
Abstract
Introduction
Clozapine is the treatment of choice in patients with refractory schizophrenia with response rates of 30–60% [Meltzer et al. 1989; Kane et al. 1988]. According to the National Institute for Clinical Excellence (NICE) guidelines for the treatment of schizophrenia, clozapine should be offered to patients who have not responded adequately despite sequential use of at least two different antipsychotics [National Institute for Clinical Excellence, 2009]. Nonetheless, a substantial proportion of patients show an inadequate response to clozapine. For such patients, NICE recommends the addition of a second antipsychotic. However, evidence suggests that the addition of a second antipsychotic to clozapine results only in marginal benefits [Barbui et al. 2009; Taylor and Smith, 2009].
Furthermore, clozapine is associated with a significant burden of side effects and requires close haematological monitoring. Many clozapine-related side effects such as hypersalivation, sedation and hypotension are often benign and transient; metabolic disturbances such as weight gain, diabetes and dyslipidaemia are more significant and have long-term health implications. Other adverse effects such as agranulocytosis, myocarditis and thromboembolism may be life threatening.
There is therefore a continuing need for viable alternatives to clozapine for the treatment of patients who are wholly or partially treatment refractory as well as for patients who are poorly tolerant of clozapine. Various options have been briefly investigated in trials and in clinical practice. Despite the paucity of evidence, high-dose antipsychotics and combinations are commonly used in such patients [Paton et al. 2008].
Melperone is a butyrophenone antipsychotic licensed as Buronil in many countries in Europe but not in the UK. It has antagonist activity at D2 and 5HT2A receptors and fulfils criteria for atypical antipsychotic drugs with its low rate of extrapyramidal side effects and tardive dyskinesia [Bjerkenstedt et al. 1979]. In addition, the ratio of dopamine D4/D2 occupancy for melperone has been shown to resemble the binding profile of clozapine [Lahti et al. 1993]. Melperone has been investigated in an open trial for the treatment of patients with refractory schizophrenia [Meltzer et al. 2001] and shown to significantly improve overall psychiatric status as measured by the Global Assessment Scale (GAS) [Endicott et al. 1976] although it did not significantly affect the Brief Psychiatric Rating Scale (BPRS) scores [Overall and Gorham, 1962].
There is very little clinical experience of the use of melperone in the UK as it is currently unlicensed. Recently, there has been interest in melperone as a possible alternative to clozapine. This retrospective case series examines the outcomes for patients with refractory schizophrenia treated with melperone at the South London and Maudsley NHS Foundation Trust where it was first used in the UK.
The South London and Maudsley NHS Foundation Trust provides a range of mental health and substance misuse services in the UK. It provides care and treatment for a local population of 1.1 million people in South London. In addition, there are specialist services for people from across the country. The National Psychosis Unit is one of such tertiary referral services for the treatment of patients with refractory schizophrenia and melperone was first used here in the UK in 2005. This is thus the first published evidence of the experience with melperone in the UK.
Method
Using the pharmacy database, we identified all patients prescribed melperone from April 2005 to July 2010. From patient medical notes we extracted relevant information on past antipsychotic treatments and reasons for prescribing of melperone. For patients treated and discharged from the National Psychosis Unit, we contacted the care team to find out what the current antipsychotic treatment was. The main outcome was to determine proportion of patients discharged on melperone: a proxy for acceptable treatment outcome.
Results
Patient characteristics: summary.

Patient characteristics and outcome.

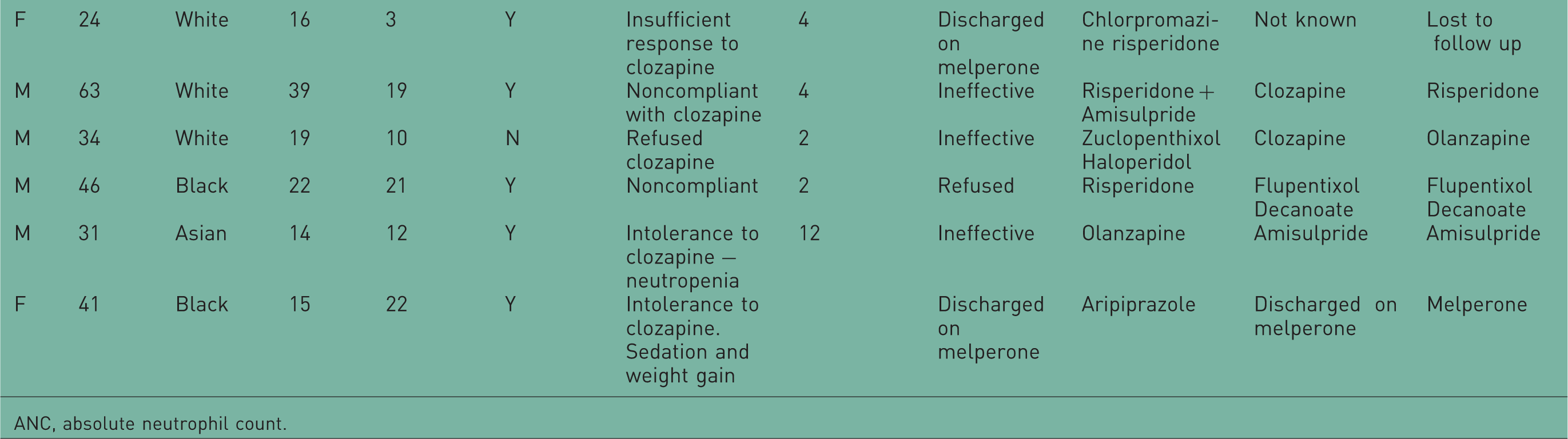
ANC, absolute neutrophil count.
This sample comprised patients with severe and treatment-refractory illness. The average age of onset of illness was 19 years of age. Almost all patients (18/21, 86%) had a prior exposure to clozapine. Of these, 10 patients had discontinued it because of adverse effects, 6 because of noncompliance with medication or blood tests and 2 patients because of inadequate response. Three patients had no prior exposure to clozapine. In two patients, this was because they had low baseline neutrophil counts and so they were ineligible for clozapine treatment. The third patient had not been exposed to clozapine because of a refusal to comply.
Duration of treatment
Three (14%) patients were discharged on melperone and 18 patients discontinued treatment during their stay on the unit. Of those who stopped treatment, the mean duration of treatment was 5.4 months. Of the three patients who were discharged on melperone, one was lost to follow up while two continued to take melperone at follow up, one for 4 years 11 months and the other for 4 years.
Reason for discontinuation of treatment
The primary reason for discontinuation of melperone was lack of efficacy in 13/18 (72%) of patients. Four patients were poorly compliant and so melperone was stopped. In the remaining patient adverse effects were the main reason for discontinuation.
Tolerability of melperone
Melperone was reasonably well tolerated. One patient was discontinued due to ECG changes with a QTc interval of 498 ms. This patient also had akathisia. Another patient experienced extrapyramidal side effects at a dose of 300 mg daily. One patient refused to continue melperone due to gastrointestinal disturbance, eye pain and insomnia. No other serious adverse effects such as seizures or blood dyscrasias were reported.
Dose of melperone
Dose was in the range of 225–600 mg daily for all but one patient who was treated on a dose of 900 mg daily.
Discussion
Although the data on the efficacy of melperone in treatment-resistant schizophrenia are rather limited, it was initially perceived in our unit as ‘clozapine without blood tests’ and an option particularly for refractory patients who refused clozapine or those who were intolerant to the various adverse effects observed with clozapine.
The sample treated comprised a cohort of patients with severe refractory psychotic disorders, with a relatively early onset of psychotic illness and mean duration of antipsychotic treatment of 13 years. The majority of patients had been previously treated on clozapine, hence there is some selection bias although it is noteworthy that of the sample who discontinued melperone, more than half were subsequently re-exposed to clozapine with therapeutic benefits. This is in contrast to the findings by Meltzer and colleagues who found that nonresponders to melperone generally did not respond to clozapine treatment [Meltzer et al. 2001].
Of 21 patients treated, only three patients (14%) were discharged on melperone (the primary outcome measure). One patient was lost to follow up and two patients remain clinically stable on long-term treatment. Of these, one patient has a diagnosis of schizoaffective disorder, depressive type. She had remained well on clozapine for 2 years but discontinued due to weight gain and sedation and suffered a relapse of her illness. She was tried on other medications without success and refused to go back on clozapine, hence the trial of melperone. She remains on melperone treatment in addition to sodium valproate, mirtazapine and venlafaxine in the community. The second patient on long-term treatment with melperone has a diagnosis of severe depressive episodes with psychotic symptoms. She was previously treated on clozapine but developed myocarditis. She failed to respond to other antipsychotic and antidepressant combinations as well as to ECT treatment. She is currently in a rehabilitation unit on treatment with melperone in combination with lithium, lamotrigine and mirtazapine.
Limitations
This is a rather small retrospective case notes review including only 21 patients. There may be bias in the sample population as more than half (13/21) the patients were treated in a tertiary referral centre and most had previous exposure to clozapine. There were no formal clinical assessments or ratings of psychopathology nor systematic evaluation of melperone tolerability and adverse effects.
Conclusions
This is the first attempt to evaluate the efficacy of melperone in the treatment of refractory psychotic illness in a naturalistic setting. Although it may be a worthwhile option in a very few patients, our results indicate a low overall success rate with melperone in patients with treatment refractory psychotic illness. Melperone should probably not be seen as an alternative for patients for whom clozapine is not suitable. Routine ECG monitoring should be considered at doses greater than 300 mg daily.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None declared.