
Abstract
Difficulty tolerating distress (e.g., distress tolerance [DT]) and regulating emotions (e.g., emotion regulation [ER]) are implicated as transdiagnostic risk factors for various internalizing disorders. The present study investigated the relationships among six internalizing disorder symptoms, baseline ER, and DT in college students (N = 137) to identify which internalizing disorders were most closely associated with DT. We expected ER and internalizing symptoms to be associated with DT and that ER would moderate relationships among internalizing symptoms and both trait DT and state distress. Results indicated that ER, Post-traumatic Stress Disorder (PTSD), and social anxiety symptoms influenced trait DT. ER moderated the associations between depression, anxiety, and panic disorder (PD) symptoms, and trait DT at the .05 level. Similarly, ER moderated the association between PD symptoms and anticipatory distress at the .05 level. However, these analyses did not withstand the Bonferroni adjustment (p = .008) for multiple comparisons. Findings suggest that, when considering transdiagnostic symptoms, certain internalizing symptoms (i.e., social anxiety, PTSD) may have a stronger influence on trait DT. Further, strong ER abilities may buffer the adverse effects of internalizing symptoms on one’s perceived ability to handle distress. These patterns may not translate to individuals’ behavioral capacity to handle distress.
Introduction
There is growing research examining transdiagnostic approaches to studying, conceptualizing, and treating psychopathology, such as the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2017) model and Research Domain Criteria (RDoC; Insel et al., 2010), which offer an alternative perspective to the traditional categorical diagnostic systems, such as the Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev.; DSM-5-TR; American Psychiatric Association [APA], 2022). Transdiagnostic frameworks conceptualize mental health disorders as continua of symptomology, moving away from strict diagnostic categories to address shortcomings of the categorical approach, such as high comorbidity rates among disorders (e.g., Van Loo & Romeijn, 2015) and evidence of limited diagnostic reliability of the DSM-5 (e.g., Newson et al., 2021). Additionally, as outlined by Kotav and colleagues (2017), traditional methods struggle to identify individuals who experience significant distress or impairment but do not meet the criteria for any specific disorder. Importantly, this growing approach may offer a more precise understanding of psychological distress associated with symptoms across diagnostic categories to allow for more targeted interventions (e.g., Sunderland & Slade, 2015). Altogether, these initiatives emphasize examining transdiagnostic factors (e.g., distress tolerance, emotion regulation) across traditional diagnostic boundaries to obtain a more comprehensive understanding of psychopathology (e.g., Clark et al., 2023), as well as examining relations between a range of symptom dimensions across diagnostic boundaries (e.g., Stanton et al., 2020). Distress tolerance (DT) is one such factor that plays a significant role in the etiology and maintenance of several psychological disorders (Leyro et al., 2010).
DT refers to an individual’s perceived or behavioral capacity to endure and withstand negative or uncomfortable emotional states (Simons & Gaher, 2005) and has been extensively studied using various measures. One notable self-report measure is the Distress Tolerance Scale (DTS; Simons & Gaher, 2005). The DTS assesses an individual’s perceived ability to endure and cope with distressing situations, often referred to as trait DT (Veilleux et al., 2019). Researchers have also employed objective measures (e.g., Carpenter et al., 2019) to behaviorally assess individuals’ distress abilities. A common behavioral DT task, particularly assessed with trauma-related disorders, is the trauma film paradigm, which instructs participants to watch distressing films depicting traumatic scenes (Holmes & Bourne, 2008). Studies have used the Subjective Units of Distress Scale (SUDS; Wolpe, 1969) to quantify the distress experienced during such tasks, which allows participants to assign a numerical value to indicate their subjective distress levels at different time points while engaging in the task (e.g., Siegesleitner et al., 2019). Previous research using the trauma film paradigm has primarily focused on the association between DT and the subsequent emergence of post-traumatic stress disorder (PTSD) symptoms, such as intrusive memories (e.g., Albanese et al., 2021).
Of note, researchers evaluating experimental outcomes across behavioral versus self-report measures have reported mixed outcomes (e.g., Hsu et al., 2023), leading some researchers to suggest that there may be a fundamental difference between one’s perceived ability to tolerate distress and their actual behavioral responses to stressful tasks (e.g., state distress levels). Thus, as recommended by Andrés and colleagues (2021), we examined distress tolerance as both a trait (e.g., the DTS) and state phenomenon (e.g., subjective distress levels) by analyzing SUDS reported while watching the trauma film paradigm to examine whether associations were consistent across both a trait- and state-assessment of DT. Additionally, while few studies have examined anxiety and depression symptoms to measure emotional responses to the film (e.g., Clark et al., 2015), there is a lack of research examining this task with symptoms from other internalizing disorders (e.g., social phobia, obsessive compulsive disorder [OCD], panic disorder [PD] symptoms).
Distress tolerance and internalizing psychopathology
Internalizing disorders encompass a range of emotional distress and symptom patterns in response to life stressors, representing the most common mental health problems during emerging adulthood (Bruffaerts et al., 2018; McLaughlin & Hatzenbuehler, 2009). DT is implicated in the etiology and maintenance of various internalizing disorders, including depression (Elhai et al., 2018), generalized and social anxiety (Laposa et al., 2015), PTSD (Banducci et al., 2017; Vujanovic & Zegel, 2020), OCD (Laposa et al., 2015), and PD (Yavari & Maroufi, 2022). These studies reveal that individuals experiencing greater difficulty in tolerating distress tend to exhibit higher severity of internalizing symptoms (Macatee et al., 2016; Ranney et al., 2022). However, previous research has primarily focused on examining individual disorders with trait DT separately (e.g., studying depression and DT, PTSD and DT), which siloes findings and interpretations. This separation can make it difficult to translate findings to clinical interventions, given that many individuals do not have only one diagnosis. While some studies have examined depression and anxiety together (e.g., Felton et al., 2017; Qi et al., 2019), they have predominantly not included other internalizing disorders, leaving gaps in our understanding of assessing internalizing psychopathology from an inclusive and transdiagnostic perspective. Given that internalizing disorders frequently co-occur at rates exceeding 50% during emerging adulthood (Eres et al., 2021), there is a push in clinical psychology to adopt a transdiagnostic approach that addresses multiple symptoms across diagnoses. By embracing this perspective, researchers and clinicians can better develop and implement intervention strategies that are tailored to individuals’ needs. Moreover, evidence suggests that improvements in one’s ability to tolerate distress are strongly associated with positive treatment outcomes for individuals with specific internalizing disorders (e.g., Banducci et al., 2017; Boffa et al., 2018). Thus, understanding which symptoms are most strongly associated with one’s capacity for tolerating distress can inform clinicians when to prioritize incorporating distress tolerance skills into treatment. Therefore, the current study attempted to address this gap in the literature by examining the association between a host of internalizing symptoms and distress tolerance. Further, we examined two forms of distress tolerance to assess if these associations were consistent across psychopathology (i.e., trait and state).
Emotion regulation, distress tolerance, and internalizing psychopathology
Deficits in emotion regulation (ER) are also recognized as a transdiagnostic risk factor, influencing the development and maintenance of various psychological disorders (Fernandez et al., 2016; Gratz & Roemer, 2004). The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004) has been extensively used as a self-report measure to assess emotion dysregulation. Numerous studies have shown a positive association between ER deficits and symptom severity across various internalizing disorders (Eichholz et al., 2020; Eres et al., 2021; Klemanski et al., 2017; Phillips et al., 2014; Strauss et al., 2019; Tull et al., 2020; Yap et al., 2018). Beyond psychopathology, difficulty tolerating distress has been associated with low ER ability (Jeffries et al., 2016; Van Eck et al., 2017). Moreover, ER and DT have been acknowledged as influential factors in how individuals respond to stressful situations. For instance, using unhelpful ER strategies (e.g., brooding, rumination; Lewis et al., 2018) or having difficulty tolerating distress (e.g., Buckner et al., 2019) has been individually linked to higher levels of state distress, measured by participants’ ratings (i.e., SUDS) of how nervous or stressed they felt before, during, and immediately after completing a stress-inducing task under experimental conditions. Thus, exploring their interrelationship across internalizing symptoms is crucial. Indeed, Van Eck and colleagues (2017) showed a positive association between higher levels of depression and anxiety symptoms and increased difficulties in tolerating distress and regulating emotions. However, there is a lack of information on the association between baseline ER and subjective distress levels (i.e., SUDS). Therefore, our study examined the potential moderating role of baseline ER in the relationship between internalizing symptoms and trait DT, as well as the association between internalizing psychopathology and subjective distress experienced during the trauma film paradigm.
Study aims
The current understanding of baseline internalizing symptoms and trait DT using a transdiagnostic perspective is limited. Further, there is no examination of how the association between baseline internalizing symptoms and distress differs by trait and state level. Moreover, few studies have examined the potential moderating role of ER between internalizing disorders and distress (assessed via trait DT and subjective distress). The present study investigated the relationships between baseline internalizing psychopathology, baseline ER, and both trait and state dimensions of DT in undergraduate college students, considering the significant burden of psychopathology (e.g., Lipson et al., 2019) and stress exposure (e.g., Karyotaki et al., 2020) during emerging adulthood. In this study, DTS (i.e., trait DT) was reverse-coded so that higher scores on the DTS indicated greater difficulty tolerating distress to be consistent with the direction of other measures used in the study (e.g., higher scores indicating greater severity in psychopathology and difficulty regulating emotions).
For Aim 1, our objective was to explore relationships between internalizing disorders (i.e., depression, general anxiety, PTSD, social phobia, panic disorder, and obsessive compulsive disorder) and trait DT. Given our explorative approach to examining transdiagnostic internalizing symptoms, ER, and DT, we employed forward stepwise linear regression modeling, a variable selection method that sequentially adds variables to the model based on their statistical significance. This approach, used in previous transdiagnostic studies (e.g., Linkas et al., 2022), is particularly suitable for exploratory analyses, as it aims to identify the strongest associations of an outcome while iteratively considering the contribution of each variable (as outlined by Braun & Oswald, 2011). Specifically, given the broad literature on depression, anxiety, and PTSD symptoms (Akbari et al., 2022; Brown et al., 1998; Macatee et al., 2016) with trait DT, we formulated two hypotheses. We hypothesized that 1a) all six internalizing disorders would be positively associated with trait DT, with depression, general anxiety, and PTSD symptoms having the most statistical contribution to distress tolerance. Additionally, considering the extensive body of literature linking greater difficulties with ER to greater deficits in trait DT (Jeffries et al., 2016), we hypothesized that 1b) greater difficulty in regulating emotions (baseline ER) would be associated with greater difficulty tolerating distress and would continue to have a substantial impact on distress tolerance scores even when considering internalizing disorders. We expected that all six internalizing disorders would maintain significant associations with trait DT, even after accounting for the influence of baseline emotion regulation ability.
For Aim 2, as Stanton and colleagues (2020) recommended, we conducted separate moderation analyses to explore the potential moderating role of baseline ER in the relationship between each internalizing disorder and trait DT. We hypothesized that individuals with greater difficulties in ER abilities would show a positive association between internalizing symptoms (i.e., depression, anxiety, social phobia, PTSD, PD, and OCD) and trait DT. That is, we expected individuals with higher DERS scores, reflecting worse ER abilities, to exhibit a stronger association between symptom severity for each internalizing disorder and trait DT than individuals reporting better ER abilities.
Lastly, for Aim 3, following similar guidelines as Aim 2, we explored the practical implications of our findings by investigating whether baseline ER moderated the association between each internalizing disorder listed above and subjective distress levels reported during the trauma film paradigm. Specifically, we anticipated a stronger positive association between each internalizing disorder and subjective distress levels among individuals with higher DERS scores, indicating poorer ER abilities, at each time point during the trauma film paradigm (anticipatory, peak, and end SUDS).
Method
Participants
One hundred sixty-six undergraduate college students participated, and 141 completed the study protocol. There were no exclusionary criteria. Of the sample, 104 were female and 37 were male. No participants identified as transgender, gender neutral, non-binary, or other. The mean participant age was 20.5 years (SD = 7.6), aged 18–41 years. Of these participants, 62% were non-Hispanic White, 19.7% were Hispanic/Latine, 7.3% were Asian, 2.2% were African-American/Black, <1% were Native American/Alaskan Native, <1% were Pacific Islander, and 7.3% identified as Other.
Measures
Distress tolerance
Distress tolerance scale (DTS)
The DTS is a 15-item self-report measure assessing an individual’s perceived ability to tolerate emotional distress, subjective appraisal regarding whether or not distress is seen as acceptable, level of attention absorbed by distressing emotions, and efforts taken to alleviate distress (Simons & Gaher, 2005). Participants rated each item (e.g., “When I feel distressed or upset, all I can think about is how bad I feel”) on a 5-point Likert scale that ranged from strongly agree (1) to strongly disagree (5). In the current study, we reverse scored the DTS, so that higher scores would indicate greater difficulty tolerating distress. The total DTS demonstrated excellent internal consistency (α = .92).
Subjective distress
Trauma film paradigm
We examined subjective distress levels using the trauma film paradigm. This paradigm involved presenting participants with distressing films depicting traumatic scenes, which has been employed in previous studies assessing DT (Holmes & Bourne, 2008; Olatunji & Fan, 2015). During the study, participants were instructed to watch a 5-minute film featuring graphic scenes of car accidents to evoke distress.
Subjective units of distress scale (SUDS)
SUDS is a common method of measuring self-reported subjective distress experienced by an individual (e.g., Bibb et al., 2015; Paz et al., 2017; Siegesleitner et al., 2019; Tonarely et al., 2020). The scale ranges from 0 “No distress; totally relaxed” to 10 “highest distress/anxiety you have ever felt,” with higher scores indicating increased levels of current distress. Prior research has suggested that scores between 0 and 6 are considered tolerable, while scores of 7 and above are considered highly distressing (e.g., Dal Molin, 2015). Distress was assessed before (e.g., anticipatory SUDS) and after (e.g., end SUDS) viewing the film, with participants also reporting the highest level of distress they experienced while watching the film (e.g., peak SUDS).
Internalizing symptom severity
Depression and anxiety
The Depression, Anxiety, and Stress Scale (DASS-21; Lovibond & Lovibond, 1995) is a 21-item scale used to measure symptoms of depression, anxiety, and stress over the past week. Each item is rated on a four-point Likert scale from 0 (Did not apply to me at all) to 3 (Applied to me very much or most of the time). The depression subscale (7 items) assesses symptoms such as anhedonia, hopelessness, and lack of interest. Scores of 0–9 are considered within the normal range, 10–13 indicate mild symptoms, 14–20 suggest moderate symptoms, 21–27 signify severe symptoms, and scores of 28 or higher represent extremely severe symptoms. Similarly, the anxiety subscale (7 items) measures symptoms including autonomic arousal, situational anxiety, and subjective experience of anxious effect. Scores of 0–7 fall within the normal range, 8–9 indicate mild symptoms, 10–14 suggest moderate symptoms, 15–19 signify severe symptoms, and scores of 20 or higher represent extremely severe symptoms. In the present study, similar to previous work (e.g., Larsson et al., 2022), the internal consistency was excellent for the depression subscale (α = .91) and good for the anxiety subscale (α = .85).
Social phobia
The Social Phobia Inventory (SPIN) is a 17-item scale designed to measure symptoms associated with social anxiety (Connor et al., 2000). The scale evaluates symptoms associated with social phobia including fear (of people, social events, and criticism), avoidance (of talking to strangers, large social gatherings), and physiological reactions (blushing, palpitations, and trembling). Each item is measured on five-point Likert scale, ranging from 0 (not at all) to 4 (extremely). The total score range is 0–68, with scores of 19 and above suggesting a possible diagnosis of social phobia. Internal consistency, similar to recent work with undergraduate college students (e.g., Fawwaz et al., 2022), for our sample was excellent (α = .92).
Obsessive compulsive disorder
OCD symptoms were measured using the Obsessive-Compulsive Inventory-Revised scale (OCI-R; Foa et al., 2002). The OCI-R is an 18-item self-report measure that assesses the distress associated with obsessions and compulsions, including washing, hoarding, and obsessing. Each item is rated on a five-point scale from 0 (Not at all) to 4 (Extremely). Scores range from 0 to 72, with scores of 21 or higher indicating likely presence of OCD. Internal consistency of the OCI-R is good among college students α = 0.88 (e.g., Hajcak et al., 2004), and was excellent in our sample α = .91.
Post-traumatic stress disorder
PTSD symptoms were measured via the primary care PTSD screen for the DSM-5 (PC-PTSD-5; Cameron & Gusman, 2003). The PC-PTSD-5 is a 5-item measure designed to assess if an individual has experienced a traumatic event over the course of their lifetime. The first item on the measure is designed to assess whether the participant has had exposure to traumatic events. If the respondent denies exposure, the PC-PTSD-5 is complete with a score of 0. If the answer is yes to this item, the respondent then answers five additional yes or no questions regarding PTSD symptoms over the past month. Each item answered with “yes” is considered a score of 1, with total scores of 4 or higher indicating probable PTSD. For the purposes of the present study, PTSD symptom scores were only included in analyses among participants who endorsed prior trauma exposure. Internal consistency has shown to be good in other samples α = .83 (e.g., Cheng et al., 2021). In our sample, internal consistency was acceptable, with α = .79.
Panic disorder
PD symptom severity was measured on the Panic Disorder Severity Scale (PDSS; Shear et al., 2001). The PDSS is a 7-item scale that measures psychopathology symptom severity associated with PD, specifically if the individual has experienced a panic attack in their lifetime. Each item is answered on a scale of (0–4), with higher scores indicating higher PD symptom severity in the participant’s lifetime (Furukawa et al., 2009). Total scores range from 0 to 28, with a score of 9 or above indicating probable diagnosis of PD. Internal consistency, similar to previous work with college students (e.g., Barber et al., 2020), for our sample was good, α = .88.
Difficulties in emotion regulation scale (DERS)
The DERS is an 18-item measure that examines different aspects of emotion regulation, such as emotional awareness, emotional clarity, goal-directed behavior, impulse control difficulties, non-acceptance of emotional responses, and limited access to ER strategies. Each item is answered on a five-point Likert scale ranging from 1 (Almost Never) to 5 (Almost Always). Scores range from 18 to 90, with higher scores indicating greater difficulties with emotion regulation. Of note, while there are no standardized clinical cutoffs for this measure, prior research suggests that the clinical range (i.e., emotion dysregulation; Gratz & Roemer, 2004) averages approximately 80–127 (Harrison et al., 2010; Staples & Mohlman, 2012). Internal consistency was good for our sample, similar to recent work with young adults (e.g., Lee & Arora, 2023), with a Cronbach’s alpha of α = .89.
Procedure
The present study was part of a larger study investigating the effect of evidence-based intervention strategies on individuals’ DT while completing distressing tasks (i.e., trauma film paradigm). Due to the COVID-19 pandemic, the study was administered remotely online on REDCap and conducted over Zoom with a trained undergraduate research assistant. Participants reported baseline levels of internalizing symptom severity, baseline ER (i.e., DERS), and trait DT (i.e., the DTS). We then measured subjective distress by having participants watch a distressing film (i.e., trauma film paradigm) and having them report their SUDS before and after watching the distressing film, as well as the maximum distress they experienced while watching the film. Participants provided written consent for course credit and were allowed to stop the study at any time during data collection without any repercussions. The University of Utah Institutional Review Board approved the present study. Individuals interested in the research materials and dataset can reach the principal investigator.
Data analytic approach
All analyses were conducted in SPSS version 29. We screened for missing data and removed 25 participants (N = 141). From 141 subjects, outliers were extracted (based on Q-Q plots, stem and leaf plots, and Shapiro–Wilk tests), and statistical analyses were conducted on a final 137 participants. Additionally, we conducted a power analysis using G-Power to estimate the required sample size for our study. Based on an alpha level of .05, power of .80, and a medium effect size (f2 = .15), the analysis indicated that a total sample size of 98 would be necessary to detect significant effects in our forward stepwise regression analyses. Therefore, our final sample size exceeded the required sample size to provide adequate statistical power.
For Aim 1, following the approach recommended by Stanton and colleagues (2020), we employed a forward stepwise linear regression to identify which internalizing disorders would be associated with trait DT (Hypothesis 1a). Then, we conducted a second stepwise linear regression to include baseline ER and internalizing psychopathology to observe which would be related to trait DT in the model (Hypothesis 1b). We assessed several assumptions for multiple regression, including the assumption of a linear relationship between the predictor and outcome variables, the normal distribution of errors, verification of homoscedasticity, and the independence of observations. Furthermore, to examine the potential issue of multicollinearity among the independent variables in our regression analyses, Variance Inflation Factor (VIF) values were computed. VIF values exceeding 10 are indicative of high multicollinearity, while values below 5 are generally considered acceptable (Alin, 2010). Our analyses revealed VIF values well below the threshold of 5 for all variables (range of 1.3–2.1), indicating that multicollinearity was not a concern in our regression models.
Aim 2 was examined using the HAYES Macro Process 4 in SPSS to explore the potential moderating role of baseline ER in the relationship between internalizing disorder symptoms and trait DT. For significant interactions, we conducted simple slopes analyses using ±1 standard deviation (SD) to better understand moderator effects. Similarly, for Aim 3, we conducted moderation analyses to assess the practical implications of our findings. Specifically, we explored whether ER influenced the association between internalizing symptom severity for each internalizing disorder and the subjective distress levels observed at three time points during the trauma film paradigm, measured by anticipatory, peak, and end SUDS. For Aims 2 and 3, interaction terms for internalizing symptoms, trait DT, and ER were created by centering each variable around the average score reported by our sample on their respective scales. Additionally, given the multiple comparisons involved in these analyses, we conducted post-hoc Bonferroni correction analyses to address any Type I error concerns. As we conducted six analyses, we set the significance level to .05/6 = .008.
Results
Descriptive statistics
Descriptive Statistics for Internalizing Symptom Severity, Distress Tolerance, Emotion Regulation, and State Anxiety.

Note. N = 137. PTSD analyses were limited to participants who reported prior exposure to at least one traumatic event (N = 74) as recommended by the PC-PTSD-5 scale. Participants without a history of traumatic experiences were not assessed for PTSD symptom severity.
PD = Panic Disorder.
OCD = Obsessive Compulsive Disorder.
SUDS = Subjective Units of Distress.
Aim 1: Internalizing psychopathology, ER, and trait DT
Baseline Internalizing Symptoms Predicting Trait Distress Tolerance.

Note. N = 137. Excluded internalizing symptoms: OCD, PD, and general anxiety symptoms. LL and UL indicate the lower and upper limits of a confidence interval, respectively.
For step 1, R2 = .34, F (1, 73) = 37.24, p < .001.
For step 2, R2 = .41, F (2, 73) = 24.57, p < .001.
For step 3, R2 = .46, F (3, 73) = 19.80, p < .001.
***p < .001.
*p < .05.
Baseline Internalizing Symptoms and Emotion Regulation Predicting Trait Distress Tolerance.

Note. N = 137. Excluded internalizing symptoms: depression, OCD, PD, and general anxiety symptoms. ER = Emotion Regulation.
For step 1, R2 = .40, F (1, 73) = 47.98, p < .001.
For step 2, R2 = .45, F (2, 73) = 28.54, p < .001.
For step 3, R2 = .49, F (3, 73) = 22.65, p < .001.
***p < .001.
*p < .05.
Aim 2: Baseline ER as a moderator between internalizing psychopathology and trait DT
Anxiety
The results revealed that the main effect of general anxiety symptoms (β = −0.019, p = .006) and baseline ER ability (β = 0.037, p = .00) were negatively and positively associated with trait DT, respectively, but were qualified by a significant positive interaction (β = 0.0010, p = .027). Simple slope analysis was conducted to probe the nature of the moderation effects. As seen in Figure 1, the line representing high ER abilities was steeper, indicating at high levels of ER ability, the impact of anxiety symptoms on trait DT was weaker. However, as anxiety symptoms increased, the influence of high ER ability diminished, corresponding with greater difficulty tolerating distress. However, the interaction between anxiety symptoms and baseline ER (p = .027), which was significant at the conventional alpha level of .05, did not meet the adjusted significant level after applying the Bonferroni correction (adjusted significance level = .008). Baseline Emotion Regulation as a Moderator Between Anxiety Symptoms and Trait Distress Tolerance. Note. Those with low ER ability showed greater differences in distress tolerance between those with low anxiety symptoms and those with high anxiety symptoms when compared to those with high ER ability. Trait DT = Trait Distress Tolerance. ER = Emotion Regulation Ability.
Depression
The main effect of depression symptoms was not significant (β = 0.013, p = .07), but baseline ER ability was positively associated with trait DT (β = 0.038, p < .0001), but these main effects were qualified by a significant positive interaction (β = 0.0007, p = .048). Consistent with anxiety, simple slopes (see Figure 2) indicated that for those with greater difficulty regulating emotions (e.g., higher scores on the DERS), there was a weak and non-significant association between depression symptoms and trait DT (β = 0.02, p = .71). On the other hand, among those with less difficulty regulation emotions (e.g., lower scores on the DERS), the positive relationship between depression symptoms and trait DT was significant (β = 0.003, p = .03). However, when depression symptoms increased, high ER ability was no longer a protective factor, associated with lower trait DT. Importantly, the interaction between depression symptoms and baseline ER ability, which was originally significant at the .05 alpha level (p = .048), did not meet the adjusted significance level after applying the Bonferroni correction (adjusted significance level = .008). Baseline Emotion Regulation as a Moderator Between Depression Symptoms and Trait Distress Tolerance. Note. Those with low ER ability showed greater differences in distress tolerance between those with low depression symptoms and those with high depression symptoms when compared to those with high ER ability. Trait DT = Trait Distress Tolerance. ER = Emotion Regulation Ability.
Panic disorder
PD symptoms (β = 0.0322, p = .021) and baseline ER ability (β = 0.39, p < .0001) were positively associated with trait DT but were qualified by a significant interaction (β = 0.0023, p = .018). The interaction plot showed that the association between PD symptom severity and trait DT was strengthened by higher ER abilities (see Figure 3). Further analysis of the simple slopes indicated that among individuals with greater difficulty regulating emotions, there was a weak and non-significant positive association between PD symptoms and trait DT (β = 0.0010, p = .95). In contrast, among individuals with low scores on the DERS (indicating better ER abilities), the positive relationship between PD symptoms and trait DT was significant (β = 0.06, p = .0049). This finding suggests that at high levels of ER ability, ER buffered the relationship between PD symptoms and trait DT when PD symptoms were low. However, as PD symptoms increased, ER was no longer a protective factor between high PD symptoms and deficits in one’s ability to tolerate distress. Additionally, contrary to hypothesis 2, the interaction between PD symptoms and baseline ER ability, which was originally significant (p = .018), did not meet the adjusted significance level after applying the Bonferroni correction (p = .008). Baseline Emotion Regulation as a Moderator Between Panic Disorder Symptoms and Trait Distress Tolerance. Note. Those with low ER ability showed greater differences in distress tolerance between those with low PD symptoms and those with high PD symptoms when compared to those with high ER ability. Trait DT = Trait Distress Tolerance. ER = Emotion Regulation Ability based on DERS scores. PD = Panic Disorder.
PTSD, social anxiety, and OCD
Contrary to hypothesis 2, the analysis revealed that baseline ER did not significantly moderate the associations between PTSD, social anxiety, and OCD symptoms with trait DT. Specifically, PTSD exhibited a significant main effect on trait DT (p = .0086), as did baseline ER (p < .0001), but these effects were not qualified by a significant interaction (p = .094). OCD exhibited a non-significant main effect on trait DT (p = .69), while baseline ER contributed a significant main effect (p < .0001), but these effects were not qualified by a significant interaction (p = .37). Similarly, social anxiety symptoms were not significant (p = .42), while baseline ER was significant (p < .0001), but effects were not qualified by a significant interaction (p = .13).
Aim 3: Baseline ER as a moderator between internalizing psychopathology and state distress
For Aim 3, we investigated the practical implications of our study by examining whether ER moderated the relationship between each internalizing psychopathology and state distress levels reported at different time points throughout the trauma film paradigm, including before (anticipatory SUDS), after (end SUDS), and the highest level of distress experienced during (peak SUDS).
Anticipatory distress
Consistent with the findings from Aim 2, our moderation analyses revealed that PD symptoms (β = 0.14, p = .0024) and baseline ER (β = −0.06, p = .0001) had a respective positive and negative main effect on anticipatory SUDS. Baseline ER significantly moderated the association between PD symptoms and anticipatory distress (β = −0.0068, p = .034). However, the significance did not meet the adjusted significance level after applying the Bonferroni correction (p = .008).
Depression (β = 0.07, p = .004), anxiety (β = 0.08, p = .0004), and social anxiety symptoms (β = 0.03, p = .034) demonstrated significant main effects on anticipatory SUDS. However, the main effects for PTSD symptoms (p = .67) and OCD symptoms (p = .32) were non-significant. Notably, baseline ER had a significant main effect on anticipatory SUDS across all 6 internalizing symptoms (ps ≤ .025). However, the interaction variables for these models were not significant (ps > .05).
Peak distress
Anxiety (β = 0.06, p = .011), OCD (β = 0.04, p = .027), and social anxiety (β = 0.04, p = .026) symptoms significantly influenced peak SUDS, while depression (p = .35), PTSD (p = .81) and PD symptoms (p = .07) were not significant. Baseline ER did not exhibit any significant main effects, ps ≥ .07. Lastly, no significant interactions emerged with peak SUDS as the dependent variable (ps ≥ .26).
End distress
Anxiety (β = 0.08, p = .002), OCD (β = 0.04, p = .039), social anxiety (β = 0.04, p = .024), and PD symptoms (β = .11, p = .043) significantly influenced end SUDS, whereas depression (p = .30) and PTSD (p = .56) did not have significant main effects. Moreover, baseline ER did not exhibit any main effects (ps ≥ .05). Similar to peak distress, no significant interactions were identified with SUDS as the dependent variable (ps ≥ .25).
The overall findings did not fully align with the predicted pattern of moderation. Notably, while we found indications that baseline ER exhibited moderation effects on PD symptoms and anticipatory SUDS at the conventional significance level (Figure 4), they did not withstand the Bonferroni correction. This underscores the need for further investigation to elucidate the role of ER in moderating the effects of internalizing symptoms on one’s perceived ability to tolerate distress. Baseline Emotion Regulation as a Moderator for Panic Disorder Symptoms and Anticipatory SUDS. Note. Those with low ER ability showed greater differences in subjective distress experienced in anticipation of completing the trauma film paradigm, measured using anticipatory SUDS, between those with low PD symptoms and those with high PD symptoms when compared to those with high ER ability. ER = Emotion Regulation Ability based on DERS scores. PD = Panic Disorder. SUDS = Subjective Units of Distress.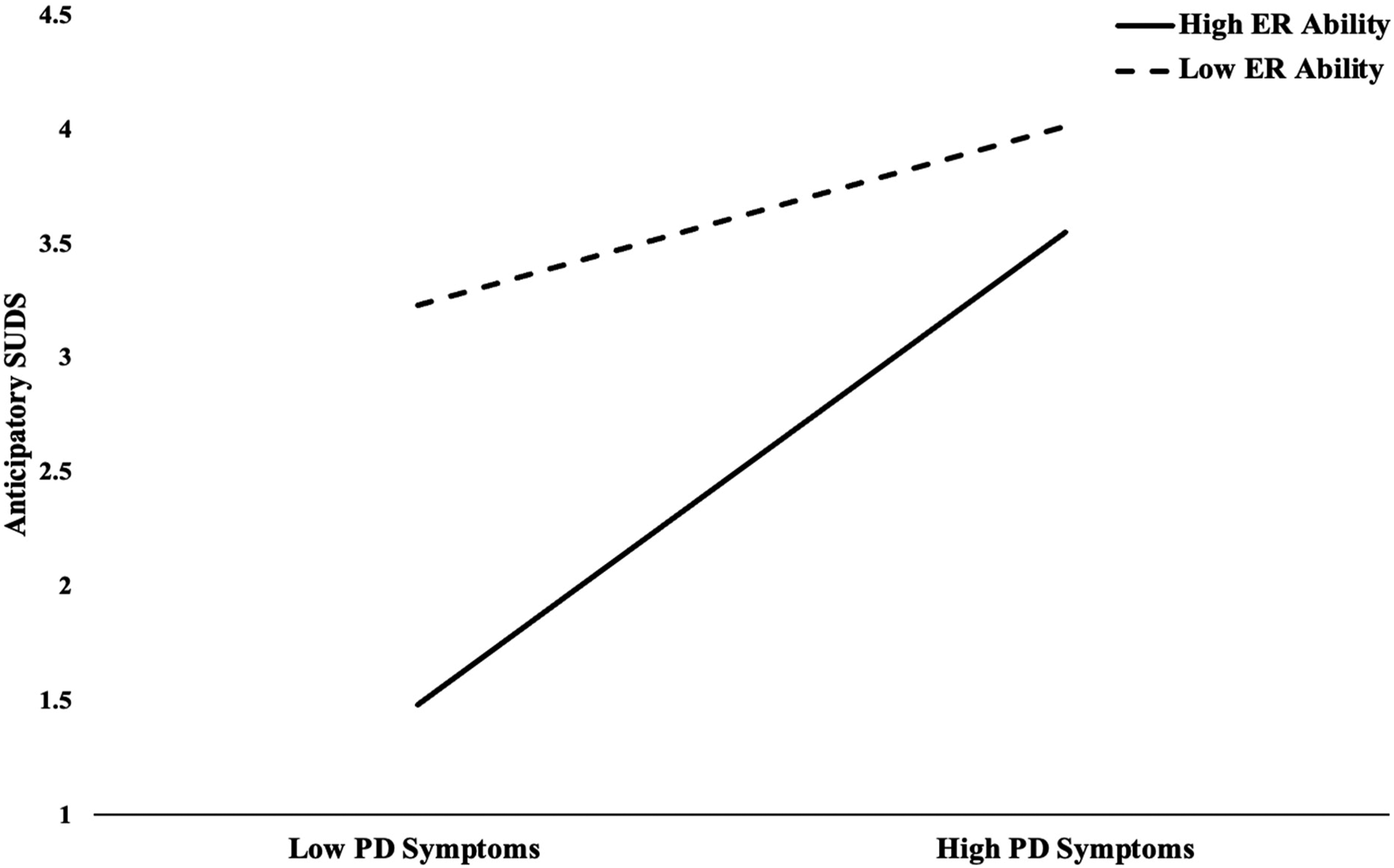
Discussion
Transdiagnostic approaches hold promise in addressing the limitations of the traditional categorical approach to internalizing disorders. Importantly, understanding how internalizing disorders relate to distress tolerance (DT) from a transdiagnostic perspective is critical in exploring how internalizing symptoms influence one’s perceived and behavioral capacity to tolerate distress, even when presenting symptoms from multiple disorders. Existing transdiagnostic literature has predominantly focused on depression and general anxiety symptoms and has not examined DT as both a trait and state phenomenon. The present study aimed to address these gaps in the literature by investigating the relationships between baseline internalizing psychopathology, baseline ER, trait DT, and state distress. Specifically, we examined the influence of several internalizing disorders using a transdiagnostic approach on trait DT, the moderating role of baseline ER on the relationship between internalizing symptoms and trait DT, and exploring practical implications by examining the moderating effect of baseline ER on the relationship between internalizing symptoms and state distress levels from the trauma film paradigm.
In Aim 1, depression symptom severity emerged as the initial variable positively associated with DTS scores, indicating a substantial influence of depressive symptoms on one’s perceived ability to tolerate distressing events even when other dimensions of internalizing symptoms were considered in the model. In the second step of the regression model, PTSD symptoms emerged as positively associated with trait DT. Notably, even after accounting for the influence of PTSD symptoms, depression remained significant, suggesting its independent contribution to one’s perceived ability to tolerate distress. This finding aligns with previous work showing that difficulty tolerating distress is associated with concurrent PTSD and depression symptoms (Holliday et al., 2016). However, at step three, depression was no longer significant when social phobia symptoms were introduced, supporting the limited research that has identified a significant positive relationship between social phobia symptoms and trait DT (e.g., Laposa et al., 2015). Notably, within the existing literature, no studies have examined baseline social phobia and depression symptoms concurrently in the context of trait DT among undergraduate populations. Although Yao et al. (2023) recently identified that baseline social phobia and depression symptoms related to trait DT in a Chinese population, it is important to note that their study examined trait DT as a mediating variable, with problematic social media usage as the outcome variable. They also used differing measures for assessing depression, social phobia, and trait DT compared to the methods in the current study. Further, Macatee and colleagues (2016) concurrently analyzed daily depressive and social anxiety symptoms measured across 6 days within an undergraduate sample. Their hierarchical regression model revealed that daily depression symptoms were linked to trait DT but not daily social phobia symptoms. This disparity in findings could be attributed to the difference in methodology, such as measurement of daily symptoms versus baseline symptoms. Further, these findings may be attributed to the nature of social phobia, which typically entails avoidance of external stimuli (e.g., social interactions), while depression often involves avoidance of internal stimuli (e.g., unpleasant mood and distress; Lass & Winer, 2020). It is important to acknowledge that our study’s findings may be driven by the elevated endorsement rates of social phobia symptoms and low rates of depression in our sample. Thus, future work examining depression, social phobia, and trait DT should prioritize samples characterized by elevated symptom severity in both domains to further assess current findings.
In the second model (hypothesis 1b), which included baseline ER alongside internalizing psychopathology, difficulty regulating emotions was associated with low self-perceptions of distress tolerance, aligning with prior expectations. This outcome aligns with previous literature demonstrating the connection between poor emotion regulation and reduced perceived ability to withstand distress (e.g., Conway et al., 2021; Jeffries et al., 2016). Moreover, present findings underscore the critical role of ER in understanding trait DT, even when accounting for internalizing symptoms. In partial support of hypothesis 1b, symptoms related to PTSD and social phobia remained significantly associated with trait DT even after accounting for the influence of baseline ER. This finding may indicate that these internalizing symptoms continue to influence trait DT directly, even when considering an individual’s ER abilities. While no previous transdiagnostic studies have simultaneously examined PTSD and social anxiety symptoms in the context of trait DT, both PTSD and social anxiety symptoms have been independently found to be related to trait DT as indexed by the DTS (Laposa et al., 2015; Marshall-Berenz et al., 2010). Given the inclusion of various internalizing symptoms in our analyses, our findings imply that from a transdiagnostic perspective, individuals coping with higher symptom severity associated with PTSD and social phobia may be particularly more likely to report feeling less able to cope with distress. Hence, individuals with elevated symptom severity related to social phobia and/or a history of traumatic exposure may especially benefit from interventions that enhance the perceived ability to tolerate distress, potentially mitigating the impact of distressing symptoms on daily functioning and overall well-being.
Aim 2 examined whether baseline ER was a moderator between internalizing disorders and trait DT. Our analysis indicated that baseline ER uniquely moderated the associations between depression, anxiety, and panic disorder (PD) symptoms, and trait DT when using the conventional significance level of .05. That is, our findings suggested that an individual’s ability to regulate their emotions may play a protective role in the relationship between internalizing symptoms and perceived ability to tolerate distress. Specifically, at low internalizing symptoms (i.e., low depression, anxiety, and PD symptoms), high ER ability buffered the adverse effects of these symptoms on trait DT in our sample. However, this ability to regulate emotions no longer served as a protective factor at higher internalizing symptom severity. Given the well-established link between self-perceived reduced capacity for tolerating distress and poor ER ability (e.g., Jeffries et al., 2016; Van Eck et al., 2017), researchers have suggested that promoting adaptive emotion regulation behavior among individuals with less perceived ability to tolerate distress may conversely help protect individuals against the harmful effects of stress (Larrazabal et al., 2022). Our results suggest that better ER abilities could serve as a buffer against the detrimental influence of specific internalizing symptoms (e.g., depression, anxiety, and PD symptoms) on how capable one perceives themselves in tolerating distress. Moreover, present findings suggest that individuals with higher ER abilities may report being more capable of tolerating distress, mitigating the negative impact of low internalizing symptoms on trait DT. However, this protective factor of ER weakens as internalizing symptoms (mainly depression, anxiety, and PD symptoms) become more pronounced. This finding may imply that even those with strong ER abilities might experience challenges in effectively coping with higher levels of internalizing symptoms and may benefit from interventions aimed at bolstering ER skills, which may also improve their perceived ability to tolerate distress. It is important to note that these associations did not meet the adjusted significance threshold following the Bonferroni correction, which was implemented to limit the risk of Type I errors, so we should interpret these findings cautiously.
Contrary to our expectations, moderating effects of baseline ER were not observed for social anxiety, OCD, and PTSD symptoms. While previous research has individually established direct links between OCD, PTSD, and social anxiety symptoms with perceived distress tolerance capacity (e.g., Laposa et al., 2015; Nargesi et al., 2018; Vujanovic & Zegel, 2020), our study examined the potential moderating role of baseline ER. The absence of significant interaction effects suggests that contrary to our expectations, one’s ability to regulate emotions did not influence the relationship between these specific internalizing symptoms and trait DT. While previous work has identified ER ability as a moderator between these specific disorders and various associated outcomes (e.g., Kim & Kwon, 2020; Mahoney et al., 2022; Mikonowicz & Tull, 2023), present findings suggest that this interaction may not extend to perceived capacity to tolerate stress as an outcome. It is important to consider that the findings pertaining to OCD and PTSD may have been influenced by the average symptom severity scores falling below the threshold for clinical diagnosis according to the respective scales (see Table 1). While average social anxiety symptom severity in our sample did meet the threshold for clinical diagnosis, replication in clinical and/or treatment-seeking samples is still needed to validate the consistency of these findings.
Our study also explored relationships among internalizing symptoms, baseline ER, and DT as a state phenomenon via subjective distress levels experienced at three distinct time points during the trauma film paradigm. Our predictions were partially supported, with ER moderating the association between PD symptom severity and anticipatory distress. However, we did not observe similar moderating effects for other internalizing symptom severities across the three distress time points. This result aligns with the well-established recognition of anticipation as a core feature of PD (e.g., DSM-5-TR; American Psychiatric Association, 2022; Helbig-Lang et al., 2012). Furthermore, even though the concurrent exploration of ER and DT within the context of PD is novel, prior research has demonstrated that ER can act as a protective factor, mitigating the link between risk factors for PD and the onset of PD symptoms during stress exposure (e.g., Kashdan et al., 2008). This finding underscores the potential role of ER as a safeguard between PD symptoms and subjective distress levels. On the other hand, the unexpected findings between other internalizing disorders and subjective distress levels may be attributed to several factors. Firstly, it is important to consider that our sample, on average, reported low levels of distress during the trauma film paradigm (see Table 1). This outcome may have been influenced by our study’s remote delivery, which differs from previous research using the trauma film paradigm. Similarly, our sample, on average, did not endorse high rates across all internalizing symptoms (see Table 1). Thus, future research should focus on treatment-seeking samples to explore potential relations between internalizing symptoms, ER, and DT. Finally, as mentioned previously, researchers evaluating experimental outcomes across behavioral versus self-report measures have reported mixed findings, leading some researchers to suggest that there is a fundamental difference between the perceived ability to tolerate distress (e.g., trait DT) and actual behavioral responses during an aversive task (e.g., subjective distress levels). For example, previous transdiagnostic work employing both measurements of DT found significant associations between internalizing psychopathology in clinical samples and self-reported DT (as indexed by the DTS). However, they found that behavioral DT measures (measured using the breath-holding and mirror tracing tasks) were unrelated to internalizing symptoms (Bernstein et al., 2011). This discrepancy may elucidate why we observed associations with DT when employing the DTS while not finding such associations with subjective distress levels as hypothesized.
The present study has several important strengths and limitations. One strength of this study is the transdiagnostic approach of internalizing symptoms and their relationship with trait DT. The study captures a broad range of psychopathologies and their impact on trait DT by including multiple internalizing disorders, measured using separate scales. This approach enhances generalizability by reflecting the complexity and comorbidity often observed in clinical populations. On the other hand, using cross-sectional data limits the ability to establish causality or examine temporal relationships between variables. Longitudinal designs would provide stronger evidence of the relationships and potential causal pathways. Moreover, it is important to note that this study relied solely on self-report measures for assessing internalizing symptoms, DT, and ER. Self-report measures are subject to biases and may not fully capture the complexity of these constructs (e.g., Pavlova & Uher, 2020). Using multiple assessment methods (e.g., clinical interviews and behavioral tasks) could enhance the validity of future findings.
Conclusion
Exposure to stress is linked to various mental health outcomes. This study used a transdiagnostic approach to investigate relationships between internalizing symptom severity on individuals’ perceived ability to cope with distress. Additionally, it is crucial to understand the unique associations of psychopathology with the perceived ability to tolerate distress. This understanding holds significance for developing and modifying evidence-based treatments that target transdiagnostic mechanisms (e.g., ER and DT abilities; Asnaani et al., 2020) and foster resilience against the adverse effects of co-occurring internalizing symptoms. Our findings indicate that among transdiagnostic internalizing symptoms, depression, PTSD, and social anxiety may exert a greater influence on self-perceptions of distress tolerance, with depression losing significance when accounting for baseline ER ability. Moreover, individuals with lower levels of specific internalizing symptoms (i.e., depression, anxiety, and PD symptoms) and stronger ER abilities may be more likely to counteract the negative impact of these symptoms on trait DT than those with higher symptomology and worse ER abilities. Furthermore, these findings suggest that this pattern might not apply to individuals’ behavioral capacity to manage distress. Overall, this research contributes to the evolving transdiagnostic framework, which attempts to better understand mechanisms, such as ER and DT, and their implications for contributing to and managing internalizing psychopathology.
Footnotes
Acknowledgments
We are very thankful for the team at the Treatment Mechanisms, Community Empowerment, and Technology Innovations (TCT) Lab (PI: Asnaani), especially Ifrah Majeed, Angela Pham, Ally Askew, Sami Soufi, Jasmine Moretz, and Rachel Cole for conducting the experiments and collecting data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.