted under the auspices of the Multi-Centre Research Ethics Committee that granted ethical approval. English was the first language of each participant and written consent was obtained from each participant.
Results
A total of 41 people were interviewed and, of these, 16 (39%) exhibited AIMs, a putative feature of dopamine supersensitivity psychosis. Two subsequently died (both AIM +ve males) so follow-up data were available on 39 individuals (Table 1). There were 20 women (mean age 45) and 21 (19 at follow up) males (mean age 46). The AIM groups did not differ in age or gender distribution but they were statistically more likely to live in a care home (p = 0.03 two-tailed).
Background variables.
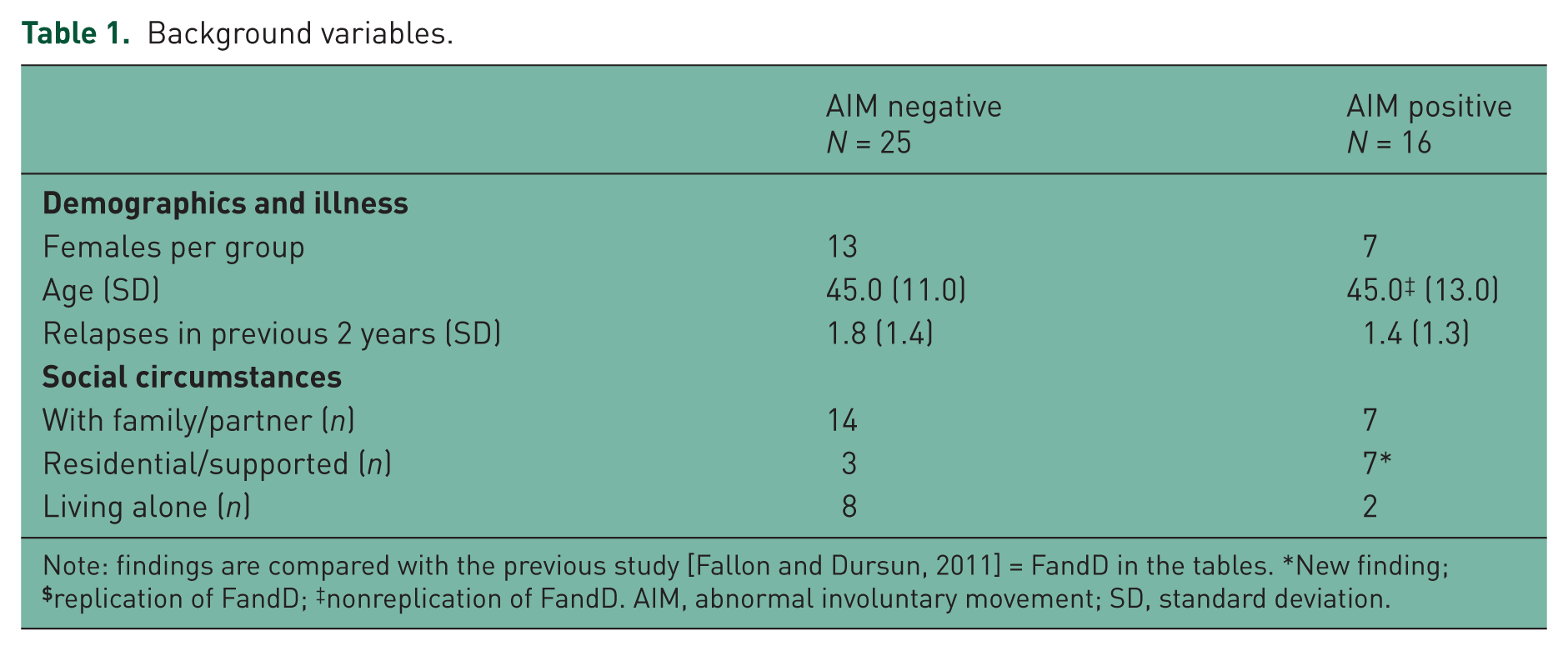
Note: findings are compared with the previous study [Fallon and Dursun, 2011] = FandD in the tables. *New finding;
Abnormal movements were not associated with the type of antipsychotic prescribed (see Table 2). The use of typical antipsychotic drugs (oral or depot) was not over-represented in those with AIMs. Indeed only one of the AIM +ve group was taking a typical oral, whereas a third of the AIM -ve group was taking oral typicals and this almost reached statistical significance (p = 0.06 two-tailed). The prevalence of anticholinergic use and the total exposure to antipsychotic drugs (chlorpromazine equivalents) was similar in the AIM +ve and AIM -ve groups.
Treatment at time of relapse.
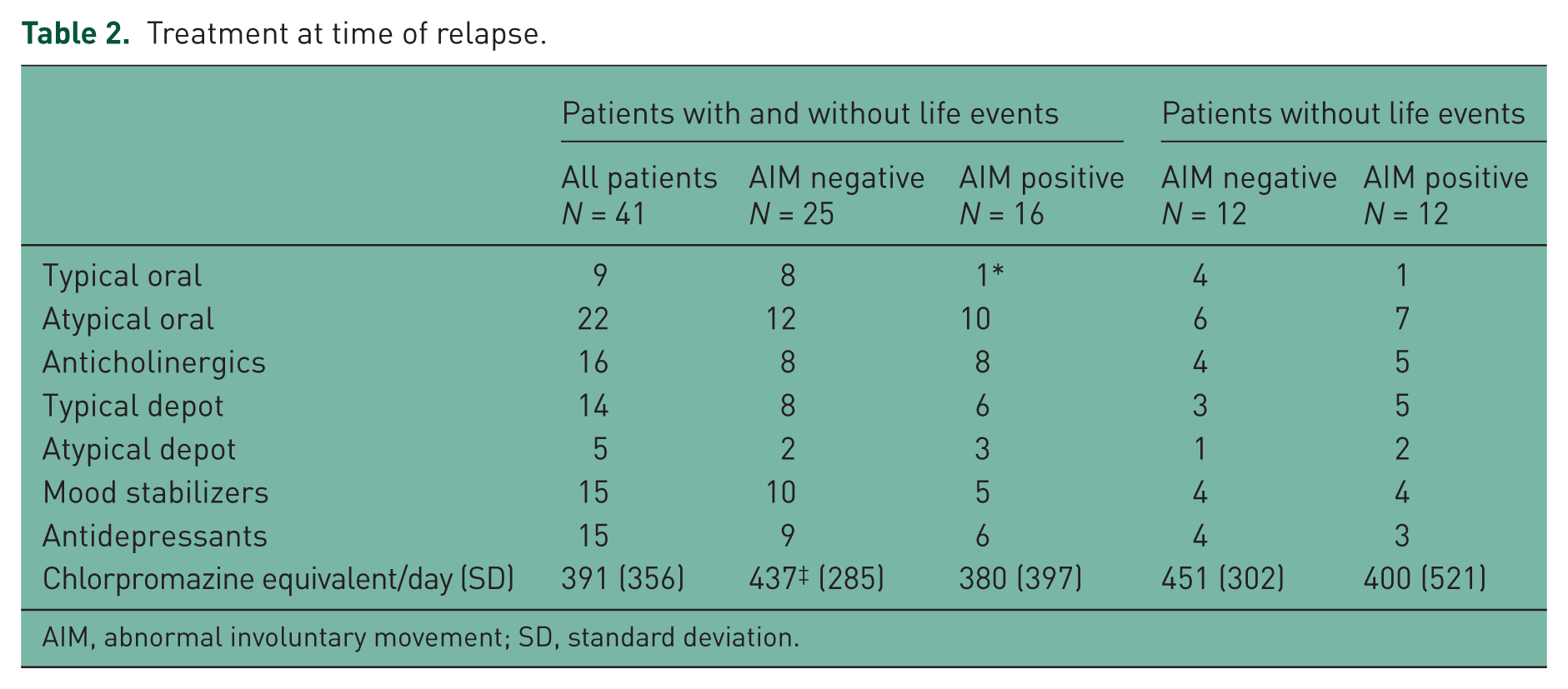
AIM, abnormal involuntary movement; SD, standard deviation.
A total of 17 patients (41.5%) reported life events that had occurred prior to relapse and 13 were AIM -ve relapsers, but this predicted difference [Fallon and Dursun, 2011] was at the trend level of significance (p = 0.08 one-tailed). Minor life events were not recorded in this study. Adding the patients with life events and/or AIM +ve, the checklist identified a cause of relapse for 29 patients (71%). An analysis was made of all patients without life events to remove this as a possible confounding variable, 12 AIM +ve, 12 AIM -ve. This confirmed the whole group findings that those with supersensitivity psychosis were highly likely to experience residual symptoms and were less likely to have made a full recovery at 6 months from relapse.
At relapse, delusions, hallucinations and thought disorder were equally distributed in the AIM groups. Although almost the entireAIM +ve group experienced hallucinations (13/16), this did not differ significantly from the AIM -ve group (14/25) (Table 3). However, the AIM +ve group was statistically more likely to experience symptoms in more than one domain (p = 0.05 two-tailed) (Table 3).
Symptoms in relation to abnormal movement.

AIM, abnormal involuntary movement.
In the treatment of relapse, the AIM +ve patients were half as likely as the AIM -ve patients to have their medication increased (p = 0.06 two-tailed) (Table 4). The groups did not differ in terms of admission, social or psychotherapeutic care.
Treatment change at relapse.
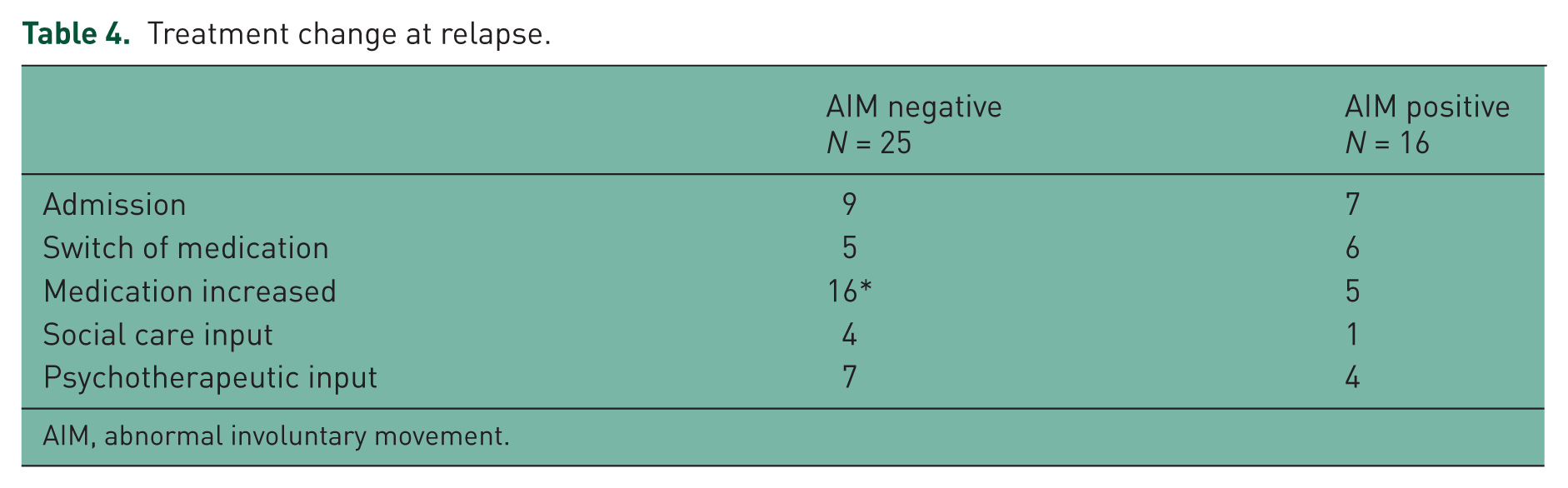
AIM, abnormal involuntary movement.
The outcome at follow up (see Table 5) revealed two statistically significant differences between the two samples. The AIM +ve patients were statistically more likely to have residual symptoms between episodes (11/14 AIM +ve versus 8/25 AIM -ve; p = 0.008 two-tailed) and make a worse recovery at 6 month follow up (3/14 had made a full recovery at 6 months compared with 18/25; 2 × 3 chi square p = 0.05). These findings remained significant when the possible confounding effects of life events were removed by comparing the AIM groups in those without life events.
Outcomes at follow up.

Discussion
This study had five aims. The first aim was to discover if the cause of psychotic relapse in 41 individuals relapsing without any obvious precipitants could be determined by using the checklist and a review of clinical records. The second was to determine whether any of the participants exhibited AIM evidence of dopamine supersensitivity. It was found that 39% (16/41) of patients met the criteria for supersensitivity psychosis, a figure comparable to the earlier study by Fallon and Dursun that found 32% met the criteria [Fallon and Dursun, 2011]. A further group of 41.5% (17/41) had an identifiable life event prior to relapse that could have been implicated in the relapse. Of these two groups only four patients had both abnormal movements and a life event. If this result (10%) was adjusted for the assessment still identified a cause of relapse for 71% of patients. Therefore, the clinical checklist was able to identify a cause of relapse for a significant proportion of the sample and specifically was able to identify the presence of supersensitivity psychosis in a significant number of them.
The group with supersensitivity psychosis differed from the rest of the sample in several respects (third aim). As well as displaying AIMs, they exhibited several other features that could reflect dopamine supersensitivity and breakthrough of symptoms. They experienced more psychotic symptoms at relapse, they were more likely to experience residual symptoms, and had worse outcomes at 6 months follow up. They were also statistically more likely to live in residential care, which may be a reflection of their greater degree of chronicity.
The fourth aim was to compare the results obtained using the checklist with a previous study that used comprehensive clinical interviews [Fallon and Dursun, 2011]. There were a number of replicated findings, such as the presence of abnormal movements, higher degrees of psychopathology especially hallucinations, a greater degree of chronicity, that were potential indicators of dopamine supersensitivity in both studies. In addition, in both studies, the AIM +ve patients were unlikely to have their medication increased. It could be that this reflects an understanding by the prescribing clinician that these individuals had noticeable side effects and reflects an attempt not to exacerbate them by increasing the dose of antipsychotic. In both studies patients with relapses associated with a life event subsequently experienced a more benign course of their illness. Previous research has also found that patients with life events prior to psychotic relapse were more likely to score zero on the AIM scale, more likely to experience complete symptom remission between episodes of illness and have less need for antipsychotic maintenance medication [Van Os et al. 1994].
In the present study, the AIM -ve patients were more likely to have their medication increased than the AIM -ve patients in the previous study, and this almost reached statistical significance (p = 0.06 two-tailed). Furthermore, the AIM +ve group were prescribed lower doses that the AIM -ve group, which was not found previously [Fallon and Dursun, 2011]. However, this may be because a significant proportion of those with abnormal movements were prescribed oral atypical antipsychotic medications. When these medications are converted to chlorpromazine equivalent doses, they are prescribed in smaller doses than were the doses of typical antipsychotics historically. For example, olanzapine 5 mg equates to 100 mg of chlorpromazine [Woods, 2003], therefore, the maximum daily dose of olanzapine currently prescribed on license in the UK (20 mg) equates to 400 mg of chlorpromazine per day.
The fifth aim was to develop the diagnostic criteria for supersensitivity psychosis and two main differences to Chouinard’s criteria were found in this study [Chouinard, 1990]. Firstly, withdrawal of medication was not present in the sample, which is unsurprising as this was a study into patients compliant with stable doses of medication. Secondly, antipsychotics were not prescribed in high doses and evidence of tolerance was not present. This can be explained by the changes in prescribing atterns as atypical antipsychotics are now the redominant form of antipsychotic prescribed.
It has been argued that the newer atypical medications are more tolerable as they produce fewer side effects [Voruganti et al. 2000]. However, in this study, patients prescribed atypical antipsychotics were as likely as patients prescribed typical antipsychotics to display AIMs, and risperidone has previously been found to induce extrapyramidal side effects comparable to haloperidol [Knable et al. 1997]. The picture was clouded slightly by two patients who were prescribed both a typical depot and an atypical oral antipsychotic. However, of the 16 patients with AIMs, 9 were prescribed an atypical antipsychotic only. For some the abnormal movements may have been a carry over from previous typical antipsychotic medication as it is well known that the side effects of tardive dyskinesia are not always reversible, but it is also possible that some patients experienced abnormal movements caused by atypical antipsychotics. This research studied antipsychotics with a high affinity for dopamine D2 receptors and it has been argued that patients exhibiting signs of dopamine supersensitivity should be switched to a lower affinity antipsychotic [Chouinard and Chouinard, 2008].
There appeared to be two distinct relapse subgroups: those whose breakthrough of psychotic symptoms was associated with life events that subsequently recovered well and those that experienced a breakthrough of psychosis associated with features of dopamine supersensitivity including AIMs. This second group were more likely to experience residual psychotic symptoms and spend shorter periods in remission between florid episodes of psychosis. They were also less likely to have experienced a life event prior to relapse.
Community clinicians including community psychiatric nurses (CPNs) aim to prevent or ameliorate the distressing symptoms of psychotic illness. This includes identifying why patients relapse in order to develop strategies for subsequent relapse prevention work. The 41 patients studied here were compliant with medication and not significant abusers of alcohol or illicit drugs, therefore, the causes of relapse were not immediately apparent. Interviews with the checklist identified adverse life events and signs of dopamine supersensitivity as causes of relapse for 71% of the patients demonstrating the utility of the checklist in helping to determine both reasons for relapse and type of relapse. For some there was no discernable cause of relapse indicating that there are reasons why patients experience a breakthrough of psychotic symptoms that remain unidentified.
Relapse is an important issue; it has been estimated that for people with schizophrenia, there is a 40% relapse rate on medication in the first year following discharge from hospital [Hogarty and Ulrich, 1998]. Therefore, identifying the causes of relapse is vital as it will have implications for the choice of treatment.
Monitoring medication compliance and efficacy are key roles for CPNs and other care co- ordinators. However, this has implications for the therapeutic relationship between patient and CPN. Marland and Sharkey state that compliance is often viewed as an outcome with those that remain well assumed to be compliant [Marland and Sharkey, 1999]. Therefore, those that do not remain well are often assumed to be noncompliant and this can lead to tension in the nurse–patient relationship. In the present study, all 41 patients stated that they were compliant with their medication, as they understood the importance of compliance to the study and there were no benefits to them from taking part in the study, the researcher had no reason to disbelieve them. Furthermore, apart from the fact that they had relapsed no care co-ordinator had identified any other compelling evidence (such as a history of noncompliance or large quantities of medications found at their home) to indicate that they were noncompliant (which would have excluded them from the study). Where there were any doubts concerning an individual’s compliance, they were excluded from the study. As dopamine supersensitivity-induced breakthrough psychosis occurs in compliant patients, CPNs and other care co-ordinators need to guard against compliance-related complacency. Furthermore, although CPNs and other community care co-ordinators are best placed to monitor for side effects due to their sustained regular contact with patients, it has been found that CPNs tend to assess for a small number of side effects, such as akathisia, and often do not assess for tardive dyskinesia and other AIMs [Bennett et al. 1995]. However, this has implications for their ability to assess for, and identify supersensitivity psychosis cases at an early stage. This indicates that there is a need for CPNs to be better trained to assess for the presence of the broad range of side effects associated with both typical and atypical antipsychotics.
A limitation of the present study is whether the checklist could be used in clinical practice. For a trained LEDS interviewer assessing for the presence of life events was not difficult, the main difference was in remembering the 10 domains and using appropriate probing questions. It could be argued that this would not be the case for most CPNs in practice. However, LEDS is primarily concerned with people in their social context and would complement the assessment skills used by mental health workers, for example, asking about increases or decreases in contact with family and friends, satisfaction with the home and local area, financial difficulties or windfalls, physical or psychological health concerns to self or close ties, relationship difficulties with partner and experiences of crime, are the type of questions that staff use frequently in routine assessments. Therefore, as with assessing for side effects, this research identified a need for community staff to be trained in some brief modified form of LEDS to aid clinical assessment.
Conclusion
This study used a checklist of diagnostic criteria for supersensitivity psychosis and found it present in 39% of relapses. The checklist demonstrated its utility by identifying a probable cause of relapse for 70% of the participants. This study found that supersensitivity psychosis occurred in antipsychotic-compliant patients. Furthermore, there was no evidence of an association with an increased tolerance to antipsychotics indicated by higher doses. It is suggested that the advent of atypical antipsychotics and changes to prescribing patterns account for the lack of an association with high doses of antipsychotics.
The iatrogenic nature of supersensitivity psychosis raises questions about the use of antipsychotic medications as they may ultimately cause adaptive changes in the brain that lead to treatment failure. Caution should be exercised before increasing doses in relapsing patients. It is suggested that further research into prescribing regimes is required, including alternative dosing strategies, switching to antipsychotics with a lower affinity for dopamine D2 receptors and augmentation with novel agents.
As the main providers of community mental healthcare, CPNs occupy a key position in monitoring and supporting people with psychosis. An awareness that relapses can occur in medication-compliant patients will inform assessments of mental health and avoid mistrust occurring in the nurse–patient relationship. Furthermore, as AIMs and life events may provoke a breakthrough of psychotic symptoms, mental health nurses need training in recognizing side effects and how to assess for life events.
Footnotes
Appendix 1 Supersensitivity psychosis checklist
This work was supported by the Department of Health UK R&D Training Fellowship (grant number RDO/33/94) to Paul Fallon.
The authors declare no conflicts of interest in preparing this article.