
Abstract
Mindfulness interventions have gained empirical support for treating anxiety. This study investigated the benefit of adding anxiety-specific practice to a mindfulness intervention for anxiety symptoms in young adults. A pre-post design was used with 117 undergraduate students to compare three interventions: a mindfulness intervention with anxiety-specific practice, a conventional mindfulness control, and an audiobook control intervention. Participants completed self-report scales of social anxiety, agoraphobia, interoceptive fear, worry, and trait mindfulness at baseline and post-intervention. Results indicated that compared to audiobook control, the mindfulness group with anxiety-specific practice reported less post-intervention social anxiety. Furthermore, albeit only at high baseline symptom levels, the mindfulness group with anxiety-specific practice reported less post-intervention agoraphobia and interoceptive fear compared to the audiobook group, and the conventional mindfulness group reported less post-intervention agoraphobia compared to the audiobook group. There were no group differences on worry or mindfulness. No convincing evidence was found that the mindfulness intervention with anxiety-specific practice had an advantage compared to the conventional mindfulness intervention. Possible mechanisms for observed effects include exposure and mindfulness-related processes. Considerations for future research include using samples with elevated anxiety. More research is needed to interpret these results with more confidence.
Anxiety disorders are among the most prevalent mental health disorders and substantially impact the quality of life and functioning of those affected (Kessler et al., 2005; Lochner et al., 2003). The first-line therapeutic intervention for anxiety disorders is Cognitive-Behavioral Therapy (CBT), which has the most extensive evidence base supporting its efficacy (e.g., Hofmann et al., 2012; National Institute for Health and Care Excellence (NICE, 2019)). However, the effective treatment of anxiety and concomitant reduction of the societal and individual burden associated with anxiety disorders is hampered by a few important factors: up to 35% of patients who complete treatment do not benefit sufficiently from these first-line interventions (Taylor et al., 2012). Moreover, therapy is not easily accessible, with less than 50% of patients with mental health problems receiving adequate treatment (Lattie et al., 2024). To address these drawbacks, a number of research avenues have developed, which, among others, focus on modifying existing treatment approaches, developing new treatments, and developing preventative approaches (e.g., Lattie et al., 2024; Sampson et al., 2023). Among newer promising treatment approaches in the treatment for anxiety are mindfulness interventions.
Anxiety is characterized by adverse cognitive, emotional, and behavioral responses in anticipation of potential threat (Barlow, 2002; Grupe & Nitschke, 2013). To the extent that it can prepare the individual for the occurrence of a real threat, anxiety can be adaptive (Grupe & Nitschke, 2013). However, anxiety becomes maladaptive when the anxious response is disproportionate to the actual probability or impact of a given threat (Grupe & Nitschke, 2013) and results in excessive behavioral and cognitive avoidance of anxiety-inducing situations (Panayiotou et al., 2014), which in turn contributes to functional impairment by interfering with daily life and goals (Arnaudova et al., 2017). Furthermore, both behavioral and cognitive avoidance prevent obtaining information that may contradict beliefs about the probability or impact of a given threat, thereby contributing to the maintenance of symptoms (Craske et al., 1990; Spinhoven et al., 2017). Therefore, the reduction of avoidance is one important treatment target in the treatment of anxiety (Curtiss et al., 2021).
The concept of mindfulness has attracted great research interest in recent decades and has emerged as a promising practice for therapies for anxiety. Mindfulness practices have long been followed to counteract human suffering across a number of contemplative traditions, including Stoicism and Buddhism (Hadot, 1995; Teasdale & Chaskalson, 2011). Mindfulness has been defined as involving two components: (i) awareness of moment-to-moment experience and (ii) orienting to this experience with an accepting stance (Bishop et al., 2004; Kabat-Zinn, 2015). Turning attention to the present moment could facilitate attention being directed away from the potential for future harm, and strengthening an accepting stance could lead to reduced avoidance of unpleasant experience (Roemer & Orsillo, 2002). Indeed, acceptance has been conceptualized as antithetical to experiential avoidance (Hayes et al., 1996). Concomitantly, this should lead to reduced reactivity towards aversive experiences (Bishop et al., 2004). Thus, acceptance-based approaches such as mindfulness interventions may be well-suited to the treatment of anxiety disorders, which are associated with extensive avoidance of unwanted emotions (Bishop et al., 2004).
Indeed, research has shown that mindfulness interventions are effective for treating anxiety in healthy (e.g., Cavanagh et al., 2018) as well as clinical samples (Abreu Costa et al., 2018). The most well-known and studied mindfulness interventions are Mindfulness-Based Cognitive Therapy (MBCT) and Mindfulness-Based Stress Reduction (MBSR). Effects of these interventions have been shown to be comparable to other evidence-based interventions such as Cognitive-Behavioral Therapy, yielding mostly moderate effect sizes (Fumero et al., 2020; Goldberg et al., 2018). However, a multitude of mindfulness interventions have since emerged and have been studied targeting different populations (e.g., non-clinical, students), with varying intervention durations (e.g. brief interventions), and varying delivery modes (e.g., online or audio-based deliveries). For instance, interventions as short as 5 weeks in duration have been shown to reduce anxiety in both treatment-seeking samples (Burgess et al., 2021) and samples presenting with sub-clinical anxiety symptoms (Diplock et al., 2024). Brief interventions have been defined as interventions that last up to 4 weeks and involve practicing mindfulness for no more than 30 min per session and up to 100 min per week (Howarth et al., 2019). Available evidence suggests that such brief interventions can have a significant positive impact (Howarth et al., 2019), even when delivered online and audio-guided (e.g., Cavanagh et al., 2018; González-García et al., 2021). For instance, an online audio-based intervention lasting 2 weeks with daily mindfulness sessions lasting only 10 min resulted in significantly reduced anxiety symptom levels in a healthy student sample (Cavanagh et al., 2018). These findings are promising, as such adaptations could be helpful in the development of easily accessible and cost-effective interventions.
Mindfulness interventions have thus demonstrated efficacy in alleviating anxiety symptoms. However, existing treatments such as MBSR or MBCT typically focus on general mindfulness practices without targeting specific anxiety-related symptoms directly (Santorelli et al., 2017; Segal et al., 2018). This omission may limit the effectiveness of such interventions, particularly for individuals with heightened reactivity to anxiety triggers. 1 Addressing the symptom directly should have stronger effects than addressing it indirectly through a more general approach: just as explicitly training for a specific sport should lead to greater improvements in that sport compared to training for general fitness, so too could applying mindfulness directly to anxiety be argued to be more helpful for anxiety symptoms compared to training mindfulness in a general way. . Although interventions such as MBCT may informally involve symptom-focused mindfulness practices, to our knowledge, previous research has not formally examined the benefit of systematically focusing on anxiety as an explicit target of mindfulness training. There is some evidence to suggest that MBCT is superior to MBSR in the treatment of anxiety (Haller et al., 2021). This may be due to the cognitive-behavioral elements of MBCT; that is, a greater focus on psychological symptoms and inclusion of treatment elements such as psychoeducation and cognitive restructuring (Segal et al., 2018). Moreover, a study found that individuals with panic disorder who participated in a brief acceptance intervention to cope with a CO2 challenge (i.e., 15 min of breathing CO2-enriched air designed to produce aversive physical sensations associated with panic attacks) reported less anxiety and less avoidance of the challenge, compared to a control group that did not receive an acceptance intervention (Levitt et al., 2004). Although Levitt et al. did not compare acceptance of anxiety versus a general acceptance intervention, these findings support the idea that targeted practice may have beneficial effects. It may be that repeated practice of explicitly targeting anxiety in formal meditation increases the ability to use mindfulness as a coping mechanism for anxiety in daily life. Such symptom-specific practice is already used in mindfulness interventions of other disorders, such as depression in MBCT (Segal et al., 2018), emotions associated with food intake in eating disorders (Kristeller & Hallett, 1999), and cravings in substance use (Bowen et al., 2014; Brewer et al., 2011). Although to our knowledge there is a dearth of experimental investigations into the potential benefit of adding symptom-specific practice, engagement in these targeted exercises has been correlated with positive treatment outcomes (Brewer et al., 2011; Kristeller & Hallett, 1999). Based on these findings, we hypothesize that anxiety-specific mindfulness practices could help alleviate anxiety in the context of a mindfulness intervention.
While mindfulness interventions have shown some efficacy for the treatment of anxiety, to our knowledge no studies to date have examined whether adding explicit anxiety-targeted practice enhances outcomes in a non-clinical population. The present study aims to address this gap by testing whether adding anxiety-specific practice enhances the effect of mindfulness meditation on symptoms of anxiety disorders from an experimental psychopathology perspective. Experimental psychopathology encompasses experimental research that focuses on increasing knowledge of etiological and maintaining factors of psychopathology as well as mechanisms and active ingredients of interventions (Waters et al., 2017). We aimed to test the principle that adding anxiety-specific practice in a healthy sample of participants would lead to greater reductions of anxiety symptoms compared to control and a general brief mindfulness intervention. A student sample lends itself well to this proof-of-principle study, as the prevalence of anxiety symptoms is high in student populations (Chung et al., 2021) and as using easily accessible analog samples is a common method in experimental psychopathology research, assuming that anxiety symptoms in a student population represent the lower end of anxiety symptom severity (Zvolensky et al., 2001). We used a pre-post control group design to compare three intervention arms: one brief audio-guided mindfulness intervention consisting of conventional mindfulness practice (mindfulness-conventional), one brief audio-guided mindfulness-intervention consisting of elements of conventional practice and anxiety-specific practice (mindfulness-anxiety), and an audiobook control intervention, which were completed during a lab session and for 12 days at home. We hypothesized that (H1) post-intervention scores on anxiety and worry symptoms would differ between groups when controlling for baseline symptom scores, with the lowest levels of symptoms expected for the mindfulness-anxiety group, followed by the mindfulness-conventional group, with the control group having the highest levels of symptoms. As a secondary hypothesis (H2), we expected scores on a measure of trait mindfulness to differ between groups when controlling for baseline scores, with the lowest levels of trait mindfulness expected for the control group, followed by the mindfulness-conventional group, and the mindfulness-anxiety group having the highest scores. This is based on the rationale that practicing mindfulness in the context of difficult emotions may help respond mindfully in everyday life, which also includes situations that are characterized by difficult emotions. The applied practice to memories of everyday experience may facilitate the transfer to applying mindfulness to other somewhat difficult experiences in daily life, facilitating an increase in trait mindfulness.
Method
The study was approved by the ethics committee of the faculty of behavioral and social sciences. Participants gave written informed consent prior to inclusion in the study.
Participants
Participants that were recruited were 148 first-year students from both English- and Dutch-language tracks of a psychology undergraduate program (79.7% Female, Mage = 19.88, SDage = 1.838). Based on an a priori power analysis for ANCOVA F-tests (Fixed effects, main effects, and interactions) conducted in G*Power (version 3.1.9.4), the required minimum sample size to detect medium sized effects (f = .25) with a power of 80% at an alpha level of .05 is 158. This was the goal of the current study. However, due to time constraints on data collection, this number was not reached. Participants participated in the study to fulfill course requirements. Specifically, the requirement was that every student was asked to choose a number of studies to participate in over the course of the academic year out of a pool of many available studies in exchange for a certain amount of study credit points. There are drawbacks to this method, as it could be argued that participants were extrinsically motivated to participate in the study. However, as they could choose among many studies, we hope to have reduced this possible source of bias sufficiently. The study advertisement was titled “stress management study” and students self-selected to participate. Of course, this title could also be a source of bias. However, this should be balanced across conditions through the use of a strong control condition. The majority of the participants were German (53.4%) or Dutch (20.9%), with the remaining 25.7% indicating diverse nationalities.
For the main analysis, treatment completers (defined as having completed >50% of the intervention; cf. Gluck & Maercker, 2011; see Winter, Russell, Ugalde, White, & Livingston for information on commonly used adherence cutoffs) were included. Thirty-one participants were excluded because they indicated completing less than half of the daily sessions (control condition = 9; mindfulness-conventional = 12; mindfulness-anxiety = 10; 67.7% Female, Mage = 19.77). No other exclusion criteria were applied. The final sample thus consisted of 117 participants (82.9 % Female, Mage = 19.91, SDage = 1.918), of which 40 were in the control group, 38 in the mindfulness-conventional group, and 39 in the mindfulness-anxiety group. There was thus an overrepresentation of females in this sample which could limit generalizability of findings.
Procedure
Participation in the study involved coming to the lab on two occasions and completing an intervention for 10 minutes/day on 12 consecutive days in between the sessions. Participants were run in groups of one to four and worked at private workstations. During the first session, participants provided informed consent and completed demographics and individual difference questionnaires. Participants were allocated to private workstations based on order of arrival and then completed the audio-guided intervention exercise for a first time in the lab. Participants were allocated using a quasi-random approach for feasibility reasons: There were multiple private workstations in one room and this method of allocation made it easier for experimenters to keep the study running smoothly with multiple participants in a room at the same time. Specifically, tasks and links could be opened prior to arrival and participants could then be seated according to order of arrival to cause the least possible amount of disturbance if other participants arrived a few minutes later. Assignment was not blind, as experimenters knew which condition was assigned to which workstation. However, this knowledge did not affect assignment to condition and thus should not have an impact on the validity of the data. Following the first session, participants received a daily email containing a link to the intervention, followed by five questions about stress, relaxation, acting with awareness, non-judging and non-reactivity following each exercise. On day 6, participants received an additional short survey during which they completed the Five Facet Mindfulness Questionnaire (FFMQ; Baer et al., 2006) and a question pertaining to frequency of doing the intervention exercise during the first 6 days, emphasizing the need for honesty and that there would be no penalty for lack of adherence. During the second lab session, all questionnaires were again completed, including an equivalent question pertaining to adherence during the latter 6 days of doing the intervention exercise (“We are interested to know how often participants practice the stress management exercises. Please indicate how many of the 6 days you have practiced the exercises over the past week. Again, please be honest – there will be no penalty if you have not practiced all of the days or even if you have not practiced at all. Your honest reply will help us to better understand what sorts of stress management exercises are interesting for students to practice”).
Interventions
Audiotapes for all conditions were recorded by author BDO, a clinical psychologist trained to teach Mindfulness-Based Stress Reduction (MBSR) with over 15 years of MBSR teaching experience. Transcripts of a daily home practice session of both the mindfulness-conventional and the mindfulness-anxiety interventions can be found in the Supplemental Material. Scripts were adapted from the MBSR teacher training program and the MBCT manual (Segal et al., 2018). All interventions consisted of a 20-minute intervention delivered via headphones in the baseline session and a daily 10-minute homework intervention on 12 consecutive days.
Conventional Mindfulness
For the conventional mindfulness intervention, the content of baseline and daily interventions was similar. To start, the opening of the session consisted of instructions to commit to the practice, to find a comfortable but upright position, and to take a moment to allow the tension to leave the body and to close or find a resting point for the eyes. Instructions then focused on paying attention to the breath, observing it without trying to control it, and gently bringing attention back when noticing the mind wander (“Once you have found whether the sensations of breathing are stronger at the nostrils or the belly, bringing your attention to feeling each breath at that point. Noticing the sensations of breathing in, noticing the sensations of breathing out. Letting your breath be natural, there is no need to try and control the breath, just allowing the breath to breathe itself”). Next, the instructions moved on to focusing on bodily sensations. Again, instructions focused on observing these objects of attention without judging or reacting to them in any way (“Just opening to and allowing these sensations to be, whether they feel good, or bad, or somewhere in between. Not having to do anything about them, except to just observe them, allowing your experience to unfold in each moment, creating space for all of your experience, that occurs”). After this, the instructions moved on to expand the awareness to include thoughts. The practice involved observing these objects of attention as passing events in the mind, instead of getting lost in them or trying to control them (“And rather than following individual thoughts, or getting involved in the content of the thoughts, or going from one thought to the next, and to the next, and so forth, simply see each thought as it comes up in the mind, as a thought, as an observable event”). Finally, the focus shifted to letting go of all specific objects of attention, being aware of and being with whatever comes to awareness, noticing how it feels, and allowing it to pass.
Mindfulness With Anxiety-Specific Practice
For the mindfulness intervention with anxiety-specific practice, participants were asked in the baseline session to think about a moderately anxiety- or worry-inducing event that could be used in the subsequent practice. The in-session intervention and the first six homework interventions were equivalent to the conventional mindfulness intervention. The reason that the first half of the intervention consisted of conventional mindfulness practice was to facilitate first building mindfulness skills with relatively easy targets (e.g., breath, spontaneous thoughts) before moving to more intense targets (i.e., anxiety), as it should be more difficult to bring mindful attention to strong emotions. The intervention delivered for the latter 6 days again started with opening instructions to commit to the practice, to find a comfortable but upright position, and to take a moment to allow the tension to leave the body and to close or find a resting point for the eyes. The practice itself also started similarly by first focusing on the breath, observing it and allowing it to be, and gently bringing attention back to the breath without judgment when becoming distracted. Then, the intervention diverged from the conventional intervention, instead focusing on recalling the moderately stressful event or situation and picturing the self in that situation (“And now I would like you to bring the scenario that you’ve chosen to mind, a situation that was really stressful for you. One that you felt some nervousness in, or were experiencing worry, where you kept thinking about bad outcomes, and how to control them. Imagine yourself in that situation. See if you can feel the sensations and feelings you would experience if you were actually there, in that situation”). The instructions then focused on noticing the sensations and emotions associated with the experience, without judgment and without needing to change them (“Really picturing yourself in that place, situation, […], bring yourself right to that point where your emotions are getting strong, and then just pausing here for a moment, noticing the emotions that arise, noticing the physical sensations you’re experiencing, […] just allowing the sensations to be, just observing them without needing to change them in any way.” The exercise then moved on to thoughts that arise with the experience, again to observing these objects of attention arise and subside without getting involved in them or trying to fight them (“Just observing thoughts as though each thought was a cloud in the sky, as that thought comes into your awareness, stays for a while, and if you don’t feed it, if you don’t get involved with it, noticing that the thought eventually passes away”). Finally, the focus shifted to letting go of the experience and returning attention to the breath. Participants were free to use the anxiety-inducing event thought of in the first session or different moderately anxiety-inducing memories.
Control
The control intervention consisted of listening to consecutive recordings of excerpts from the book Harry Potter and the Sorcerer’s stone (Rowling, 1997). This audiobook was chosen due to its popularity, as it was assumed to be engaging to a wide range of participants. This was to ensure the engagement of the control group with the intervention. Before the start of each excerpt, instructions included to commit to listening to the excerpt, allowing the self to get absorbed in the story, and bringing attention back to the audio when finding that the mind has wandered.
Measures
Panic and Phobia
Symptoms associated with panic disorder and social anxiety were assessed with the Albany Panic and Phobia Questionnaire (APPQ; Rapee et al., 1994/1995). The scale’s 24 items describing symptom-relevant situations were rated according to how much fear they would induce if they occurred in the next week on a 9-point Likert-type scale ranging from 0 (“no fear”) to 8 (“extreme fear”). Items correspond to three subscales: agoraphobia (e.g., “driving on highways”), interoceptive fear (e.g., “playing a vigorous sport on a hot day”), and social phobia (e.g., “eating in front of others”). Cronbach’s alphas at baseline indicated acceptable internal consistency for interoceptive fear (α = .780), good internal consistency for agoraphobia (α = .80) and excellent internal consistency for social phobia (α = .92) at baseline. At follow-up, Cronbach’s alphas indicated good internal consistency for interoceptive fear (α = .86) and agoraphobia (α = .81), and excellent internal consistency for the social phobia subscale (α = .92). The scale has been found to have good test-retest reliability (Rapee et al., 1994/1995).
Worry
Worry was assessed with the Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990). The questionnaire consists of 16 statements describing the individual’s experience with worrying (e.g., “My worries overwhelm me”) that are rated according to the extent to which they are true for the individual on a 5-point Likert-type scale ranging from 1 (“does not describe me”) to 5 (“describes me perfectly”). Cronbach’s alpha indicated excellent internal consistency at baseline (α = .91) and follow-up (α = .92). The PSWQ has demonstrated good test-retest reliability (Meyer et al., 1990).
Trait Mindfulness
Trait mindfulness was assessed with the short form of the Five Facet Mindfulness Questionnaire (FFMQ-SF; Bohlmeijer et al., 2011). The scale consists of 24 self-statements related to different facets of mindfulness that are rated on a 5-point Likert-type scale ranging from 1 (“never or rarely true”) to 5 (“very often or always true”) according to the extent to which they are true for the individual. The items assess five facets thought to represent trait mindfulness: non-reactivity (e.g., “When I have distressing thoughts or images, I just notice them and let them go”), observing (e.g., “I notice the smells and aromas of things”), acting with awareness (e.g., “I rush through activities without being really attentive to them”), describing (e.g., “I’m good at finding the words to describe my feelings”), and non-judging (e.g., “I tell myself that I shouldn’t be feeling the way I’m feeling”). A sum score was used in the present analysis for the sake of parsimony and because there were no specific hypotheses regarding the subscales. There is research suggesting that the observing subscale may not be a valid indicator of ability to observe mindfully in novice meditators, as evidenced by findings that the factor structure of the FFMQ is inconsistent depending on whether the sample consists of inexperienced or experienced meditators (Gu et al., 2016). The quality of observing may be different depending on the respondent and this seems to not be well captured with the current items on this subscale. It has been suggested that a four-factor solution best reflects the construct in participants with little or no experience and therefore to use either only the four other subscales or a sum score without the observing subscale (Gu et al., 2016). Thus, the observe subscale was excluded from the sum score. Cronbach’s alpha indicated good internal consistency at baseline (α = .85) and follow-up (α = .89). Research has demonstrated that the FFMQ-SF is sensitive to change in response to treatment (Bohlmeijer et al., 2011).
Data Analyses
Analyses were conducted using IBM SPSS Statistics 25. The preliminary analysis included bivariate correlations at baseline to see if the variables correlated in the expected directions. To examine differences on post-intervention scores between the groups, controlling for baseline scores, a one-way ANCOVA was conducted for each outcome variable. The decision to use ANCOVA was based on recommendations that for pre-post control group designs, ANCOVA is the more powerful method of analysis for assessing between-group differences in pre-post control group designs (See e.g., Dugard & Todman, 1995; van Broekelen, 2013). Effect size estimates used were partial eta squared, with values of .01, .06, and .14 defined as respectively indicating small, medium, and large effects. Where the F-test indicated significant between-group differences, Holm-Bonferroni-corrected pairwise comparisons were examined to determine which groups differed significantly. The Holm-Bonferroni method was used to control the family-wise error rate. Here, the smallest to largest p-values were tested against significance levels of .0167, .025, and .05, respectively.
A post-hoc power analysis for ANCOVA F-tests (Fixed effects, main effects, and interactions) conducted in G*Power (version 3.1.9.4) showed a power of .15 for small effects (f = .10), .66 for medium effect sizes (f = .25) and a power of .98 for large effects (f = .40). A supplementary analysis using the full sample is provided in the Supplemental Material.
Results
Means and Standard Errors at Pre- and Post-Intervention Assessment, and Adjusted Post-Intervention Means Per Group for the Completer Sample.

Note. APPQ = Albany panic and phobia questionnaire; APPQ SP = social anxiety subscale; APPQ AG = agoraphobia subscale; APPQ IN = interoceptive fear subscale; PSWQ = Penn state worry questionnaire; FFMQ-O = five facet mindfulness questionnaire sum score without observe subscale; M = mindfulness-conventional condition; M + A = mindfulness-anxiety condition.
Adjusted post-intervention means estimated at mean of baseline covariate.
Responses to Self-Report Questions Assessing Frequency of Practice Completion After the First and Second Half of the Intervention per Condition.

Bivariate Correlations Between All Variables at Baseline.

Note. Correlations derived from full sample (N = 148).
APPQ = Albany panic and phobia questionnaire; APPQ SP = social anxiety subscale; APPQ AG = agoraphobia subscale; APPQ IN = interoceptive fear subscale; PSWQ = Penn state worry questionnaire; FFMQ-O = five facet mindfulness questionnaire sum score without observe subscale.
*p < .05, **p < .01.
Hypothesis Testing
F-Tests, Associated p-Values, and Effect Sizes for Each Outcome Variable.

Note. * = F-test for interaction effect; df = degrees of freedom; APPQ = Albany panic and phobia questionnaire; APPQ SP = social anxiety subscale; APPQ AG = agoraphobia subscale; APPQ IN = interoceptive fear subscale; PSWQ = Penn state worry questionnaire; FFMQ-O = five facet mindfulness questionnaire sum score without observe subscale.
Multiple Comparisons at Low and High Baseline Symptom Levels for Analyses With Significant Baseline Symptom and Condition Intervention Effects for the Completer Sample, Outliers Omitted.

Note. APPQ = Albany panic and phobia questionnaire; APPQ SP = social anxiety subscale; APPQ AG = agoraphobia subscale; APPQ IN = interoceptive fear subscale; PSWQ = Penn state worry questionnaire; FFMQ-O = five facet mindfulness questionnaire sum score without observe subscale; C = control condition; M = mindfulness-conventional condition; M + A = mindfulness-anxiety condition.
Adjusted Mean Difference is based on estimated marginal means.
*significant under Holm-Bonferroni correction.
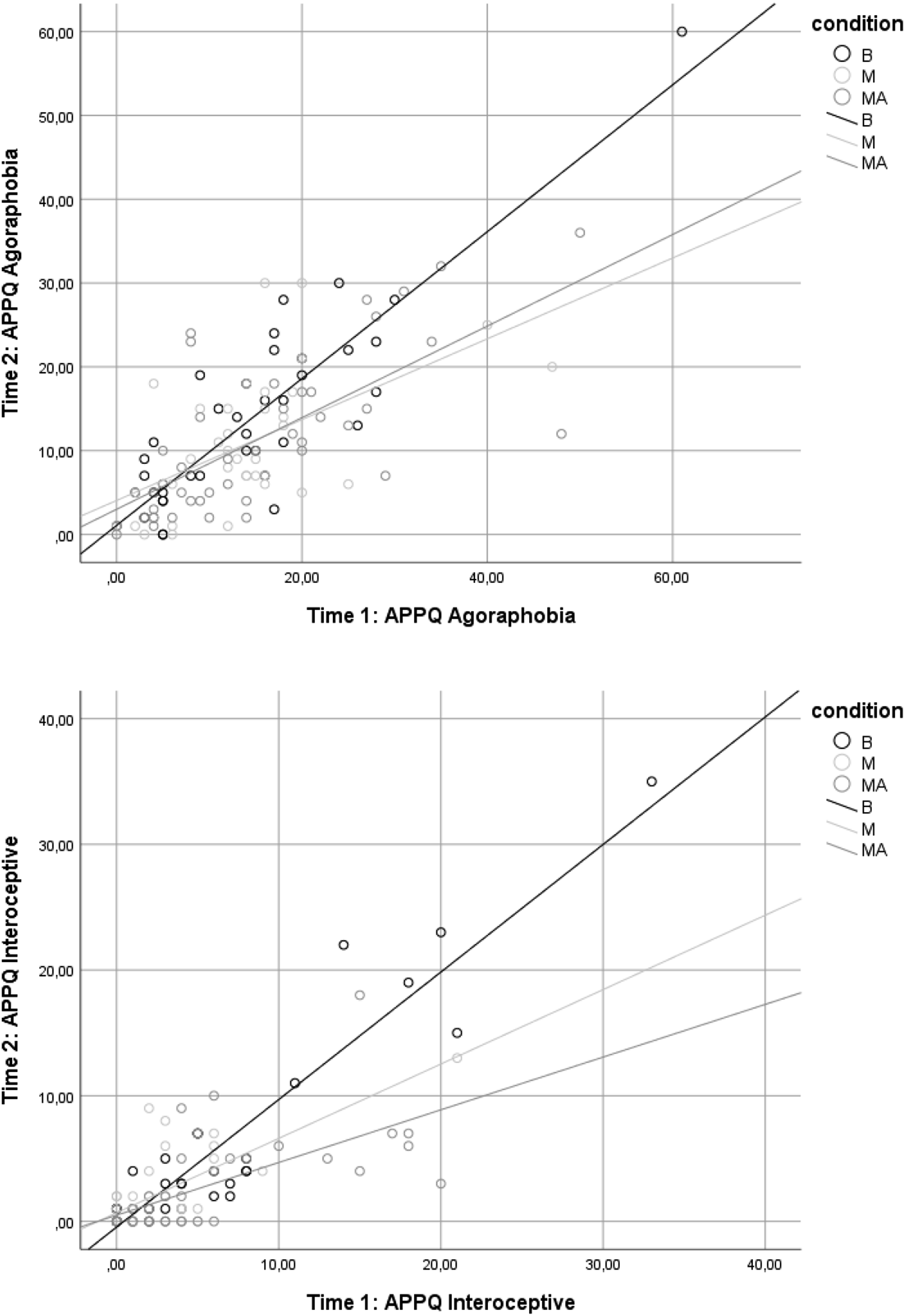
Scatterplots of Post-Intervention Symptom Levels on Baseline Symptom Levels for Agoraphobia and Interoceptive Fear Symptoms, With Separate Fit Lines for Each Group. APPQ = Albany Panic and Phobia Questionnaire.
Anxiety Symptoms
For social anxiety, the effect of condition was significant and associated with a medium effect size. Multiple comparisons revealed a significant difference between the control and mindfulness-anxiety conditions (p = .013) with lower symptoms for the mindfulness-anxiety condition. The differences between control and mindfulness-conventional and between the two mindfulness groups were not statistically significant (ps > .05). Thus, the mindfulness-anxiety group showed significantly lower post-intervention social anxiety symptoms compared to the control group, but no significant differences were shown between the two mindfulness groups.
For agoraphobia, because the relationship between baseline symptoms and group assignment varied, we focused on analyzing the interaction effects. Follow-up multiple comparisons showed no significant between-group differences at low levels (i.e., 25th percentile) of baseline symptoms. However, at high levels (75th percentile) of baseline agoraphobia, there were significant differences between the control and both the mindfulness-conventional (p = .004) and mindfulness-anxiety (p = .003) conditions, with lower symptom levels for the mindfulness-conventional and mindfulness-anxiety groups than the control group. The difference between the mindfulness-conventional and mindfulness-anxiety conditions was not significant. 2 In sum, only for high baseline symptom levels, both the mindfulness-anxiety group and the mindfulness-conventional group showed significantly lower post-intervention agoraphobia symptoms compared to the control group, while no significant differences were shown between the two mindfulness groups.
Similarly, for interoceptive fear, as the relationship between baseline symptoms and group assignment varied, the interaction effects were again analyzed. Multiple comparisons showed no significant between-group differences at low levels of baseline symptoms. Note, however, that the 25th percentile is at a score of zero on baseline symptoms (see Table 5), indicating that at low levels, any comparisons would not be valid due to floor effects. However, at high levels (75th percentile) of baseline interoceptive fear, the difference between the control and mindfulness-anxiety groups was again significant (p < .001), with lower symptom levels for the mindfulness-anxiety group than the control group. There was no significant difference between control and the mindfulness-conventional group (p = .052), or between the mindfulness-conventional and mindfulness-anxiety groups (p = .089). The normality assumption was violated. Following identification and removal of eight residual outliers (control: 1 low, 1 high, mindfulness – conventional: 2 high, mindfulness-anxiety: 1 low, 3 high), the only differences in multiple comparisons at high levels of baseline symptoms were a significant difference between the control group and the mindfulness-conventional (p = .007) and between the mindfulness-conventional and mindfulness-anxiety groups (p = .007). 3 In summary, again only for high baseline symptom levels, the mindfulness-anxiety group showed significantly lower post-intervention interoceptive fear symptoms compared to the control group, while no significant differences were shown between the two mindfulness groups. Only after outlier removal, significantly lower post-intervention interoceptive fear symptoms were also shown for the mindfulness-anxiety group compared to the mindfulness-conventional group.
For worry, the effect of condition was not significant. 4 As seen in column (c) of Table 1, although differences were not significant estimated marginal means for the mindfulness-anxiety group were lowest, while estimated means for the control and mindfulness-conventional groups were similar. Thus, no significant differences between conditions were shown on post-intervention worry symptoms.
Trait Mindfulness
Finally, to investigate H2, an ANCOVA was conducted on FFMQ scores. The results for trait mindfulness indicated no significant effect of condition. 5 The estimated marginal means were close together, with estimated means for the control group being slightly lower, followed by the means of the mindfulness-conventional group and the mindfulness-anxiety group, respectively. An exploratory ANCOVA was also conducted on each of the mindfulness subscales to see whether the intervention changed any specific facets of mindfulness. However, the results indicated that the intervention did not have a significant effect on any subscale. In sum, no significant differences between conditions were shown on post-intervention trait mindfulness.
Discussion
The present study investigated whether adding anxiety-specific practice to a brief mindfulness intervention may enhance its effects. We expected lower post-intervention scores on (H1) different anxiety symptoms and worry for a brief mindfulness intervention with anxiety-specific practice, followed by a brief conventional mindfulness intervention, and finally the audiobook control intervention. We further expected (H2) the highest post-intervention mindfulness scores for the mindfulness intervention with anxiety-specific practice, followed by the conventional mindfulness intervention, and finally the audiobook control intervention.
The hypotheses were partially supported by the data. Regarding (H1), results showed that the mindfulness-anxiety group exhibited lower post-intervention symptoms on social anxiety, as well as agoraphobia and interoceptive fear (albeit only for high baseline symptom levels), compared to the audiobook control. The mindfulness-conventional group only exhibited lower post-intervention symptom levels compared to control on agoraphobia symptoms, again only for high levels of baseline symptoms. Analyses with outliers removed in response to violation of the normality assumption showed additional findings that for interoceptive fear at high baseline levels, symptoms at post-intervention were also lower for the mindfulness-conventional compared to the control group, and lower for the mindfulness-anxiety group compared to the mindfulness-conventional group. However, the findings from the analysis with outliers removed need to be interpreted with caution, as we cannot be sure that outliers represent measurement error and as removal of outliers can inflate Type 1 error rates when data deviate from normality (Karch, 2023). For worry, there were no significant main effects. In sum, results suggest that a mindfulness-anxiety intervention can be beneficial compared to an audiobook control for social anxiety, agoraphobia, and interoceptive fear.
The fact that the mindfulness-conventional intervention showed mostly non-significant effects, compared to the audiobook control, is somewhat at odds with previous research regarding online and audio-based brief mindfulness interventions. Previous studies have shown significant anxiety-reducing effects for brief audio-based interventions of varying lengths (Howarth et al., 2019) and in student samples (e.g., Barcaccia et al., 2024; Cavanagh et al., 2013). However, the effect sizes in these studies were shown to be small to medium, and thus the difference in findings could stem from the present study being underpowered to detect small effects. However, there have been other studies that have reported null findings for brief online mindfulness interventions applied to student samples: One study found no significant effect of a 28-day app-based mindfulness intervention on a screening for anxiety symptoms, compared to an active psychoeducation control condition (Lahtinen et al., 2021) and a review of studies investigating effects of mindfulness interventions in healthy student samples concluded that when compared to active control conditions, the effect of mindfulness interventions on trait anxiety was not shown to be superior (Dawson et al., 2020). Thus, our findings regarding the effects of the mindfulness-conventional intervention on anxiety symptoms fit into an already mixed evidence base. There is a large variability in intervention lengths and protocols, and systematically reviewing which intervention intensity is effective in the reduction of anxiety symptoms will be crucial in order to design good brief and audio-based interventions.
Although the results suggest that compared to control, participants completing a mindfulness intervention with anxiety-specific practice showed lower levels of symptoms post-intervention; whereas those completing a conventional mindfulness intervention did not, there was no convincing evidence for significant differences between the two mindfulness interventions (i.e., there was only a difference for interoceptive fear when outliers were removed). The non-significant differences between the two mindfulness conditions could be due to a number of factors. One possibility is that adding anxiety-specific practice may indeed not be associated with overall greater benefits compared to conventional mindfulness practice. If this is corroborated in future studies, this would suggest that tailoring mindfulness approaches to anxiety symptoms does not have an added benefit over more general mindfulness interventions and thus, resources should not be allocated to such tailored interventions. The findings of the present study do not permit such a conclusion however, as the findings are preliminary. There is little research comparing tailored versus general treatment approaches within the realm of mindfulness interventions. However, there is initial research to suggest that there may be benefit of tailoring approaches to their target population, with one study showing beneficial effects of a tailored mindfulness intervention (i.e., including elements that were designed to facilitate engagement for the specific target population, such as including relevant local images/phrases, emphasizing mindfulness as a life attitude and integration of the practice into daily routines) compared to a relaxation training control condition on multiple outcomes, including depressive symptoms (Cheng et al., 2023). However, the intervention in that study was not tailored towards specific symptoms, but rather towards facilitating engagement in daily life for a specific target population (Cheng et al., 2023). However, to the extent that a tailored intervention has the aim of facilitating mindful engagement in relevant daily contexts, the idea behind tailoring mindfulness interventions has similarities. Thus, it remains to be determined whether tailoring mindfulness interventions to specific symptoms such as those of anxiety adds substantially to the effect of more general mindfulness interventions. The effects of the mindfulness-anxiety intervention warrant more thorough investigation of the benefit of adding anxiety-specific practice.
Another possible explanation for the non-significant differences between the two mindfulness interventions is that the statistical power of the study was too low to detect an effect—that is, the mindfulness-anxiety condition may be associated with greater benefits on anxiety than the mindfulness-conventional condition, but that these effects are too small to be detected with the current sample, as the power to detect small effects was only .15. Indeed, the effect between the two interventions can likely be assumed to be small, as both interventions include mindfulness training and differ only in terms of the added anxiety-specific focus of the mindfulness-anxiety intervention during the second intervention week. Moreover, participants reported having completed on average approximately five of the latter six sessions, which may have further diminished the difference between the two intervention (see Table 2). Although we assumed that introducing the anxiety-specific elements only from day 7 onwards would be the best strategy in order to first build mindfulness skills before moving to more difficult targets such as anxious memories, future studies may consider introducing the anxiety-specific practice earlier to set the intervention more clearly apart from the conventional mindfulness intervention. Furthermore, future research would benefit from testing these hypotheses in larger samples.
A third possible explanation for the non-significant differences between the two mindfulness interventions regards the methods used in this research. We conducted the study from an experimental psychopathology approach with the aim of providing proof-of-principle evidence regarding whether adding anxiety-specific elements would be beneficial. Following methods typical in experimental psychopathology we used a non-clinical sample and a relatively low-intensity intervention (Waters et al., 2017; Zvolensky et al., 2001). Although this approach has a number of benefits, including that it can help determine whether resources should be directed to more costly clinical studies, the sample and intervention intensity may have contributed to the non-significant findings in the comparisons between mindfulness and mindfulness with anxiety-specific practice.
Specifically, the use of an unselected non-clinical sample means that participants may not have exhibited sufficient symptom levels to benefit from the intervention significantly, which may explain the general lack of main effects of both interventions. Two considerations in the present study support this perspective for agoraphobia and interoceptive fear. First, the analyses showed that for agoraphobia and interoceptive fear, mindfulness was associated with lower post-intervention symptom levels compared to control only at higher levels of baseline symptoms, so the intervention may work better for samples with elevated anxiety. Second, on the interoceptive fear subscale 28% of the sample had a zero-score prior to the intervention, thus there was little room for improvement on this dimension. The finding that participants with more panic-disorder symptoms seem to have benefited more from the mindfulness interventions is supported by previous findings that mindfulness interventions improve agoraphobia and panic symptoms in participants who meet criteria for panic disorder (Kabat-Zinn, 2015; Ninomiya et al., 2019). Other research with student samples has shown similar findings—for example, benefits of a 1-week mindfulness intervention on depression occurred for participants with higher baseline levels but not lower levels of depression (Vollbehr et al., 2024). Future research should investigate these interventions in samples with elevated anxiety symptoms in order to avoid floor effects.
In addition, although the study was conducted with a dose of the intervention we expected to be strong enough to influence anxiety, the dose was not as intense as typical of clinical interventions. This factor may be especially relevant for worry, which was moderately elevated in this sample (31.8% demonstrated heightened worry using the cutoff score suggested by Behar et al., 2003). One feature of worry is that it is more generalized and concerns a wide range of situations, lacking a specific focus (Roemer & Orsillo, 2002). The pervasive nature of worry may mean that a longer mindfulness intervention is needed to have a significant impact on the breadth of situations that would normally trigger worry. Indeed, beneficial effects of mindfulness interventions on worry have been typically found with more extensive interventions such as MBCT (Querstret et al., 2020). However, previous research with relatively brief mindfulness interventions has shown effects on worry (Sass et al., 2019). Two methodological differences may explain the discrepancy between these findings and those of the current study. First, the intervention used in the study by Sass and colleagues (2019) was 2.5 times longer (5 × 75 min) than the intervention used in the present study. Second, given that their control group did not receive any intervention compared to the active control in the current study, the comparison in the study by Sass and colleagues (2019) may be more likely to show effects. In social anxiety, agoraphobia and interoceptive fear symptoms, the objects of fear are more specific, which may suggest that the practice of responding mindfully to these situations may more easily generalize to situations relevant to these symptom dimensions. Alternatively, a different intervention focus may be helpful to tailor mindfulness interventions for worry. Newer theoretical approaches have suggested that worry serves the specific function of avoiding affective reactivity associated with emotional shifts from neutral to negative states (Newman et al., 2014). Worry is thereby thought to be used to reinstate a sense of control over emotional experience (Newman et al., 2014). Thus, a mindfulness intervention with worry-specific practice may instead focus on memories of sudden emotional shifts (e.g., of receiving unexpected bad news such as having failed an exam). Presumably, this could facilitate learning that negative shifts in affect need not be feared and that attempts to control emotional experience are not needed or beneficial, and concomitantly developing a tolerance toward such changes in affect. In sum, more research is needed to further investigate effects on worry at higher doses of the intervention in order to derive more confident conclusions regarding whether the addition of anxiety-specific practice has an alleviating effect on worry or not. Given the above considerations, it is a real possibility that this type of anxiety-specific practice does not have a beneficial effect on worry outcomes. If that is the case, this type of intervention should not be implemented as an intervention for worry.
Regarding (H2), between-group differences on trait mindfulness were non-significant. One explanation for this could be that a brief intervention may be enough to decrease anxiety symptoms but not enough to consistently enhance trait mindfulness. Our hypotheses were based on the idea that practicing mindfulness would increase state mindfulness, and that repeated practice would lead to increased trait mindfulness over time (Kiken et al., 2015). However, although the Five Facet Mindfulness Questionnaire is a reliable trait measure, it has recently been found to be relatively insensitive to state changes (Truong et al., 2020). It stands to reason that a 12-day mindfulness intervention may not sufficiently affect trait mindfulness. The extremely small effect size associated with the non-significant main effect is in line with this explanation. However, there is a lack of research investigating a possible dose-response relationship between time spent meditating and changes in levels of mindfulness in the context of brief interventions, and future research should investigate this. Although a previous study using a similar design showed that a brief mindfulness intervention increased trait mindfulness, the effect size was small and a different measure of mindfulness was used (i.e., the Mindful Attention and Awareness Scale; Forbes et al., 2018). Different trait mindfulness scales may exhibit different levels of sensitivity to change in state mindfulness, so the reason for these different findings is unclear. Moreover, problems with the assessment of trait mindfulness have been noted in the literature, such as validity concerns related to potentially large individual differences regarding the ability of observing one’s own mind, which is required when responding to common self-report mindfulness measures (Davidson & Kaszniak, 2015), calling into question the use of trait mindfulness measures to assess the effect of mindfulness interventions.
Because there was no difference on post-intervention trait mindfulness between groups, it is unclear what the mechanisms for the effect of our intervention on anxiety symptoms were. One possibility is that even though mindfulness training for anxiety may not lead to general improvements in trait mindfulness, such training could lead to improved mindful coping in anxiety-inducing situations. Assessment of such mindful coping may require neither trait or state mindfulness, but a process measure assessing use of mindful coping. One such scale was developed by Li et al. (2016) to assess the extent to which mindfulness is used to cope with stressors. Their measure operationalizes mindful coping as being able to take a decentered stance on thoughts and emotions (i.e., not identifying with thoughts and emotions and not perceiving them as necessarily reflecting the truth), as fostering enhanced processing of positive experience and appraisal of experience as positive, as well as fostering relaxation and non-reactivity in response to distress (Li et al., 2016). Indeed, decentering, reappraisal and decreased affective reactivity have all been proposed and investigated as potential mechanisms for the benefits of mindfulness practice and have been associated with positive treatment outcomes (e.g., Hoge et al., 2014; Ostafin et al., 2014; Pruessner et al., 2024). It could be argued that mindfulness practice that is applied to specific relevant unpleasant experiences such as anxiety facilitates this process of coping mindfully. Specific aspects of mindful coping that may be facilitated through anxiety-specific practice are those related to decentering and non-reactivity, as symptom-specific practice could facilitate taking a more detached stance from anxious thoughts as well as facilitate a non-reactive approach towards specific experience, whereby an anxiety-inducing experience can be observed to arise and subside without having to react to it. Future studies could explore these processes in the context of our intervention and investigate whether they mediate the effect of the intervention on anxiety outcomes to shed further light on the mechanisms of the mindfulness-anxiety intervention.
Alternatively, it would be informative to investigate whether exposure may be responsible for the observed between-group differences. Similar to imaginal exposure, instructions during the mindfulness intervention with anxiety-specific practice involved picturing the self in an anxiety-inducing situation and observing associated sensations and thoughts without trying to fight them. As the results suggest that the mindfulness—anxiety group showed lower levels of post-intervention symptoms on social anxiety, as well as for higher baseline symptom levels of agoraphobia and interoceptive fear, symptoms which are commonly treated with exposure-based approaches, this option also seems plausible. Indeed, exposure to aversive emotional experience has previously been suggested to be one mechanism by which mindfulness exerts its beneficial effects (e.g., Shapiro et al., 2024). Through being aware and paying attention mindfully, generally, exposure to unpleasant emotional experience is thought to be facilitated which in turn enables learning that unpleasant emotions such as anxiety can be tolerated and do not require avoidance (Shapiro et al., 2024). This exposure effect may be facilitated through symptom-targeted mindfulness practice, and this should be explored further in future studies. It would also be important to compare anxiety-specific mindfulness practice to recall of an anxiety-inducing situation without mindful awareness to assess whether anxiety-specific mindfulness has an effect beyond exposure to anxiety-inducing memories.
Finally, it cannot be ruled out that the intervention had an impact simply because it was explicitly focused on anxiety. Thus, to rule out potential placebo effects, investigating mechanisms and expectancies associated with the intervention is an important next step.
Limitations and Future Research
A number of limitations need to be considered when interpreting the findings. As mentioned above, as part of conducting this pilot study from an experimental psychopathology perspective, it was conducted in a non-clinical student sample. This use of a student sample with relatively low anxiety levels may limit the generalizability of the findings to populations with heightened anxiety levels and clinical populations. It is possible that students respond differently to brief interventions compared to populations experiencing some level of symptoms. For instance, that participation was tied to the fulfillment of course requirements may mean that participants were primarily extrinsically rather than intrinsically motivated. To enhance generalizability, future studies should test the intervention in samples with elevated anxiety and clinical samples.
Regarding both the conventional mindfulness intervention and the intervention with anxiety-specific practice, we did not include manipulation checks. Thus, we cannot know the extent to which the mindfulness instructions were followed as instructed and the extent to which the group exposed to the mindfulness intervention with anxiety-specific practice actually engaged in the anxiety-specific elements of the intervention. This limits the strength of inference about effects on the mindfulness conditions. Responses to the self-report items on frequency of engagement with the practice provide some value as they suggest that participants did largely complete the practice during the latter 6 days of the intervention (see Table 2). However, we cannot be certain that participants in the mindfulness conditions followed the practice as intended. Similarly, we cannot be certain that participants in the intervention with anxiety-specific practice actually recalled and applied the practice to anxious memories during those parts of the practice focused on anxiety-specific mindfulness. Similarly, we did not assess the range or aversiveness of all stressful memories used. How many different memories were used and how aversive they were may have influenced the anxiety-reducing effect of the intervention. Future studies should add a few items assessing whether anxiety-inducing memories were recalled and the practice applied to these, how aversive these memories were and whether a different memory was recalled after each session.
A limitation that may have specifically hampered the power to differentiate between the control and experimental groups lies in an attentional instruction included in the control condition. The instruction included the direction to bring attention back to the audio when finding that the mind has wandered. Given that redirecting attention from distractions to the present moment is a key element of mindfulness training, this element of the control intervention may have led to unintended mindfulness practice in the control group, reducing the contrast between the control intervention and potentially diluting observed effects. Another element of the control intervention that should be considered concerns the content of the audiobook. The Harry Potter book series may carry substantial meaning for those who grew up while the book series or associated movie series were published, which spans a period from the 1990s into the early 2010s. Since the mean age in the present sample was approximately 20, there is a possibility that the audiobook elicited associations with peaceful and pleasant memories or states, inadvertently causing decreased engagement with anxious thoughts. Previous research has indeed shown a positive association between fictional audiobooks and increased meaning in life and well-being, specifically when readers were absorbed in the content of the audiobook (Poerio & Totterdell, 2020). Increased meaning in life, in turn has been associated with decreased anxiety (Ostafin et al., 2021). In sum, the content of the audiobook as well as attentional instructions may have obscured between-group differences and thus should be adapted for future studies.
A further limitation concerns the risk of Type 1 error, which could be increased through the number of analyses conducted in the present study, as the sample size was relatively small. We did correct for family-wise error rates in follow-up analyses but did not correct for the total number of analyses. Given these considerations and the lack of power, the findings should be interpreted with caution. Nevertheless, the findings regarding the intervention effect on post-intervention anxiety levels are consistent in direction and warrant additional research to corroborate these findings.
Another consideration for future studies concerns adherence. Overall, only 79% of the sample reported completing more than 50% of the intervention, resulting in an attrition of 20.9%. This low adherence rate may have impacted the observed effects associated with the mindfulness-anxiety condition, as high engagement with anxiety-specific practices is likely necessary for meaningful symptom reduction. One reason for this suboptimal level of completion may be due to the student sample, who completed the study to fulfill course requirements, and so may have been more extrinsically rather than intrinsically motivated. Generally, lack of adherence and attrition are a common problem in research regarding intervention effectiveness, and this may be even more true for studies on mindfulness interventions, studies in university settings and those conducted in non-clinical samples. For instance, psychotherapy studies in clinical samples in university settings have been found to generally suffer from higher attrition rates (30%) compared to other settings, with an average attrition rate of 19.7% reported across settings (Swift & Greenberg, 2012). Moreover, attrition rates have been found to be quite high for mindfulness interventions, with a recent review reporting an average attrition rate of 29% in RCTs in clinical samples (Nam & Toneatto, 2016). Though there is a lack of reviews regarding attrition in online mindfulness interventions in non-clinical samples, a recent review of studies investigating self-help (including online) in different samples (clinical, experiencing symptoms, and non-clinical) concluded that adherence in these was generally even lower (on average, 48% of participants met varying completion criteria; Cavanagh et al., 2014). Attrition research is hampered by varying definitions of adherence, resulting in high variations in attrition rates (Nam & Toneatto, 2016). However, the attrition rate of 20.9% in the present sample is thus quite low compared to average attrition rates in research on mindfulness interventions and specifically self-help mindfulness interventions. Nevertheless, as it has been reported that adherence is related with outcomes (Cavanagh et al., 2014), and thus increasing adherence should be a priority when designing and optimizing mindfulness interventions. Although the impact of such strategies has been difficult to assess, according to a recent review, ways of increasing adherence that have been reported in online mindfulness interventions include engagement with a therapist, for instance, through reminders, as well as program-based strategies such as possibilities of personalizing part of the intervention, homework exercises or self-reflections (Winter et al., 2022). Future research should consider employing and investigating such methods in order to increase adherence.
Despite the limitations and considerations above, the present study also had important strengths. This study is among the first to demonstrate that incorporating anxiety-specific practices in mindfulness training can affect certain anxiety symptoms more effectively in a student sample, a population which carries a high risk of developing anxiety disorders (Gustavson et al., 2018). Although preliminary, the present findings suggest that incorporating anxiety-specific practice in brief mindfulness interventions may enhance outcomes for such sub-clinical populations, potentially providing a cost-effective approach for early intervention. There were also some strengths in the design of the current study, including that compared the mindfulness intervention with anxiety-specific practice to both a standard mindfulness intervention and an audiobook control. This way, we could assess the effect of mindfulness meditation as well as the effect of adding anxiety-specific practice. Overall, although differences between a conventional mindfulness intervention and the addition of anxiety-specific practice in most cases did not reach significance, the mindfulness intervention with anxiety-specific practice was found to be associated with enhanced outcomes on common anxiety symptoms, compared to the control condition. These findings warrant more thorough investigation in samples with elevated levels of anxiety and possibly in higher-intensity mindfulness interventions to investigate the value of adding anxiety-specific practice elements in mindfulness interventions for populations experiencing anxiety symptoms.
Supplemental Material
Supplemental Material - Adding Anxiety-Specific Practice to a Brief Audio-Based Mindfulness Intervention for Anxiety in Undergraduate Students: A Pilot Study
Supplemental Material for Adding Anxiety-Specific Practice to a Brief Audio-Based Mindfulness Intervention for Anxiety in Undergraduate Students: A Pilot Study by I. Papenfuss, M. J. J. Lommen, and B. D. Ostafin in Journal of Experimental Psychopathology
Footnotes
Ethical Statement
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.