
Abstract
Clozapine is a widely used atypical antipsychotic with a unique effectiveness in treatment-resistant schizophrenia. An important adverse effect is seizures, which have been observed at all stages of clozapine treatment. Valproate has traditionally been considered the drug of choice for the prophylaxis of clozapine seizures, however it may not be the most suitable choice for all patients. There is disagreement as to the best point to prescribe valproate or a suitable antiepileptic: as seizure prophylaxis at a certain clozapine dose or level, or only as remedial treatment. In this review, we examine the relevant literature with an aim to evaluate the following relationships: clozapine dose and electroencephalogram (EEG) abnormalities, plasma levels and EEG abnormalities, dose and occurrence of seizures and plasma levels and occurrence of seizures. Weighted linear regression models were fitted to investigate these relationships. There was a strong relationship between clozapine dose and plasma level and occurrence of clozapine-induced EEG abnormalities. However, a statistically significant relationship between dose and occurrence of seizures was not found. A relationship between clozapine plasma level and occurrence of seizures was not established because of the scarcity of useful data although our review found three case reports which suggested that there is a very substantial risk of seizures with clozapine plasma levels exceeding 1300 µg/l. Seizures are more common during the initiation phase of clozapine treatment, suggesting a slow titration to target plasma levels is desirable. An antiepileptic drug should be considered when the clozapine plasma level exceeds 500 µg/l, if the EEG shows clear epileptiform discharges, if seizures, myoclonic jerks or speech difficulties occur and when there is concurrent use of epileptogenic medication. The antiepileptics of choice for the treatment and prophylaxis of clozapine-induced seizures are valproate (particularly where there is mood disturbance) and lamotrigine (where there is resistance to clozapine).
Background
Clozapine is an atypical antipsychotic agent displaying unique effectiveness in the treatment of refractory schizophrenia. Its superior efficacy over other antipsychotics [Kane, 1998] has been confirmed by numerous studies [Wahlbeck et al. 1999] and clozapine is widely used despite its broad range of adverse effects. An important adverse effect is seizures, which have been observed at all stages of treatment [Sajatovic and Meltzer, 1996]: at low doses during the titration phase and at high doses during the maintenance phase of clozapine [Pacia and Devinsky, 1994]. As many as 8% of patients taking clozapine have seizures [Wilson, 1992] and resulting fatalities have been reported [Taylor et al. 2009b; Atkinson et al. 2007].
Valproate has, in the past, been considered as the drug of choice for the prophylaxis of clozapine seizures [Devinsky and Pacia, 1994]; however, since the introduction of other antiepileptic drugs (AEDs), it might not be the best choice and it is not prescribed to every patient receiving clozapine [Atkinson et al. 2007]. There is disagreement as to when best to prescribe valproate during clozapine treatment. Suggestions have included prescribing valproate prophylactically before the occurrence of a seizure [Taner et al. 1998], remedially after the occurrence of one seizure [Haller and Binder, 1990] or remedially after two seizures [Wong and Delva, 2007; Liukkonen et al. 1992]. Some guidelines suggest using prophylactic valproate in individuals on clozapine who are prescribed clozapine at doses of 600 mg a day or more or whose clozapine plasma levels are above 500 µg/l [Taylor et al. 2009a].
In the absence of any definitive and widely accepted guidance on the prevention and treatment of clozapine-induced seizures we undertook a systematic review of the relevant literature.
Method
Searches of the databases PubMed and Embase were undertaken in June 2009 using the keywords ‘clozapine’, ‘seizure’, ‘anticonvulsant’, ‘antiepileptic’, ‘EEG’ and ‘valproate’ restricted to the English language and humans. All retrieved papers were examined for additional relevant references. Authors were contacted where necessary for additional information. We aimed to investigate and evaluate the following relationships: clozapine dose and electroencephalogram (EEG) abnormalities, plasma levels and EEG abnormalities, dose and occurrence of seizures and plasma levels and occurrence of seizures.
Data obtained were tabulated and weighted linear regression models were fitted to investigate the relationship between clozapine (mean dose and plasma level) and percentage of patients with abnormal EEG and also percentage of patients with seizures. The model was fitted using the Metareg command in Stata version 11.
Results
Electroencephalogram abnormalities
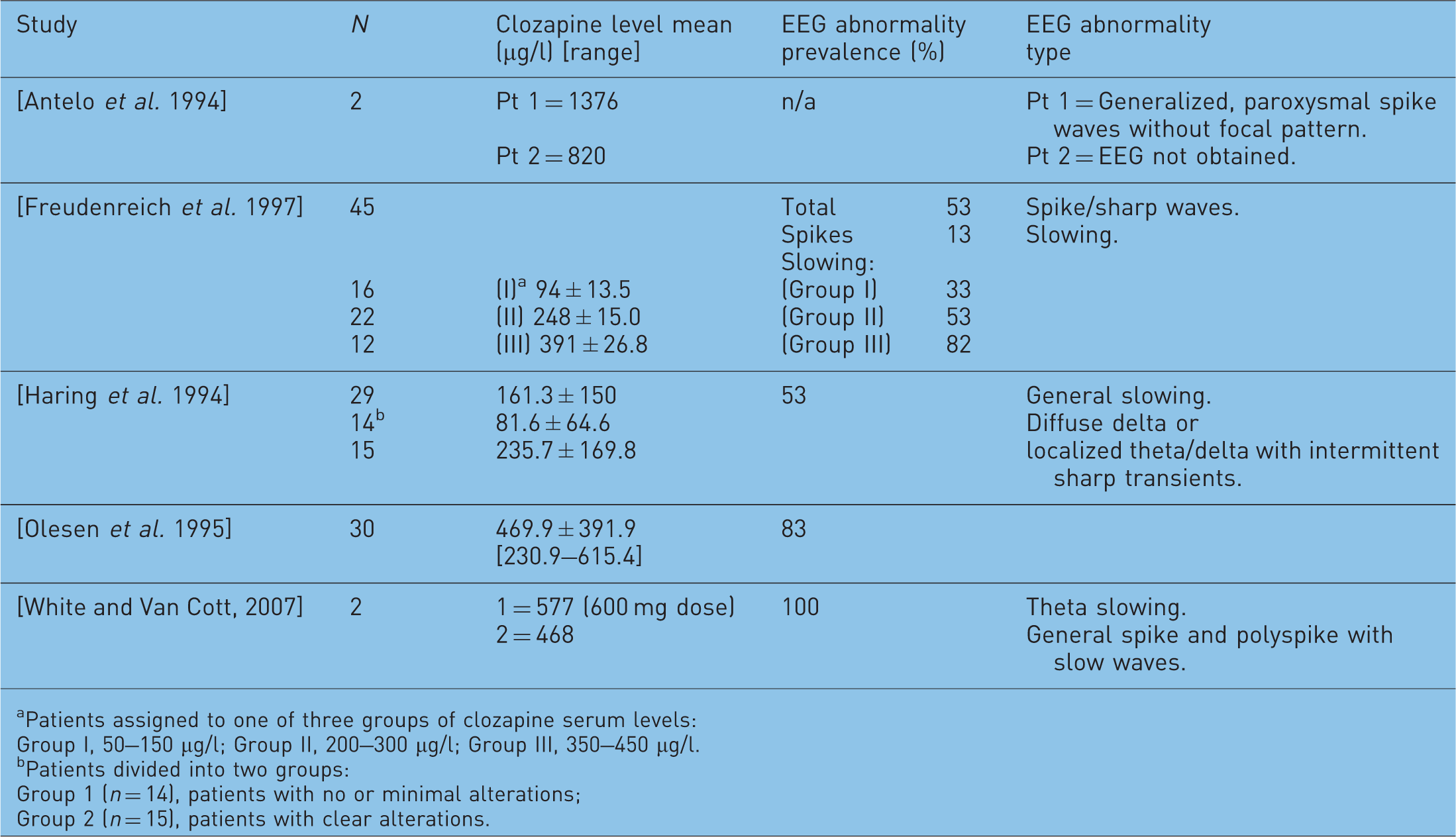
Summaries of reports on the prevalence of clozapine-associated electroencephalogram (EEG) abnormalities.


FIRDA, frontal intermittent rhythmic delta activity.
Dose range: Group I, 64–350 mg; Group II, 150–900 mg; Group III, 300–900 mg.
Patients assigned to one of three groups of clozapine serum levels:
Group I, 50–150 µg/l;
Group II, 200–300 µg/l;
Group III, 350–450 µg/l.
Patients divided into two groups:
Group 1 (n = 14), patients with no or minimal alterations;
Group 2 (n = 15), patients with clear alterations.
Epileptiform activity consisting of sharp waves, spikes, spike–wave complexes, bilateral and polyspike discharges
PDT, profound disturbance of background activity and also paroxysmal episodes consisting of delta and theta waves; EP, epileptiform activity.
Although a spectrum of EEG abnormalities was observed in association with clozapine, the most common EEG abnormality was nonspecific generalized slowing [Chung et al. 2002; Schuld et al. 2000; Freudenreich et al. 1997; Treves and Neufeld, 1996; Haring et al. 1994; Welch et al. 1994] involving delta and theta waves (slow waves). Delta is the frequency range below 4 Hz, it is normally seen in deep sleep (slow wave sleep) in adults and is not usually seen in the awake adult. Theta is the frequency range from 4 to 8 Hz and can be observed in meditation and drowsy states. Theta waves are considered abnormal if they occur in excess in the awake adult [Alarcon et al. 2009]. Spike or sharp activity was present in a relatively smaller proportion.
The effect of clozapine dose on EEG
There was strong evidence of a dose-related effect on EEG, illustrated in the graph of proportion of patients with abnormal EEG versus clozapine mean dose (see Figure 1).
Proportion of patients with abnormal electroencephalogram (EEG) versus clozapine mean dose.
Twelve studies contributed data to this weighted analysis; this enabled the size of each study to be taken into account, with larger studies carrying more weight which is proportional to the variance. One study [ Freudenreich et al. 1997 ] included results for three subsets of patients based on different dose levels; these were included as three separate data points. The study by Malow and colleagues [ Malow et al. 1994 ] was excluded, as it was unclear how they identified their 10 patients for EEG analysis from a subset of 40 patients. (All 10 patients displayed EEG abnormality.) Another study [ Silvestri et al. 1998 ] was also excluded, as the clozapine doses used or levels attained were not given. The mean clozapine dose and standard deviation were not specified in the studies by Welch and associates [ Welch et al. 1994 ] and Olesen and associates [ Olesen et al. 1995 ]. These data were calculated using the individual doses given in both studies. The spectrum of EEG abnormalities from general slowing to spike/sharp waves was grouped together. The circumference of the circle is proportional to the weight of the study in the regression model.
The regression model indicated a significant relationship between mean dose and percentage of patients with an abnormal EEG. Each 100 mg increase in mean dose was associated with an 8% increase in percentage of patients with abnormal EEG (0.08, 95% confidence interval [CI] 0.01–0.15, p = 0.022). The regression model (mean clozapine dose) explained 39% of the variance between the study results (abnormal EEG).
A number of individual studies also found a positive correlation between the spectrum of EEG changes and mean daily clozapine dose [Chung et al. 2002; Treves and Neufeld, 1996; Gunther et al. 1993]. One study [Neufeld et al. 1996] highlighted that even low-dose clozapine in psychotic Parkinsonism caused EEG changes, albeit mild ones. Another study [Freudenreich et al. 1997] reported a contrasting relationship between clozapine dose/plasma levels and EEG spikes versus clozapine dose/plasma levels and EEG slowing. Spikes were seen at doses as low as 150 mg (plasma level 100 µg/l) and the authors concluded these were not related to clozapine dose or plasma level. Similar to Gunther and coworkers [Gunther et al. 1993], they did, however, find a positive relationship between EEG slowing and clozapine dose.
The effect of clozapine plasma level on EEG
Studies investigating clozapine-induced EEG abnormalities and clozapine plasma levels are summarized in Table 2. Combining results from three studies [Freudenreich et al. 1997; Olesen et al. 1995; Haring et al. 1994], we found a positive relationship between clozapine plasma level and percentage of patients with abnormal EEG (see Figure 2). One study [Freudenreich et al. 1997] included results for three subsets of patients based on different dose levels, these were included as three separate data points. The mean clozapine level and standard deviation were not specified in the study by Olesen and associates [Olesen et al. 1995]. These data were calculated using the individual levels given in the study.
Proportion of patients with abnormal EEG versus clozapine plasma level. Summaries of reports on the prevalence of clozapine-induced electroencephalogram (EEG) abnormalities against clozapine level. Patients assigned to one of three groups of clozapine serum levels: Group I, 50–150 µg/l; Group II, 200–300 µg/l; Group III, 350–450 µg/l. Patients divided into two groups: Group 1 (n = 14), patients with no or minimal alterations; Group 2 (n = 15), patients with clear alterations.
The regression model indicated a significant relationship between clozapine level and percentage of patients with abnormal EEG. Each 100 µg/l increase in clozapine level was associated with a 12% increase in percentage of patients with abnormal EEG (0.12, 95% CI 0.03–0.21, p = 0.023).
Relationship between EEG changes and seizures
Most studies of clozapine-associated seizures have surmised that the occurrence of seizures is not necessarily predicted by changes in nonspecific EEGs [Chung et al. 2002; Treves and Neufeld, 1996; Risby et al. 1995; Haring et al. 1994; Gunther et al. 1993].For example, Antelo and coworkers [Antelo et al. 1994] reported the case of a patient experiencing myoclonic jerks and ‘leg folding’. His EEG during the event showed generalized paroxysmal spikes suggestive of seizures; however, the EEG prior to the event was normal. In contrast, an uncontrolled study of a chronically ill group of treatment-refractory psychotic patients [Welch et al. 1994] revealed that the EEG was a sensitive indicator of liability to seizures. The authors stated that seizures were more likely to occur in patients displaying EEG abnormalities with paroxysmal spike/sharp wave discharges. Conversely, two studies [Treves and Neufeld, 1996; Risby et al. 1995], reported a positive association between the occurrence of clozapine-induced EEG abnormalities and a better clinical response to clozapine [Risby et al. 1995] with a shorter duration of psychotic symptoms [Treves and Neufeld, 1996].
Clozapine-associated seizures
Occurrence of clozapine-induced seizures.

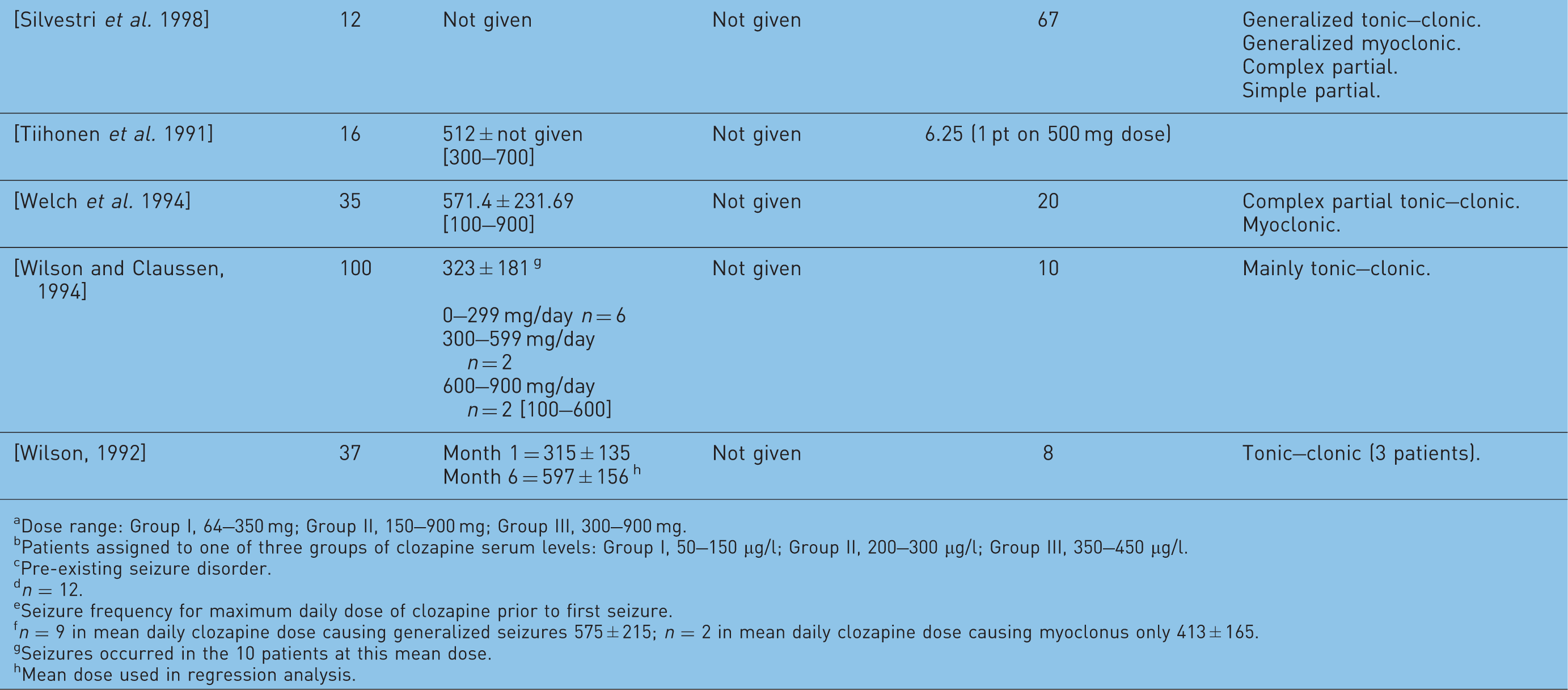
Dose range: Group I, 64–350 mg; Group II, 150–900 mg; Group III, 300–900 mg.
Patients assigned to one of three groups of clozapine serum levels: Group I, 50–150 µg/l; Group II, 200–300 µg/l; Group III, 350–450 µg/l.
Pre-existing seizure disorder.
n = 12.
Seizure frequency for maximum daily dose of clozapine prior to first seizure.
n = 9 in mean daily clozapine dose causing generalized seizures 575 ± 215; n = 2 in mean daily clozapine dose causing myoclonus only 413 ± 165.
Seizures occurred in the 10 patients at this mean dose.
Mean dose used in regression analysis.
In all studies, there was a greater risk of clozapine-induced seizures than the 1% risk associated with conventional antipsychotics [Murphy and Delanty, 2000; Balen and Procyshyn, 1999; Wilson and Claussen, 1994; Liukkonen et al. 1992; Haller and Binder, 1990]. Premarketing studies disclosed by the manufacturer reported seizure occurrence at a crude rate of 3.5% over the course of a year [Wilson and Claussen, 1994]. Devinsky and co-authors [Devinsky et al. 1991] observed the seizure incidence increasing over time, with a cumulative seizure risk of 10% after 3.8 years of clozapine therapy. A US postmarketing investigation reported generalized tonic–clonic seizures in 1.3% of clozapine-treated patients (71 out of 5629) in the first 6 months after its release. A total of 24 (34%) of these 71 patients had recurrent seizures.
The majority of clozapine-induced seizures were of the generalized tonic–clonic type [Liukkonen et al. 1992; Devinsky et al. 1991]. Clozapine may also cause myoclonus (myoclonic jerks), at times occurring alone [Antelo et al. 1994; Berman et al. 1992; Gouzoulis et al. 1991] or preceding a generalized tonic–clonic seizure. This is discussed later.
Relationship between dose and occurrence of seizures
We did not find a statistically significant relationship between mean clozapine dose and percentage of patients experiencing seizures (p = 0.353). Ten studies contributed data towards the regression analysis, illustrated in Figure 3. Patients in one study [Boachie and McGinnity, 1997] displayed a particularly high seizure incidence at doses of 200–400 mg (although these were patients with learning disability who have a higher propensity to seizures).
Proportion of patients with seizures versus mean dose of clozapine.
There was wide variation across the studies with regards to an association of clozapine dose and seizures. In the main, clozapine dose was found to be closely correlated with seizure incidence: the higher the dose; the greater the risk of seizures, even though our regression analysis did not find this to be statistically significant. The majority of case studies reported clozapine-induced seizures in patients taking doses greater than 600 mg a day [Karper et al. 1992; Baker and Conley, 1991; Haller and Binder, 1990; Simpson and Cooper, 1978]. However, a postmarketing study [Pacia and Devinsky, 1994] did not find a dose-related risk for seizures. The low-dose group had a surprisingly high frequency of seizures. This was attributed to a number of factors; seizures unrelated to clozapine therapy, a pre-existing seizure disorder, organic brain injury or a combination of epileptogenic medication [Wilson and Claussen, 1994; Devinsky et al. 1991; Haller and Binder, 1990], and initiating clozapine on a more-rapid dose titration (12 days) contrary to manufacturer recommendations of 2–3 weeks [Wilson and Claussen, 1994; Devinsky et al. 1991].
One study found most seizures occurring soon after a clozapine dose increase (mean ± SD increase = 54 ± 26 mg/day) [Wilson and Claussen, 1994], although the authors suggested this was more likely to be related to an associated rapid increase in clozapine plasma levels rather than dose per se. Similarly Haller and Binder reported an increase in seizures following large dose increments (accidental increase of 350 mg and ingestion of an additional 1200 mg as a suicide attempt). Also, seizures are reported to be more common during the initiation phase (when doses are gradually increased) [Sajatovic and Meltzer, 1996; Pacia and Devinsky, 1994; Wilson and Claussen, 1994; Devinsky et al. 1991]: Pacia and Devinsky recorded the median time to develop seizures was 42 days for the entire group, similar to Sajatovic and Meltzer who reported that half of the seizures occurred within the first 34 days of clozapine treatment.
Relationship between clozapine plasma level and occurrence of seizures
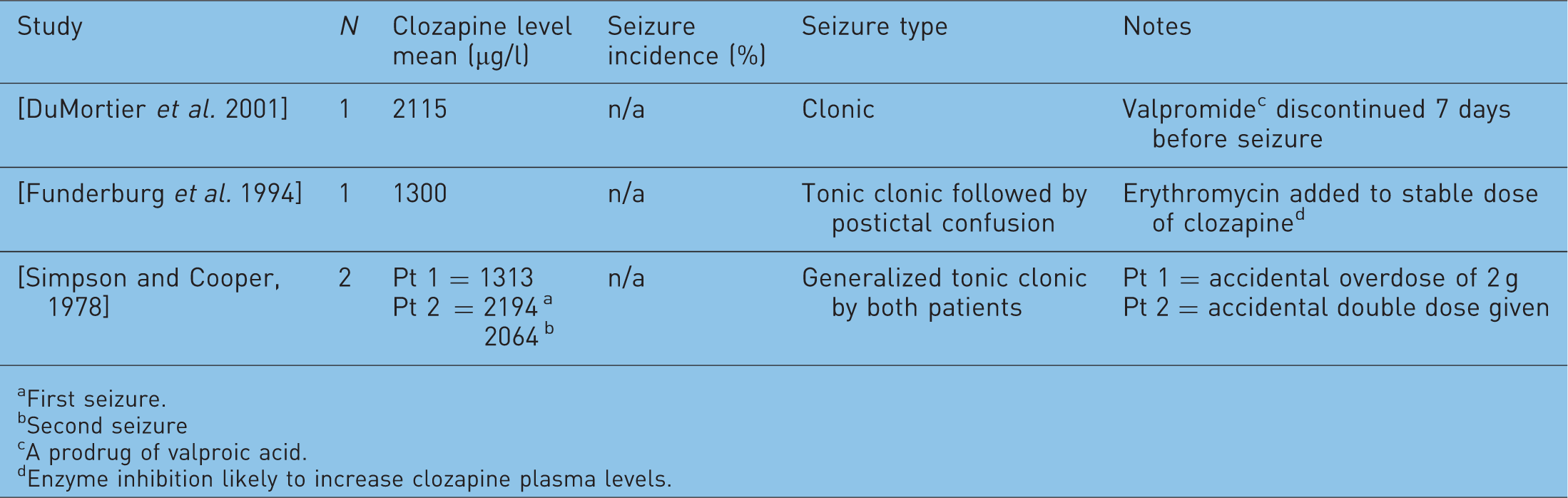
Incidence of clozapine-induced seizures against plasma levels.
First seizure.
Second seizure
A prodrug of valproic acid.
Enzyme inhibition likely to increase clozapine plasma levels.
Clozapine concentrations exceeding 1300 µg/l have been associated with an increased risk of seizures [Funderburg et al. 1994] particularly those of the tonic–clonic type. Another report [Simpson and Cooper, 1978] also found seizures occurring at levels above 1300 µg/l in two patients and proposed a safe therapeutic maximum clozapine level of 600 µg/l. Authors of all three reports emphasized the importance and usefulness of clozapine plasma level monitoring in the prevention of adverse effects related to raised concentrations.
Conversely, 3 out of 50 patients investigated by Freudenreich and associates had seizures with low clozapine levels. However, these patients had pre-existing seizure disorders, confirming the importance of obtaining a full clinical history [Freudenreich et al. 1997].
Neurotoxic adverse effects are associated with higher clozapine plasma levels and therapeutic drug monitoring has been advocated to ensure that clozapine levels are kept around the accepted therapeutic threshold. Such an approach is also likely to be valuable in assessing and monitoring the risk of clinical toxicity [Greenwood-Smith et al. 2003]; however, there is no clear, statistically significant evidence to support this suggestion.
Case reports
Clozapine-induced myoclonic seizures, myoclonic jerks, drop attacks, ‘leg folding’, stuttering and facial tics
Clozapine may cause myoclonus, at times occurring alone [Antelo et al. 1994; Berman et al. 1992; Gouzoulis et al. 1991] or preceding a generalized tonic–clonic seizure [Haddad and Sharma, 2007; Haberfellner, 2002; Sajatovic and Meltzer, 1996; Meltzer and Ranjan, 1994; Gouzoulis et al. 1993; Berman et al. 1992]. Myoclonus affects approximately 2% of clozapine-treated patients [Lieberman and Safferman, 1992]. It is a potentially serious motor phenomenon presenting as spontaneous brief jerking movements of the head, face, trunk, fingers or toes, alone or in clusters and can be epileptic or nonepileptic in nature [Sajatovic and Meltzer, 1996]. Myoclonic seizures tended to occur during the clozapine initiation phase [Taner et al. 1998] and at doses ranging between 150 mg [Haberfellner, 2002] and 500 mg [Gouzoulis et al. 1993]. Associated EEG abnormalities were observed and ranged from paroxysmal (epileptiform) patterns [Haberfellner, 2002; Gouzoulis et al. 1991] to generalized spike–wave complexes [Gouzoulis et al. 1993]. Sajatovic and Meltzer encountered an equal number of patients (2 out of 11) experiencing myoclonus alone and myoclonus followed by a generalized seizure. Thus the authors, along with others, postulated that myoclonus may be a harbinger of generalized seizures [Dhar et al. 2008; Haberfellner, 2002; Taner et al. 1998; Sajatovic and Meltzer, 1996; Antelo et al. 1994; Gouzoulis et al. 1993; Berman et al. 1992].
Three case studies reported clozapine-induced myoclonic jerks along with ‘drop attacks’ or ‘leg folding’ [Dhar et al. 2008; Antelo et al. 1994; Berman et al. 1992]. In all cases there was no loss of consciousness and the patient was well oriented to time. ‘Drop attacks’ in this context were thought to be atonic seizures, which are the result of sudden loss of muscle tone [Berman et al. 1992] or flexion tonic seizures [Antelo et al. 1994] resulting from muscle contraction rather than loss of muscle tone.
Eight cases of clozapine-induced stuttering have been reported [Hallahan et al. 2007; Lyall et al. 2007; Begum, 2005; Duggal et al. 2002; Supprian et al. 1999; Thomas et al. 1994]. These occurred at doses ranging between 125 mg [Thomas et al. 1994] and 700 mg [Supprian et al. 1999] with two authors suggesting a dose-dependent relationship [Hallahan et al. 2007; Thomas et al. 1994]. Three case reports associated clozapine-induced stuttering with seizure activity [Begum, 2005; Duggal et al. 2002; Supprian et al. 1999] and this view is supported by four cases where the use of valproate greatly improved speech difficulties [Lyall et al. 2007; Begum, 2005; Duggal et al. 2002; Supprian et al. 1999], including facial tics as reported by Begum. Three patients went on to have a generalized seizure [Hallahan et al. 2007; Duggal et al. 2002; Supprian et al. 1999].
Special cases: cigarette smoking and Asian patients
Cigarette smoking reduces clozapine plasma levels by up to 50% and higher doses may be required in smokers than in nonsmokers. Plasma level reduction may be even greater in those receiving valproate [Taylor et al. 2009a]. Tobacco smoke contains polycyclic aromatic hydrocarbons that induce liver enzymes, in particular CYP1A2 which in turn increases the metabolism of clozapine. This effect is particularly important when patients give up smoking; the enzyme activity lessens causing the clozapine plasma level to rise substantially, often requiring a reduction in dose. Nicotine replacement agents, however, have no effect on this process. Close monitoring of clozapine plasma levels is crucial, as seizures have occurred 8 weeks following smoking cessation in a clozapine responder [McCarthy, 1994]. The patient was also on fluoxetine, which can raise clozapine levels by 30–75% [Spina et al. 1998; Centorrino et al. 1994] however, the author observed seizure occurrence only after the smoking cessation.
Seizures were reported in two Asian patients on low-dose (200 mg) clozapine: in one case a male Chinese patient discontinued low-dose benzodiazepine (lorazepam), and a seizure occurred 40 hours after the last lorazepam dose [Lane et al. 1999]. The authors hypothesized that stopping the lorazepam may have unmasked the underlying seizure potential from clozapine. In the second case [Ravasia and Dickson, 1998] a tonic–clonic seizure was observed in a female Vietnamese patient whose clozapine plasma level was 1076 µg/l preseizure. Considering the lack of more familiar risk factors, the authors suggested the patient may have been a slow metabolizer of clozapine, and that race may be a risk factor for seizures on clozapine. Asians show higher plasma levels than Caucasians for a given clozapine dose [Ng et al. 2005].
A comparison of clozapine use in Korean and Caucasian patients found a greater change in the Brief Psychiatric Rating Scale (BPRS) scores in Korean patients while on significantly lower doses of clozapine [Matsuda et al. 1996]. It appears that lower maintenance doses of clozapine might be enough to treat Asian patients successfully but that seizures (which are usually associated with higher clozapine doses) might present at much lower clozapine doses.
The use of valproate for prophylaxis of clozapine-induced seizure
Valproate is an effective GABA-ergic antiepileptic drug (AED) [McElroy et al. 1989]. It has been widely regarded as the drug of choice for the treatment and prophylaxis of clozapine-induced seizures [Foster and Olajide, 2005; Iqbal et al. 2003; Miller, 2000; Littrell et al. 1995; Kando et al. 1994; Toth and Frankenburg, 1994; Liukkonen et al. 1992], and is the most commonly used AED for this indication. There are, however, very few studies prospectively examining the efficacy of valproate in preventing clozapine-related seizures.
Valproate has advantages over other AEDs: it has a broad spectrum of antiepileptic activity; it is effective in primary generalized seizures such as tonic–clonic, tonic, clonic, myoclonic (seizures and jerks) and both simple and complex absence seizures [McElroy et al. 1989]. Valproate has been used successfully in one case of clozapine-induced tonic–clonic seizure in a patient with treatment-resistant schizophrenia [Foster and Olajide, 2005]; the authors noted an improved outcome in treatment-resistant schizophrenia with the concomitant use of an antiepileptic/mood-stabilizing agent.
Clozapine-associated myoclonic seizures seem to respond well to valproate. Two cases reporting myoclonic seizures with clozapine therapy described successful treatment with valproic acid [Taner et al. 1998]. This allowed the patients to continue with their effective clozapine treatment whilst remaining seizure-free. The authors of another case report [Meltzer and Ranjan, 1994] also advocate the use of valproic acid in the treatment of clozapine-induced myoclonic jerks. Meltzer and Ranjan suggested that it may be the serotonergic receptor blocking properties of clozapine that causes myoclonus, with valproic acid displaying an antimyoclonic effect.
It is the dual effect of valproate when added to clozapine treatment that is attractive to clinicians. It acts prophylactically against seizures and also has psychotropic properties; it acts as a mood stabilizer and as an antimanic agent [Brodtkorb and Mula, 2006]. This can add greatly to the potential therapeutic benefits for the patient. A retrospective study of 55 patients examined the safety of the concurrent clozapine and valproate [Kando et al. 1994]; valproate was used as a mood stabilizer in 25 of the patients, as seizure prophylaxis in 12 patients, and as an antiepileptic in 5 patients with a history of a seizure disorder. The combination of clozapine and valproate was found to be effective and well tolerated in 87% of the patients. No seizures occurred, nor were any blood dyscrasias reported. Another advantage of valproate is that it may be less likely to cause cognitive impairment in comparison with some of the older AEDs [McElroy et al. 1989].
Common adverse effects of valproate include dyspepsia, gastric irritation, nausea, increased appetite and weight gain (8–14 kg in up to 59% of patients) [Tranulis et al. 2006]. Many of these adverse effects are additive to those caused by clozapine. In one study [Kando et al. 1994], sedation was the most common adverse effect experienced by 34 patients (62%) and led to the discontinuation of valproate in 3 patients. Other adverse effects include hair loss with curly regrowth, more rarely anaemia and blood disorders leucopenia and pancytopenia [Langosch and Trimble, 2002]. A case study also reported an apparently increased risk of agranulocytosis and neutropenia with valproate used adjunctively with clozapine [Pantelis and Adesanya, 2001]. This was reversed when the valproate was stopped.
Valproate should not normally be used in women of child-bearing age because it is an established human teratogen; neural tube defects have been associated with valproate taken during the first trimester of pregnancy [McElroy et al. 1989]. If valproate cannot be avoided, then adequate contraception should be strongly recommended and prophylactic folic acid prescribed [National Institute for Clinical Excellence, 2006].
There are conflicting reports on the effect of valproate on clozapine metabolism. Two studies found a moderate increase in the clozapine level (39%, Centorrino et al. [1994], and 20%, Facciola et al. [1999]) after at least 1 week of steady dose treatment. In contrast, a case report [Conca et al. 2000] found that the clozapine plasma level was significantly decreased, suggesting an induction of clozapine metabolism by valproate. Similarly, a small study (n = 7) [Longo and Salzman, 1995] found a 15% decrease in clozapine plasma levels after the addition of valproate. The mechanism by which valproate might induce or inhibit the metabolism of clozapine is unclear. Facciola and colleagues surmised that the interaction might involve displacement of clozapine from plasma protein binding sites. The findings described above could be explained by the coexistence of two mechanisms of interaction (enzyme inhibition and protein binding displacement) leading to opposite changes in total clozapine levels [Facciola et al. 1999]. Perhaps more important is the very significant variation in measured plasma levels of clozapine in patients receiving constant dose clozapine [Palego et al. 2002] which may lead to the opposing findings described above.
Overall, valproate does not appear to cause any clinically significant change in the steady-state plasma levels of clozapine and norclozapine.
Other antiepileptic drugs for prophylaxis of clozapine-induced seizures
It has been suggested that AEDs can be divided into two categories based on their principal psychotropic properties [Brodtkorb and Mula, 2006]; AEDs can be classified as activating drugs which exert antidepressant properties by attenuating glutamatergic neurotransmission and as sedating drugs which enhance GABA-ergic neurotransmission, e.g. valproate. Valproate may not always be suitable for use in combination with clozapine because of certain adverse effects (weight gain and sedation) and so other AEDs may be preferable, according to their adverse effect/therapeutic profile.
Lamotrigine has also successfully been used in the prophylaxis and treatment of clozapine-induced generalized tonic–clonic seizures [Muzyk et al. 2010]. These authors noted that the myoclonic jerks experienced by the patient in their case report resolved with lamotrigine therapy. It is not associated with neural tube defects [Cunnington and Tennis, 2005]. It has a limited adverse effect profile and there are few pharmacodynamic interactions. Owing to its lack of effect on hepatic enzymes, there are also few pharmacokinetic interactions [Langosch and Trimble, 2002]. However, it should be noted that lamotrigine concentrations are decreased by high oestrogen levels in pregnancy and by oestrogen-containing oral contraceptives [de Haan et al. 2004].
Lamotrigine has mood-stabilizing (preventing depressive relapse) and antidepressant properties [Brodtkorb and Mula, 2006]: an advantage when an affective component is present. A meta-analysis [Tiihonen et al. 2009] and a case series [Dursun et al. 1999] suggested lamotrigine augmentation to be an effective treatment for patients with treatment-resistant or clozapine-resistant schizophrenia. Both authors suggested that the mechanism of action was an additive relationship between lamotrigine and clozapine in reducing glutamate neurotransmission.
Topiramate is a well-documented AED which is said by some to have a good safety profile [Navarro et al. 2001]. It can be given as monotherapy or as adjunctive treatment of generalized tonic–clonic seizures or partial seizures with or without secondary generalization [British Medical Association, 2010]. It has been suggested that it may be particularly beneficial in clozapine-induced weight gain as it can induce significant weight loss, with one patient losing 21 kg over 5 months whilst successfully being treated for myoclonic jerks [Dursun and Devarajan, 2000]. It may also have mood-stabilizing properties [Brodtkorb and Mula, 2006]. Topiramate has also been suggested as an adjunctive to antipsychotic medication, however there is doubt over its effectiveness as two case reports [Hofer et al. 2003; Millson et al. 2002] noted a worsening of psychosis after the addition of topiramate.
Gabapentin is a possible alternative for patients intolerant of valproate in clozapine-induced seizure prophylaxis [Landry, 2001]. It does not affect the pharmacokinetics of clozapine, as it is not metabolized by the liver [Tranulis et al. 2006]. It is usually well tolerated when used with other medicines and has a mild adverse effect profile [Usiskin et al. 2000]. It possesses anxiolytic properties [Brodtkorb and Mula, 2006] and its use has been recommended for adjunctive treatment in anxiety [Tranulis et al. 2006] and treatment [Landry, 2001], prophylaxis [Usiskin et al. 2000] of clozapine-induced seizures. However, in one case, the addition of gabapentin to clozapine was associated with an exacerbation of psychosis [Jablonowski et al. 2002].
Carbamazepine possesses a serious adverse effect in common with clozapine: agranulocytosis [Iqbal et al. 2003]. There is also a firmly established interaction between the two drugs. Carbamazepine induces the hepatic enzymes CYP3A4 and CYP1A2. This enzyme induction accelerates the metabolism of clozapine, decreasing clozapine plasma levels [Jerling et al. 1994].
Phenytoin appears to be effective for clozapine-related tonic–clonic seizures. It is also hepatically metabolized and induces the hepatic enzyme CYP1A2, increasing the metabolism of clozapine, leading to lower clozapine levels [Lieberman and Safferman, 1992; Miller, 1991]. Phenytoin intoxication has been reported in a patient with clozapine-related seizures, after an intravenous phenytoin loading dose [Gandelman-Marton et al. 2008]. The authors suggested it was CYP2C9 inhibition by clozapine that may have caused the phenytoin intoxication. Adverse effects include thrombocytopenia, leucopenia, agranulocytosis [Toth and Frankenburg, 1994] and pancytopenia with or without bone marrow suppression [Pfizer, 2010].
Phenobarbital is also hepatically metabolized and induces the hepatic enzyme CYP1A2, stimulating the metabolism of clozapine, decreasing clozapine levels [Lieberman and Safferman, 1992].
Pregabalin is an anxiolytic antiepileptic which has shown recent promise in improving anxiety and mood in patients with schizophrenia treated with antipsychotics. Data are limited to 11 patients (5 receiving clozapine) but pregabalin might be a suitable choice of antiepileptic in those on clozapine with anxiety symptoms [Englisch et al. 2010].
Discussion
We found a relationship between both dose of clozapine and, in particular, plasma level and the proportion of patients shown to have abnormal EEG. Our analysis of published data did not, however, show a clear clozapine dose-related effect on occurrence of seizures. There were insufficient data to test the hypothesis that clozapine plasma levels are related to seizure incidence but observations in patients who stop smoking strongly suggest that it is the plasma level and not the dose that predicts seizure occurrence.
This lack of relationship between dose and seizures is somewhat to be expected, as although clozapine plasma levels are broadly related to dose, it is difficult precisely to predict plasma levels from dose alone because of the many influencing patient variables: clozapine plasma levels are lower in smokers, younger patients and in males, and higher in Asian patients. Inflammation and infection also influence plasma levels [Taylor et al. 2009a]. In addition, the fixed regression analysis we conducted was dominated by the large postmarketing naturalistic study which included 5629 patients [Pacia and Devinsky, 1994]. The mean doses used were not specified in the study and so a middle value for each dose range was assumed. This approximation greatly reduced the capacity to demonstrate a dose-related effect.
Owing to the paucity of useful data, we were unable to conduct a meta-regression analysis exploring the relationship between clozapine plasma level and occurrence of seizures. Studies examining this relationship are scarce and our review only found three case reports, which suggest only that there is very substantial risk of seizures with clozapine plasma levels exceeding 1300 µg/l.
Other limitations of our analysis include selection bias (the reporting only or mainly of cases), differences in reporting (case studies, case series, retrospective population studies, study duration), the variability between study populations, the absence of data on patient risk factors (seizure history, neurological abnormalities, smoking status, etc.), the dearth of confirmatory observations of seizure occurrence and type (some seizures were clearly reported by patients or relatives), the subsequent drop-out rates, and the previously mentioned imprecision in reporting of individual or mean doses.
Can we say when to use an antiepileptic?
Our regression model showed that seizure risk increases linearly with dose and that EEG abnormalities increase linearly with dose and plasma level and so there is no clear exponential rise in risk at any dose or level. Because results showed there was no dose or level at which risk increases at a greater rate, and as there is no safe dose or level at which seizures do not occur, we cannot make a recommendation on basis of risk of seizures except to keep the plasma level as low as possible. Dose, however, is affected by too many variables for a clear risk relationship to be established.
The plasma level for acute response to clozapine is in the range 200–504 µg/l [Taylor et al. 2009a]. In those not responding to clozapine, a plasma level target range of 350–500 µg/l has been suggested. When initiating clozapine, we suggest titrating slowly to 350 µg/l, as seizures are more common during the initiation phase [Pacia and Devinsky, 1994; Wilson and Claussen, 1994; Devinsky et al. 1991]. If there is no response, increase the dose to give a plasma level of 500 µg/l. Consideration should be given to introducing an AED if the clozapine plasma levels are above 500 µg/l, if there are clear epileptiform discharges on EEG, if the patient develops stuttering or speech difficulties, or if seizures occur. Antiepileptic therapy should also be considered at the beginning of clozapine treatment: in patients using other epileptogenic medication, patients with pre-existing seizure disorder and in patients with neurological abnormalities.
Can we say which antiepileptic should be used?
The antiepileptics of choice for the treatment and prophylaxis of clozapine-induced seizures are valproate and lamotrigine. Valproate has the most data to support its use and it is widely regarded as the drug of choice. It does not appear to cause any major changes in clozapine plasma levels, although data are contradictory. It has mood-stabilizing properties and acts as an antimanic agent, so potentially optimizing therapeutic benefit. In addition, it is effective over a broad spectrum of antiepileptic activity and it is generally well tolerated. Rare adverse effects in common with clozapine include agranulocytosis and neutropenia, and so close monitoring would be prudent. Valproate is teratogenic and is not recommended in women of child-bearing age. Baseline monitoring of liver function, full blood count, weight and height is essential, with follow ups at 6-monthly intervals (weight at 3-monthly intervals).
The clinical benefits of lamotrigine for the treatment and prophylaxis of clozapine-induced seizures are being increasingly recognized by clinicians; it possesses mood-stabilizing (at least in respect to depressive episodes) [Bowden et al. 2003] and acute antidepressant properties [Geddes et al. 2009] and has been shown to have a beneficial additive antipsychotic effect when added to clozapine therapy for schizophrenia [Tiihonen et al. 2009]. In addition, lamotrigine is not sedative and does not cause weight gain. It is a good alternative to valproate in females of child-bearing age, as it is not a major teratogen (although it may be associated with cleft palate) [Holmes et al. 2008]. A disadvantage to its use in the urgent treatment of clozapine-induced seizures is the gradual titration needed to achieve a therapeutic dose (up to 6 weeks).
Topiramate may also have a place in the treatment and prophylaxis of clozapine-induced seizures; it should perhaps be considered for those patients with significant clozapine-induced weight gain. However, the risks of worsening of psychosis should be noted. Pregabalin might be considered in patients with anxiety also requiring seizure prophylaxis.
Carbamazepine and phenytoin should be avoided in clozapine therapy due to serious adverse effects additive to those of clozapine, which could potentially lead to clozapine cessation. The manufacturers of clozapine advise against the concurrent use with carbamazepine because of the risk of bone marrow suppression. If concurrent use is unavoidable, higher clozapine doses may be required as the pharmacokinetic interaction could cause clinical deterioration in the patient. Phenobarbital is not ideal in combination with clozapine and its use should be avoided. It is a very sedative drug so the additive sedative effects could potentially be very debilitating.
Conclusion and recommendations
There is a strong relationship between clozapine dose and level and occurrence of clozapine-induced EEG abnormalities. However, a relationship between dose and occurrence of seizures was not found. We consider that clozapine level is likely to be the more reliable indicator of the potential for seizure to occur. There is a distinct lack of studies investigating the relationship between clozapine plasma levels and occurrence of seizures. Additional large-scale studies are required to establish with certainty the relationship between clozapine and seizures.
For seizure prophylaxis, there appears to be a strong argument for prescribing an AED after the occurrence of myoclonus, stuttering or speech difficulties, any type of seizure, epileptiform changes on the EEG, and in those with added risk factors such as pre-existing seizure disorder or those with relevant neurological abnormalities, and also once the clozapine plasma level reaches or exceeds 500 µg/l. The AEDs of choice appear to be valproate for a schizoaffective illness, topiramate or lamotrigine for patients with clozapine-induced weight gain, and lamotrigine in clozapine-refractory schizophrenia.
When should an antiepileptic be prescribed?
In pre-existing seizure disorder or in patients with relevant neurological abnormalities. With concurrent use of epileptogenic medication. When clozapine plasma level exceeds 500 µg/l. If stuttering or other speech difficulties occur. If myoclonic jerks occur. If EEG shows epileptiform changes. Following any type of seizure. In clozapine treatment-refractory schizophrenia, augment with lamotrigine.
Antiepileptic choice
Schizoaffective disorder or mood-related psychosis: valproate. Clozapine-induced weight gain: lamotrigine or topiramate Lack of response with clozapine: lamotrigine.
Footnotes
Acknowledgement
The authors wish to thank Victoria Cornelius for her statistical advice.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.