
Abstract
Dysmorphic concerns are a core symptom of body dysmorphic disorder (BDD), a mental disorder characterized by a preoccupation with perceived appearance-related flaws. Different cognitive and perceptual biases are associated with dysmorphic concern or BDD, including object-related short-term memory deficits and superior short-term memory performance for facial features. A face-related long-term memory bias might explain the feature of perceiving flaws and why individuals with BDD experience adverse outcomes of cosmetic surgery. The present study aimed at investigating long-term memory (LTM) performance for different facial stimuli. 62 participants completed an online experiment (30 with low and 32 with high dysmorphic concern; 39 without and 23 with self-reported BDD). The experiment consisted of two consecutive old/new recognition tasks, testing memory performance of whole faces and facial features. LTM performance was higher for whole faces than for facial features across groups. Neither significant differences between the low and high dysmorphic concern groups nor an interaction of group x stimulus type were found. Post hoc exploratory analyses revealed lower long-term memory performance in individuals with versus without self-reported BDD. The results indicate that memory performance might be only affected in BDD rather than non-clinical or non–BDD-specific dysmorphic concerns.
Introduction
Body dysmorphic disorder (BDD) is a mental disorder that is characterized by a preoccupation with perceived flaws in one’s own physical appearance that are either not noticeable or appear minor to others (American Psychiatric Association, 2022). The most common areas of preoccupation are specific facial features, particularly the nose, and body features such as skin or hair (Phillips et al., 2005). Individuals with BDD often have delusional beliefs about the perceived defect and an extensive desire to alter their appearance (Phillips et al., 2014). The key features of BDD point towards the presence of biased body representations, such as high levels of body dissatisfaction (i.e. cognitive-affective body image) and a distorted perceptual body image (Möllmann et al., 2024). Prevalence estimates of BDD are around 2% in community samples of adults and adolescents (Veale et al., 2016). BDD often remains undetected, underdiagnosed, or mistaken for other disorders (Kollei et al., 2011; Schulte et al., 2020). Around 76% of individuals with (undiagnosed) BDD seek help through cosmetic surgery or minimally invasive treatments to get their perceived defect(s) fixed (Bowyer et al., 2016). Prevalence rates of BDD go up to 20.1% in cosmetic surgery samples (Veale et al., 2016). However, there is a serious risk of adverse events following surgery and dissatisfaction with the result in the presence of BDD, and such treatments can result in an exacerbation of BDD symptoms (Bowyer et al., 2016).
Research findings on visual processing and cognitive biases may help to explain the paradox effects of cosmetic surgery and, on a more general level, the discrepancy between the way individuals with BDD perceive certain aspects of their appearance compared to how others perceive these aspects. For example, several studies point towards a local, detail-oriented rather than global, holistic visual processing of (own and others’ facial) stimuli in individuals with versus without BDD (e.g., Feusner et al., 2007). In a systematic review, Beilharz et al. (2017) emphasize the overall agreement among researchers that individuals with BDD show an over-attention to details not only on their own face but also on other peoples’ faces. In general, individuals recognize facial features better when they are embedded in the whole face than when they are presented in isolation (Tanaka & Simonyi, 2016), supporting the proposition that healthy populations generally integrate face parts into a whole-face representation and therefore process faces with configural, holistic strategies. Yet, mouth and eye regions are known to be among the most crucial information individuals rely on when identifying faces (Gosselin & Schyns, 2001). An indicator for holistic face processing is the inversion effect. Holistic face processing is disrupted when stimuli are presented inverted versus upright in favor of detail-focused processing to the effect that faces are recognized more slowly and less accurately when inverted (Yin, 1969). Thus, if (face) processing in BDD was following a more detail-oriented rather than holistic strategy, the inversion effect should be smaller compared to individuals without BDD. This was reflected in some studies (e.g., Feusner et al., 2010; Jefferies et al., 2012) but not in others (Monzani et al., 2013; Ritter et al., 2020). Accordingly, Johnson et al. (2018) found a small, non-significant effect in their meta-analysis with regard to the local processing tendency of visual stimuli.
It is unclear what influences the presence or absence of this effect. Studies on selective attention are speaking in favor of the presence of a detail-oriented processing effect: Several eye-tracking studies revealed a biased visual attention for certain areas of the face, most consistent appears a focus on less liked areas with some of the studies additionally finding a pattern of neglecting most liked areas (Greenberg et al., 2014; Grocholewski et al., 2012; Kollei et al., 2017) in BDD compared to individuals without mental disorders or with social anxiety or eating disorders. Beyond the attentional bias, research has also revealed that individuals with BDD tend to have a negative interpretive bias (Buhlmann et al., 2008; Dietel et al., 2021; Hartmann et al., 2015). This tendency to exhibit a negative interpretation in ambiguous situations/stimuli is particularly present for facial expressions, that is, individuals with BDD generally interpret neutral facial expressions as threatening ones such as anger or disgust (Buhlmann et al., 2011). This line of research points towards imbalances in local versus holistic processing, a visual attention bias in favor of certain features and a negative misinterpretation bias of facial expressions.
When investigating biases in BDD, the impact of memory functioning has received relatively little emphasis in previous research, which seems somewhat surprising given the tight links between, for instance, attention and memory (Chun & Turk-Browne, 2007). So far, the existing studies have primarily focused on short-term memory components of objects rather than facial stimuli: Deckersbach et al. (2000) assessed the short-term memory performance of individuals with versus without BDD on the Rey Complex Figure Test (RCFT). Results revealed deficits in executive functioning in BDD, namely, difficulties organizing information during encoding. The study showed that the BDD group was able to store the learned information but had a deficit in free recall of the visual stimulus in comparison with healthy controls. Thus, the BDD group recalled isolated details rather than more global and larger parts of the Rey–Osterrieth figure. Similar findings on abnormalities in spatial working memory and executive functions were found in a study by Dunai et al. (2010), who compared the performance between individuals with BDD, OCD, and mentally healthy individuals. Individuals with BDD demonstrated deficits in spatial working memory as well as cognitive speed during planning tasks. These results were further supported by the authors’ subsequent study (Labuschagne et al., 2013), which also concluded greater executive functioning impairments in BDD patients than OCD patients and healthy controls. In a meta-analysis, the mean weighted effect size for short-term memory deficits (mainly immediate recall of objects) was medium (g = . 56; Johnson et al., 2018).
In contrast, in a study focusing on short-term memory with facial stimuli, which involved a change detection task, individuals with BDD compared to individuals with disfiguring or non-disfiguring dermatological conditions showed a superior performance in detecting changes in the presented facial stimuli and thus an advantage for detail-oriented facial short-term memory, potentially caused by the detail-focused processing tendency in BDD (Stangier et al., 2008). The effect that disrupted face processing and biased short-term memory functioning in individuals with BDD may have on long-term memory (LTM) of faces has not gained research attention. One may hypothesize that deficits in LTM or a memory bias for faces may override perceptual input. This hypothesis is derived from a transdiagnostic information processing model on body representations (Möllmann et al., 2024). The model proposes that the processing of online sensory input (e.g., a face stimulus) can directly be affected by long-term information of similar stimuli (e.g., a stored representation of the same face). This interaction between memory and perceptual input is not specific for body related stimuli but a general effect in information processing (e.g., Herwig & Schneider, 2014; Luck & Hollingworth, 2008; Stokes et al., 2012). Such potential deficits may explain one core symptom of BDD, namely, that individuals with BDD perceive flaws which are not visible to others in the first place. They may also explain why actual changes in the physical appearance through cosmetic surgery do not affect the core symptoms of BDD. However, this explanation would only apply if deficits were not only present in short-term memory but also established in LTM.
Irrespective of BDD status, individuals seeking cosmetic surgery usually report high levels of dysmorphic concern (Castle et al., 2004). Dysmorphic concern is one aspect of biased body representations, namely, the cognitive-affective body image. It describes concerns with the own appearance (Castle et al., 2004), sometimes also perceived malfunctions of the own body such as body odor (Oosthuizen et al., 1998). As such, measures on dysmorphic concern, such as the Dysmorphic Concern Questionnaire (DCQ; Oosthuizen et al., 1998), do not necessarily assess a clinical phenomenon but are often used as a screening tool for BDD (e.g., Schieber et al., 2018). Similarly to BDD, high dysmorphic concern has shown to be associated with some visual processing abnormalities, for example, a reduced face inversion effect (Beilharz et al., 2016).
Given the close link between the maintenance of information in working memory and long-term memory performance (Melrose et al., 2020; Nichols et al., 2006), we aimed to investigate whether the differences in short-term memory functioning reported for BDD transferred to long-term facial memory. Specifically, we aimed to determine whether facial LTM performance differed in individuals with high versus low body dysmorphic concern and whether it was affected by the type of face stimuli (whole face vs. facial features). It was expected that (1) LTM performance would be higher for whole faces versus isolated features, (2) LTM performance would be lower in individuals with high versus low body dysmorphic concern, and that (3) individuals with high body dysmorphic concern would show relatively better LTM performance compared to the low body dysmorphic concern group when being tested on isolated facial features.
Methods
Participants
Prior to recruitment of participants, a power analysis using G*Power was conducted (Faul et al., 2009) to estimate the minimum sample size to detect a medium effect (f = 0.25, power = 1-β = 80 %, α = 0.05), which was N = 54. The effect size was derived from the meta-analysis effect size on (object- and short-term-related) memory deficits (Johnson et al., 2018). A total of 80 individuals participated in the study during the defined data collection period of at least 2 weeks (see 2.2); the data of n = 62 participants were included in the analyses (100% female; M age = 32.68, SD age = 8.98, Rangeage: 20–59). The data of 18 participants were excluded because the participants only completed one of the two testing conditions (n = 12), interrupted the experiment for too long (indicated by an individual runtime > M + 1 SD; n = 4), or they did not work on the distractor task during the retention phases (n = 2).
Design and procedure
The online study had a quasi-experimental 2 x 2 mixed factorial design with the between-subjects factor dysmorphic concern (low vs. high; established via a median split on the dysmorphic concern screening tool), the within-subjects factor testing condition (whole face vs. feature during the memory test phase) and the dependent variable long-term memory performance (LTM performance).
Recruitment of participants took place in online forums and communities for individuals that were interested in, or had already carried out plastic surgery of the nose. It was decided to continue recruitment until the minimum sample size that had been determined in the power analysis was reached, with a first check after 2 weeks. Participation was voluntary and no compensation was provided for participating. The online experiment was conducted over the platform Sosci Survey. First, participants were given a short description of the purpose and procedure of the study. After providing informed consent, participants answered a brief demographic and the BDD-related questionnaires. Thereafter, the long-term memory tasks were conducted with each participant. The average run of the online-study was about 25 minutes (M = 1490s, SD = 205s).
Materials and assessments
Dysmorphic concern and BDD self-report criteria
The level of dysmorphic concern was assessed with the German translation of the screening instrument Dysmorphic Concern Questionnaire (DCQ; Oosthuizen et al., 1998; Stangier et al., 2003). The DCQ is a self-report measure consisting of seven items on a 4-point scale (from 0 = “not at all” to 3 = “much more than most people”). The sum score of the seven items can range from 0 to 21, with higher scores indicating a higher level of dysmorphic concern. Cronbach’s alpha was α = .83 in the current sample. Additionally, the BDD DSM-5 self-report criteria were assessed with the BDD-5 (Möllmann et al., 2017), consisting of six dichotomous items, reflecting the four DSM-5 criteria for BDD. We used this measure because high dysmorphic concern is not specific for individuals with BDD, but can indicate a weight-related and/or eating disorder pathology or non-clinical body dissatisfaction as well.
Facial stimuli for the memory task
The stimulus set for the memory task contained 160 face stimuli (i.e., 160 different identities; 80 per experimental condition) which were retrieved from the FACES database (Ebner et al., 2010). The stimulus set included male and female Caucasian models displaying unfamiliar faces with neutral facial expressions. The age range of the people displayed was 19–75 years.
Long-term memory performance task
Long-term memory performance was assessed in a forced-choice old/new recognition task that evaluates participants’ ability to distinguish between old and new stimuli during the test phase (i.e., stimuli that were already presented during the study phase vs. stimuli that were not previously presented). Macmillan and Creelman (2004) propose using Signal Detection Theory (SDT) to evaluate old/new face recognition tasks. The key measure of performance in SDT is d', which represents the ability to distinguish between old and new stimuli, also known as the sensitivity index (Stanislaw & Todorov, 1999). Numerous studies on face memory have adopted d' as the standard expression for evaluating memory performance (e.g., Lin et al., 2020). D′ as used in the current study (see next section) can reach values between 0 and approximately 4.65, with 0 indicating memory performance at a chance level and 4.65 indicating perfect memory performance. Besides memory performance, a general response bias c can be assessed. This bias assesses the general tendency of a person to respond “yes”, or in other words, the amount of evidence a person needs to rate a given stimulus as old. Values of 0 indicate unbiased responses; c < 0 indicates a lower and c > 0 a higher threshold to respond “yes”.
The two conditions of the memory task were identical in terms of the general procedure but differed regarding the type of stimuli (whole faces vs. facial features). Both consisted of a study phase, a retention phase, and a test phase. During the study phase, participants were presented 40 unaltered face stimuli (whole faces in both conditions) in a randomized order, each displayed for 3000 ms followed by a 1000 ms fixation cross. The subsequent retention phase included a 4-minute unrelated distractor task, namely, a computerized version of serial subtraction tasks (Serial Sevens and Serial Threes tasks) to prevent visual rehearsal of the previously seen stimuli. In the whole face condition, the test phase consisted of a total of 80 whole faces (40 old and 40 new faces). In the feature condition, the test phase consisted of 80 facial features (eyes and nose; 40 that had been extracted from the 40 faces previously shown in the study phase, and 40 new facial features). Participants were asked to respond to whether they had seen the stimulus before by clicking on “yes” or “no” on the screen, or by pressing the left or right arrow key indicating “yes” or “no”, respectively. During the test phases, answering was self-paced. Reaction times were surveyed via the online platform by default.
The stimuli in each task were presented in a randomized order. To control the effects of the repeated measures, the sequence of conditions was counterbalanced and subjects were randomly assigned to a sequence of conditions. Between the two memory tasks, participants were given the option of taking a break of up to 5 minutes, or to instantly resume with the next memory task.
Statistical analyses and data processing
Statistical analyses and data processing were conducted using IBM SPSS Statistics, Version 26 (IBM Corp, 2019), JASP (JASP Team, 2023), and Microsoft Excel.
Regarding the independent variable dysmorphic concern status, we split the sample into a low and high dysmorphic concern group. The sample median of the DCQ sum score was Mdn = 10. We included DCQ sum scores of 10 into the high concern group, based on the recommended cut-off score of 9 when screening for clinical BDD (Mancuso et al., 2010).
Regarding the dependent variable LTM performance, we determined the sensitivity index d’ for each experimental condition via the following steps (cf., Macmillan & Creelman, 2004): 1) calculation of the hit rate as proportion of old stimuli that participants correctly identified as old stimuli among all 40 old stimuli presented; 2) calculation of the false alarm rate as proportion of new stimuli that subjects falsely identified as old stimuli among all 40 new stimuli presented; 3) adjustment of extreme rates (i.e., every old stimulus was correctly detected or no new stimulus was mistaken as an old one): hit rates of 1 were reduced by 1/(2*N) and false alarm rates of 0 were increased by 1/(2*N), where N refers to the number of 40 stimuli in this study; 4) z-transformation of the hit and false alarm rates; 5) calculation d’ by subtracting the false alarm z-score from the hit rate z-score.
Descriptive statistics were performed to compare demographic characteristics of the sample, and to obtain a general overview of the variables in the data set. Differences of LTM performance (d’) depending on dysmorphic concern and testing condition were analyzed with a mixed model ANOVA (analysis of variance). In addition to analyses on d’, the same analyses were conducted for the response bias c and reaction times. 1 The significance level was set at α = 5 %. Post hoc tests were planned in case of a significant interaction effect. Bayesian statistical testing was implemented as a supplement to classical (frequentist) analyses to also quantify the amount of evidence for the presence or absence of a given effect. More precisely, we used the JASP framework for repeated measures ANOVA (van den Bergh et al., 2019) and obtained exclusion Bayes factors for predictors of interest by comparing models that contain the effect to equivalent models stripped of the effect. An exclusion Bayes factor can be seen as the evidence given the observed data for the exclusion of a particular predictor in the model and thus quantifies the evidence in favor of null results. As suggested by van Doorn et al. (2021), a Bayes factor of 1 indicates equal support for H0 and H1, a Bayes factor between 1 and 3 indicates weak, 3 to 10 moderate, and >10 strong evidence for the H1.
Results
Group characteristics
Group characteristics: Age, run time, dysmorphic concern, and BDD self-report criteria.
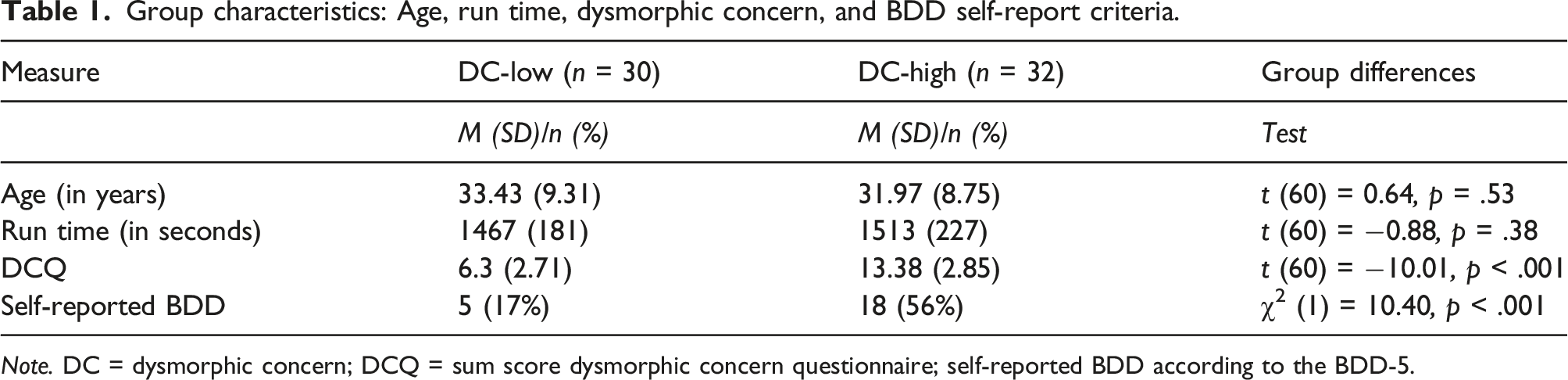
Note. DC = dysmorphic concern; DCQ = sum score dysmorphic concern questionnaire; self-reported BDD according to the BDD-5.
Long-term memory performance
Dysmorphic concern and long-term memory performance: Hit rate, false alarm rate, d’, c, and reaction times.

Note. d’ = sensitivity index and determinant of memory performance; c = response bias; DC = dysmorphic concern based on median split of DCQ sum scores. Reaction time in milliseconds as surveyed via the online platform (Means and SDs from individual median reaction times per condition).
A mixed ANOVA was conducted to determine differences in LTM performance depending on the predictors DC-group and testing condition. The results revealed a main effect of the testing condition for d’, F (1, 60) = 247.50, p < .001, η2p = 0.81, indicating better memory performance in the whole face versus feature condition across groups. There was no significant main effect of DC-group on memory performance, F (1, 60) = 0.52, p = 0.47, η2p = 0.01, indicating that the DC-group status did not affect memory performance irrespective of the testing condition. There was also no significant interaction between testing condition and DC-groups on memory performance, F (1, 60) = 0.008, p = 0.93, η2p < 0.001, see Figure 1(a). (a) and (b) Long-term memory performance. Note. Error bars indicate 95% confidence intervals. (a): DC groups based on DCQ sum score; (b) BDD status based on the BDD-5.
A complementary Bayesian ANOVA showed a BFexcl of 3.52 for the main effect of DC-groups, indicating that the data is 3.52 times more likely under the matched models that exclude than under the models that include DC-group. Likewise, the BFexcl was 3.51 for the interaction between testing condition and DC-groups, indicating that the data is 3.51 times more likely under the matched models that exclude the interaction than under the model that include the interaction.
For the response bias c, a mixed ANOVA with the factors DC-group and testing condition revealed no significant effects (testing condition: F (1, 60) = 4.00, p = 0.05, η2p = 0.06, DC-group: F (1, 60) = 1.33, p = 0.25, η2p = 0.02; interaction: F (1, 60) = 0.74, p = 0.39, η2p = 0.01), indicating no significant differences in the general tendency to respond to the task across groups and conditions.
A mixed ANOVA with the factors DC-group and testing condition on individual median reaction times revealed a significant main effect for condition, F (1, 60) = 76.85, p < .001, η2p = 0.56), indicating significantly higher reaction times in the feature versus whole face condition. The group and interaction effect were non-significant (DC-group: F (1, 60) = 0.10, p = 0.75, η2p = 0.001; interaction: F (1, 60) = 1.52, p = 0.22, η2p = 0.03).
Post hoc exploratory analyses
Self-reported BDD versus high dysmorphic concern
We conducted the same analyses based on a different group assignment, namely, based on self-reported BDD according to DSM-5 criteria, assessed with the BDD-5 (Möllmann & Buhlmann, 2017), as the descriptive statistics revealed that the measures DCQ and BDD-5 led to different group assignments.
A group assignment based on self-reported BDD (via BDD-5) rather than dysmorphic concern led to n = 23 individuals with and n = 39 individuals without self-reported BDD. From the 23 individuals with self-reported BDD, n = 18 scored in the high and n = 5 in the low dysmorphic concern group. In the group without self-reported BDD, n = 25 scored in the low and n = 14 in the high dysmorphic concern group.
Based on the group assignment via BDD-5, a mixed ANOVA on differences in LTM performance revealed a main effect of the testing condition for d’, F (1, 60) = 227.32, p < .001, η2p = 0.79, indicating better memory performance in the whole face versus feature condition across groups and a significant main effect of self-reported BDD status, F (1, 60) = 4.45, p = 0.039, η2p = 0.07, indicating worse memory performance in the BDD group. There was no significant interaction between testing condition and BDD group on memory performance, F (1, 60) = 1.01, p = 0.32, η2p < 0.02, see Figure 1(b).
The Bayesian ANOVA revealed a BFexcl of 0.68 for the main effect of BDD status, indicating that the data is 1/0.68 = 1.47 times more likely under the matched models that include than under the models that exclude BDD status. The BFexcl was 2.42 for the interaction between testing condition and BDD groups, indicating that the data is 2.42 times more likely under the matched models that exclude the interaction than under the model that include the interaction.
For the response bias c, a mixed ANOVA with the factors BDD status and testing condition revealed no significant main or interaction effects (testing condition: F (1, 60) = 3.7, p = 0.06, η2p = 0.06, BDD status: F (1, 60) = 0.001, p = 0.97, η2p < 0.001; interaction: F (1, 60) = 0.02, p = 0.90, η2p < 0.001), indicating no significant differences in the general tendency to respond to the task across groups and conditions.
Self-reported BDD and long-term memory performance: Hit rate, false alarm rate, d’, c, and reaction times.

Note. d' = sensitivity index and determinant of memory performance; c = response bias; no BDD/BDD = self-reported Body dysmorphic disorder status based on the BDD-5. Reaction time in milliseconds as surveyed via the online platform (Means and SDs from individual median reaction times per condition).
Subgroup analysis - reduced task difficulty
The mean task difficulty for the feature condition was high with weighted mean d’ values of 0.37. To rule out the possibility that the task for the feature condition was too difficult across participants and thus might have masked potential differences in memory performance between groups, we conducted the same analyses with a subgroup of participants. We included the data of those n = 33 participants (n = 15 with low and n = 18 with high dysmorphic concern) who revealed d' values for the feature condition greater than or equal to the median of d' feature, Mdn = 0.34. The mean d’ value in the feature condition was M = 0.60 in this subgroup. The mixed ANOVA on LTM performance with the factors DC-group and testing condition revealed the same pattern of results in this subgroup compared to the whole sample analysis: a main effect of the testing condition for d’, F (1, 31) = 89.05, p < .001, η2p = 0.74, no significant main effect of DC-group on memory performance, F (1, 31) = 0.12, p = 0.73, η2p = 0.004, and no significant interaction between testing condition and DC-groups on memory performance, F (1, 31) = 1.17, p = 0.29, η2p = 0.04.
Discussion
The aim of this study was to compare the long-term memory performance for faces between two types of stimuli, whole faces and facial features, and between individuals with low and high dysmorphic concern, which is a core symptom of body dysmorphic disorder. The results of the present study provide supporting evidence that LTM performance for whole faces is higher compared to facial features irrespective of low or high dysmorphic concern. Yet, the results do neither show that individuals with high (vs. low) dysmorphic concern exhibit statistically significant lower LTM performance for face stimuli, nor that high (vs. low) dysmorphic symptoms are associated with superior LTM performance for facial features. Post hoc exploratory analyses comparing groups with versus without self-reported BDD indicated lower long-term memory performance for faces in individuals with self-reported BDD.
Results in this study are only partially consistent with findings of previous literature. To begin with, results are consistent with there being a holistic advantage when facial features are presented as part of a whole face (Tanaka & Simonyi, 2016). This is reflected in LTM performance being overall higher when participants were tested on recognizing whole faces versus facial features in the current study. The analyses on reaction times support this finding with significantly lower reaction times for recognizing whole faces versus facial features. These results are in line with previous research postulating that face processing is primarily holistic rather than detail-oriented, and that global processing strategies tend to be superior (Freire et al., 2000; Taubert et al., 2011) — irrespective of BDD symptoms or dysmorphic concern.
Derived from previous research on object-related short-term memory performance in BDD, which revealed decreased memory performance (Johnson et al., 2018), we expected a similar effect for overall LTM performance for facial stimuli in individuals with high body dysmorphic concern. However, the high and low dysmorphic concern groups do not demonstrate significant differences in facial LTM performance, indicating that the short-term memory deficits found in previous research on clinical BDD do not similarly appear in long-term memory performance, at least not regarding face memory when comparing groups regarding dysmorphic concern. Further, our study does not provide evidence for a superior LTM performance for facial features versus whole faces in a high versus low dysmorphic concern group. This effect was present in a short-term memory task with facial features versus whole faces in individuals with BDD compared to individuals without BDD (Stangier et al., 2008).
These results may be interpreted in at least two ways. One interpretation would be that individuals with versus without BDD do not show reduced LTM performance for faces — in contrast to other short-term memory performance differences found in BDD (worse performance for object-related stimuli: Johnson et al., 2018; better performance for facial features: Stangier et al., 2008). If differences in LTM performance for faces did not exist in BDD, it would therefore be more likely that the findings on object-related short-term memory differences and the finding from one study on superior facial short-term memory in BDD (Stangier et al., 2008) were not primarily driven by memory processes but that processes interfered with the response to the respective tasks, for example, top-down BDD-specific response tendencies or attentional biases could have influenced the response behavior and performance.
The other interpretation would be that long-term memory performance for faces is impaired in BDD but the current study failed to detect the effect — because the effect might be specific for BDD rather than high dysmorphic concern as assessed with the DCQ. We chose the DCQ as a common BDD screening tool in combination with targeted recruitment in rhinoplasty forums with the intention to find individuals with BDD-specific dysmorphic concerns and thus a higher chance to fulfill criteria for clinical BDD. Additionally, the DCQ median split matched the recommended cut-off values. However, descriptive analyses showed that 36% of the individuals with high dysmorphic concern did not meet the BDD self-report criteria. This motivated us to conduct the exploratory post hoc analyses with group assignment based on the self-reported DSM-5 BDD criteria (BDD-5). These analyses showed lower LTM memory performance for facial stimuli in the presence versus absence of self-reported BDD. This is a first indication that the findings from previous research, namely, reduced short-term memory performance for object-related stimuli (Johnson et al., 2018), may generalize to both long-term memory and face-related stimuli in individuals with versus without BDD. In contrast, the present study did not show any evidence for a superior memory performance for facial features, as was reported by Stangier et al. (2008), neither for the groups differentiated via dysmorphic concern nor for self-reported BDD. The potential superiority effect may be thus further investigated in future studies.
Limitations
Several potential limitations should be recognized. As discussed, the group assignment was based on a dysmorphic concern self-report questionnaire. All studies that have reported differences in memory performance in BDD compared groups with and without a clinical diagnosis of BDD. Our study has provided some evidence that long-term memory performance might be a qualitative difference between dysmorphic concerns and BDD, indicating that future studies on memory processes may rather use a clinical diagnosis or BDD-specific instrument. A second potential limitation is task-related. The mean task difficulty for the feature condition was high, indicated by d’ values around 0.37. Reducing task difficulty in this condition may be beneficial as it would increase the chance to detect potential performance differences between groups. To explore the potential masking effect of task difficulty, we conducted post-hoc analyses with a subgroup of those individuals revealing d’ feature values equal to or above the median. The same pattern of results speaks against a floor effect and rather supports the interpretation that LTM performance does not differ in individuals with low versus high dysmorphic concern.
Conclusions
In conclusion, the findings of this study provide evidence that the LTM performance is higher for whole faces than for isolated facial features. Further, the results of the current study indicate that long-term memory performance for facial stimuli may be impaired in BDD but not high dysmorphic concern. Specifically, the results indicate that the findings of previous research (1) on (object-related) short-term memory deficits in BDD may be generalized to facial long-term memory in self-reported BDD (but not high dysmorphic concern) and (2) on superior short-term memory for facial features in BDD can be neither generalized to long-term memory for facial features in high dysmorphic concern nor self-reported BDD. Thus, the study highlights the possibility that LTM performance of faces might not be strongly affected in dysmorphic concern, even if other processing abnormalities, such as a reduced face inversion effect, were found in other studies focusing on dysmorphic concern. However, for BDD, LTM performance may be reduced, similarly to working-memory deficits and processing abnormalities during visual encoding. As this is one of the first studies on long-term memory for faces in relation to BDD, the findings should still be interpreted cautiously and compared with future studies on LTM for faces in BDD.
Footnotes
Author Contributions
Conceptualization: AM, AH, and NH; Methodology: CP, AH; Formal analysis and investigation: AM, CP, and AH; Writing—original draft preparation: AM and CP; Writing—review and editing: AM, CP, NH, and AH; Resources: NH; Supervision: NH and AH.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Open Access Publication Fund of Bielefeld University and the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG) (MO4224/1-1).
Ethical statement
Data Availability Statement
The datasets generated and analyzed during the current study is available through https://osf.io/a24yt/.