
Abstract
Introduction
Blockade of the dopamine D2 receptor is a key mechanism in the antipsychotic treatment of patients diagnosed with a psychotic disorder but has also been associated with emotional impairments [Artaloytia et al. 2006; Carlsson, 1988; Van Putten et al. 1981]. Evidence for a negative impact of D2 blockade on emotional experience, however, has been based mainly on results from data collected with medication-related, cross-sectional questionnaires in semi-experimental environments, lacking ecological validity. In a previous study [Lataster et al. 2010] the association between D2 receptor occupancy and experience of emotions in daily life reality was investigated using the experience sampling method (ESM), a fine-grained momentary assessment technique for collecting emotional experiences in the flow of daily life [Myin-Germeys et al. 2009; Delespaul, 1995]. Results from this study showed that occupancy of the D2 receptor, occasioned by the antipsychotics haloperidol and risperidone, was associated with impaired emotional experience [Lataster et al. 2010].
In the current experiment, the same method was used to investigate the effects of aripiprazole treatment on psychotic symptoms and emotional experience in a sample of 13 patients with schizophrenia who were switched from treatment with traditional dopamine antagonist antipsychotics to treatment with the partial dopamine agonist aripiprazole. Aripiprazole has been shown to be adequate in reducing psychotic symptoms [Kim et al. 2009] and may, because of its partial D2 agonistic properties, have preferential effects on the dopaminergic motivation and reward system compared with pure dopamine antagonist antipsychotics, possibly resulting in a different subjectively experienced side-effects profile. Indeed, despite very high levels of D2 occupancy, aripiprazole treatment has been associated with better scores on the Subjective Well-being under Neuroleptics (SWN) scale compared with traditional D2 antagonist antipsychotics [Mizrahi et al. 2009]. The current study aimed at adding ecological validity to these results by monitoring emotional experience and psychotic symptoms in daily life reality.
Method
Patients
The sample consisted of 13 patients with a diagnosis of schizophrenia, displaying insufficient therapeutic response to antipsychotic treatment. Inclusion criteria were age 18–65 years; sufficient command of the Dutch language to understand instructions and informed consent; Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) [The American Psychiatric Association, 2000] diagnosis of schizophrenia, generated with the OPCRIT computer program [Mcguffin et al. 1991]; and current use of a traditional dopamine antagonist antipsychotic. Exclusion criteria were hospitalization within 2 months prior to study entry; endocrine, cardiovascular, or brain disease; history of neuroleptic malignant syndrome; and pregnancy or lactation (women only).
The procedures followed in this study were in accordance with the ethical standards of the local institutional committee on human experimentation. After complete description of the study to the patients, signed informed consent was obtained. Stop criteria were formulated if patients requested to stop for any given reason, or the investigator or treating physician was concerned about the safety of the patient.
Study design
At study entry (T0), while continuing use of traditional dopamine antagonist medication as prescribed by their psychiatrist, patients received a digital wristwatch and a set of ESM self-assessment forms collated in a booklet for each day. Ten times a day on 6 consecutive days, the watch emitted a signal (beep) at unpredictable moments between 7:30 a.m. and 10:30 p.m. After each ‘beep’, patients were asked to stop their activity and fill out the ESM self-assessment forms previously handed out to them, collecting reports of psychopathology and emotional experience. Patients were asked to complete their reports immediately after the beep, thus minimizing memory distortions, and to record the time at which they completed the form.
After completion of the 6-day assessment, aripiprazole treatment was initialized in dosages of 15–30 mg a day, titrated against clinical response. Simultaneously, dosage of previously prescribed antipsychotic medication was gradually reduced over a 3-week period, to be discontinued altogether at the start of the fourth week of aripiprazole administration. After 5 weeks of aripiprazole treatment, patients again completed a 6-day ESM assessment (T1), while continuing aripiprazole therapy. No additional antipsychotic medication was administered during this final treatment phase.
In order to estimate whether antipsychotic dosage increased or decreased after the treatment switch to aripiprazole, all antipsychotic medication dosages were additionally recalculated into chlorpromazine equivalent terms [Woods, 2003]. Throughout the study, any change in prescribed concomitant medication was discussed with the principal investigator and registered.
Emotional experience
Emotional experience was assessed with four positive affect items and seven negative affect items rated on seven-point Likert scales [rating from not at all (=1) to very (=7)], derived from the ESM booklets as described above. Mean scores on the items ‘I feel cheerful’, ‘I feel relaxed’, ‘I feel satisfied’ and ‘Overall, I am feeling well’ (Cronbach’s alpha = 0.83) constituted the positive affect scale. The negative affect scale consisted of mean scores on the items ‘I feel insecure’, ‘[I feel lonely’, ‘I feel anxious’, ‘I feel down’, ‘I have difficulty concentrating’, ‘I feel angry’, and ‘I feel guilty’ (Cronbach’s alpha = 0.85).
Psychotic symptoms
Symptomatology was assessed with eight psychosis items, rated on seven-point Likert scales [rating from not at all (=1) to very (=7)]; ‘I feel suspicious’, ‘My thoughts are influenced by others’, ‘My thoughts can't be expressed in words’, ‘I can’t get these thoughts out of my head’, ‘I feel unreal’, ‘I hear voices’, ‘I see things that aren't really there’, ‘I’m afraid I’ll lose control’ (Cronbach’s alpha = 0.81). Symptom severity was additionally assessed with the Brief Psychiatric Rating Scale (BPRS) [Ventura et al. 1993].
Analyses
For each ESM report, the time at which patients indicated they completed the report was compared with the actual time of the beep. All reports completed more than 15 min after the signal were excluded from the analyses. Previous work has shown that reports completed after this interval are less reliable and consequently less valid [Delespaul, 1995]. For the same reason, patients with fewer than 20 valid reports at either T0 or T1 were also excluded from the analyses. T0 data from patients who dropped out of the study at T1 were not included in the analyses. All analyses, therefore, were performed on the sample that had completed both T0 and T1 assessments.
Multilevel linear regression analyses, using the XTREG procedure in STATA (Stata/Mp 10.0 for Windows © 1985–2007 StataCorp. LP), were conducted with aripiprazole treatment as an independent dichotomous variable (0 = T0 – premedication switch to aripiprazole; 1 = T1 – postmedication switch to aripiprazole), and negative affect, positive affect, and psychosis as dependent variables in three separate models, with sex and any change of concomitant medication (entered as dummies of the respective medications) added as covariates.
Results
Subjects
Sociodemographic characteristics of the sample at T0 (‘baseline’).

t-value (comparing group means; two-sided p-value presented).
Pearson’s χ2 (comparing categorical distributions between groups).
Percentages do not total 100 because of rounding.
Antipsychotic and concomitant medication use throughout the study (see text for details).

Dropout at T1 due to exacerbation of psychotic symptoms after being switched to the aripiprazole medication regime.
After 5 weeks of aripiprazole treatment, 6 of the initial 13 patients again completed a 6-day ESM assessment (T1) while continuing aripiprazole therapy. At T0 these six patients had received olanzapine (n = 3), pimozide (n = 1), haloperidol (n = 1) or quetiapine (n = 1) treatment. After recalculation of medication dosages in chlorpromazine equivalent terms, four of these patients received relatively lower dosages of an antipsychotic after the switch to aripiprazole therapy, whereas the remaining two patients received relatively higher chlorpromazine equivalent dosages after being switched to aripiprazole.
Seven patients experienced exacerbation of psychotic symptoms after they had switched to the aripiprazole medication regime, leading to discontinuation of aripiprazole treatment and dropout of the study at T1. No instance of dropout was related to patients being unable to comply with the ESM protocol. This was supported by high compliance rates at T0 for both patients who completed treatment [44 reports (73%), SD = 7.9%] and patients who dropped out [42 reports (70%), SD = 2.9%; t(df=11) = –0.68, 95% CI –9.10 to 4.81, p = 0.512). Furthermore, mean total baseline BPRS scores did not significantly differ between patients who completed treatment and those who dropped out (see Table 1).
In addition, compliance rates for patients who completed treatment at T1 were high and similar to those observed at T0 [44 reports (73%), SD = 4.8%].
Effect of switching to aripiprazole on subjectively experienced symptoms and emotions
The results are summarized in Figure 1. Multilevel linear regression analysis showed a main effect of aripiprazole treatment on psychosis [β = –0.38 (SE = 0.064), p = 0.001], with lower levels of psychotic symptoms after the start of aripiprazole treatment, supported by a significant decrease in mean total BPRS score [mean(T0) = 37.7(SD=17.2); mean(T1) = 34.2 (SD = 17.9); t(df=5) = 3.42, 95% CI 0.87 to 6.13, p = 0.019). In addition, a decrease in feelings of both positive [β = –0.26 (SE = 0.117), p = 0.027] and negative affect [β = –0.50 (SE = 0.072), p = 0.001] became apparent after the start of aripiprazole treatment. All analyses were corrected for sex and concomitant medication change.
Reduced experience of subjectively rated psychosis, and positive and negative affect after 5-weak treatment with the partial D2 agonist antipsychotic aripiprazole, compared with previous antipsychotic treatment with traditional D2 antagonistic compounds. ESM, experience sampling method.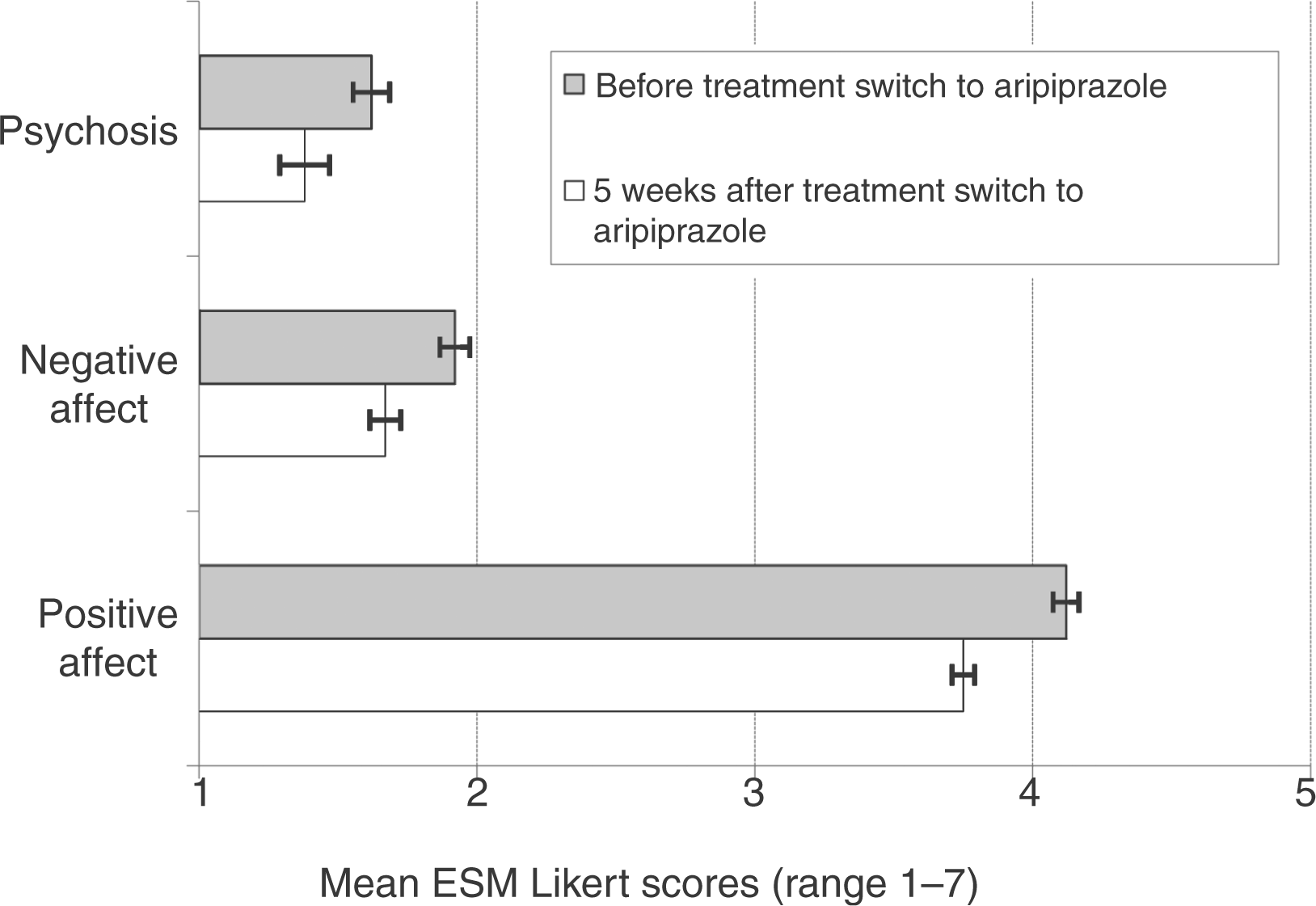
Discussion
The findings of the current study, first, indicate that switching patients with schizophrenia from treatment with traditional dopamine antagonist antipsychotics to treatment with the partial dopamine agonist aripiprazole increases risk of psychotic exacerbation, even when switching is performed gradually by tapering off previous antipsychotics over a 3-week period. More than half of the patients included in the current study experienced exacerbation of psychotic symptoms after being switched to the aripiprazole medication regime Box 1), a phenomenon that has been described in other reports [Adan-Manes and Garcia-Parajua, 2009; Pae et al. 2009; Ramaswamy et al. 2004]. As suggested by Adan-Manes and Garcia-Parajua, chronic administration of dopamine antagonists in these patients may have induced hypersensitivity to the agonistic effects of aripiprazole, resulting in a worsening of psychotic symptoms in response to aripiprazole treatment. Although it can be argued that aripiprazole dosage in the current study was well above the established clinical optimum of 10 mg/day [Sparshatt et al. 2010], clinical response to aripiprazole has not been shown to decline with increasing dosage [Mace and Taylor, 2009].
Second, the current findings suggest that, when effective in terms of reducing psychotic experiences, switching from a traditional D2 antagonist antipsychotic medication to the partial D2 agonist aripiprazole results in a decrease in both positive and negative affect, suggesting the induction of emotional dampening in the context of daily life. Previous studies have suggested that the partial dopamine agonistic properties of aripiprazole, as opposed to the dopamine antagonistic properties of other antipsychotics, have a more favorable effect on subjectively experienced side effects [Liemburg et al. 2011; Mizrahi et al. 2009; Ohlsen and Pilowsky, 2005]. These studies, however, lack ecological validity because emotional experiences were assessed retrospectively and globally using cross-sectional instruments. The current study assessed emotional states in the reality of daily life, thereby allowing examination of more subtle changes in emotional experience. Therefore, although conceptualized as a ‘dopamine system stabilizer’ [Stahl, 2001a, 2001b], the current findings of emotional dampening suggest that aripiprazole may induce behaviorally relevant inhibition of the dopamine-regulated reward system [Kapur, 2004; Berridge and Robinson, 1998]. Although it is arguable that these effects may have been purely due to an increase in D2 receptor occupancy related to administration of relatively high dosages of aripiprazole in the current study, recalculation of medication dosages in chlorpromazine-equivalent terms indicated that the majority of patients in fact received relatively lower dosages of antipsychotic when switched to aripiprazole therapy. Furthermore, as shown by Mizrahi and colleagues, the effects of aripiprazole on subjective wellbeing do not appear to be mediated by D2 receptor occupancy levels [Mizrahi et al. 2009].
It should be noted that actions at 5-HT serotonin receptor sites have been implicated in emotion regulation in depression and schizophrenia [Kranz et al. 2010; Hedlund and Sutcliffe, 2004; Meltzer, 1995] and changes in emotional experience, therefore, may have been partly influenced by changes in 5-HT receptor occupancy as a consequence of the switch to aripiprazole treatment. However, Kapur and Seeman argued that, unlike D2 receptor modulation, the mechanism of serotonin receptor antagonism is neither necessary nor sufficient in producing ‘atypical’ effects, suggesting that actions at the D2 receptor might be more closely related to emotional wellbeing [Kapur and Seeman, 2001].
It must be acknowledged that the scale and naturalistic setting of the current study, and the 54% dropout rate call for careful interpretation of the data, and replication of the findings in larger, randomized controlled studies. Nonetheless, the authors argue that implementation of the ESM in psychopharmacological research, as previously shown by Lataster and colleagues [2010], can form a novel and valuable tool for untangling the working mechanisms of compounds with regard to their impact on mental states. No instance of dropout was related to patients being unable to comply with the ESM protocol, consistent with previous studies demonstrating that ESM assessments are not restricted to small subsamples of patients with schizophrenia who are relatively asymptomatic [Lataster et al. 2010; Myin-Germeys et al. 2001; Delespaul, 1995]. The addition of established subjective side-effects questionnaires (e.g. SWN, Subjects' Response to Antipsychotics (SRA)) [Naber, 1995; Wolters et al. 2006] may help to validate subjectively experienced side effects in future pharmacological ESM studies.
Footnotes
Funding
This work was supported by an unrestricted grant of Bristol-Myers Squibb, the Netherlands.
Conflict of interest statement
Dr M. Bak has received grant/research support from Bristol-Myers Squibb. Dr M. Bak is a member of speakers/advisory boards for Eli-Lilly, Janssen-Cilag, and Bristol-Myers Squibb.