
Abstract
Aims
Cognitive models propose that negative cognitive biases in attention (AB) and interpretation (IB) contribute to the onset of depression. This is the first prospective study to test this hypothesis in a sample of youth with no mental disorder.
Methods
Participants were 61 youth aged 9–14 years with no mental disorder. At baseline (T1) we measured AB (passive-viewing task), IB (scrambled sentences task) and self-report depressive symptoms. Thirty months later (T2) we measured onset of mental disorder, depressive symptoms and life events (parent- and child-report). The sample included children of parents with (n = 31) and without (n = 30) parental depression.
Results
Symptoms of depression at T2 were predicted by IB (ß = .35, p = .01) but not AB (ß = .05, p = .72) at T1. This effect was strongest for children who experienced multiple negative life events (F2,48 = 6.0, p = .018, ΔR2 = .08). IB did not predict depressive symptoms at T2 over-and-above the effect of depressive symptoms at T1 (ß = .21, p = .13).
Discussion
These findings suggest that IB (but not AB) plays an important role in the aetiology of depression. Modifying IB may have a preventive effect on youth depression, particularly for youth who experience negative life events. This prospective study provides important foundations for future experimental studies.
Introduction
The Prevalence of Depression
Major depressive disorder (MDD) is one of the most common mental disorders worldwide with a lifetime prevalence of around 8–12% (Andrade et al., 2003). It is also one of the largest causes of disability worldwide (World Health Organisation, 2017). Adolescence sees a surge in the prevalence of MDD: in a U.S. sample around 15% of adolescents experienced an episode of MDD by the age of 18 (Merikangas et al., 2010). Meta-analyses indicate that existing strategies to treat (Eckshtain et al., 2020; Zhou et al., 2015) and prevent (Hetrick et al., 2016) adolescent MDD have relatively modest effect sizes. Since adolescent MDD is a strong risk factor for adult psychiatric difficulties (Pine et al., 1999) and other adverse outcomes later in life (Clayborne et al., 2019), understanding more about the precise mechanisms underlying the development of youth MDD could have important implications for the prevention of MDD across the lifespan.
Cognitive Models of Depression
Cognitive models assume that cognitive biases, cognitive processes which are biased towards mood-congruent information, play a central role in the aetiology of depression (Beck & Haigh, 2014; Mathews & MacLeod, 2005). Cognitive biases are driven by both automatic and reflective processes (Beevers, 2005) and can occur at the level of attention, interpretation or memory (Mathews & MacLeod, 2005). For example, attentional bias (AB) refers to the tendency to systematically attend to negative stimuli and have difficulties disengaging attention from negative versus positive information. Interpretation bias (IB) in contrast refers to the tendency to consistently draw negative rather than positive or neutral interpretations about ambiguous information. Meta-analyses suggest that the difference between adults with and without MDD is of a moderate effect size for both AB (Peckham et al., 2010) and IB (Everaert et al., 2017).
Cognitive biases play an important role in integrative models of depression, which seek to explain the complex interplay between biological, cognitive and environmental risk factors in the aetiology of depression (e.g. Beck & Bredemeier, 2016). Cognitive biases for negative information may be influenced by biological vulnerabilities such as genetic polymorphisms and neurodevelopmental dysregulation (Beck & Haigh, 2014; Fox & Beevers, 2016) and/or arise from early life experiences (Beck & Haigh, 2014). Negative cognitive biases not only increase negative mood but also reinforce maladaptive schemata (Disner et al., 2011), contributing to the maintenance of depression. Importantly, cognitive biases are thought to remain latent unless activated by an external form of stress (Ingram et al., 1998).
Experimental and Prospective Studies of Cognitive Biases and Depression Risk
In adult samples mounting evidence suggests that AB and IB are not simply correlates or products of mood disorder but may play a causal role in the development of mood disorders. Experimental studies demonstrate that inducing negative cognitive biases increases negative mood (Mathews & Mackintosh, 2000; Mathews & MacLeod, 2002). These effects appear to persist for 24 hours and predict not only mood but also stress reactivity (Mackintosh et al., 2006). Importantly, training more benign AB (Browning et al., 2012) and IB (Hirsch et al., 2018) reduced the severity of symptoms of depression (from pre- to post-training) for those with a history of the disorder.
These experimental studies have been complemented by prospective studies, which have shown that undergraduate students with a stronger negative AB who also experienced more life stress were more likely to show elevated symptoms of depression or dysphoria seven weeks (Beevers & Carver, 2003) and five months (Sanchez-Lopez et al., 2019) later. In a sample which included adults who had previously experienced MDD, the strength of negative AB predicted mood states in the following seven days (Yaroslavsky et al., 2019).
Negative IB has also been found to prospectively predict the severity of symptoms of depression and onset of MDD in unselected adult samples (Kleim et al., 2014; Normansell & Wisco, 2017; Rude et al., 2002; 2003; 2010; Sugita & Yoshimura, 2022), although one study of unselected adults failed to replicate these findings (Wisco & Harp, 2021). More recent studies have found that positive (Kleim et al., 2014) and negative (Sugita & Yoshimura, 2022) baseline IB predicts later symptoms of depression over and above the effect of baseline depression symptoms. One study of undergraduate students found that composite scores of AB and IB predicted depressive symptom severity a year later (Everaert et al., 2015).
The role of Cognitive Biases in Youth Depression
Due to ongoing neural and social development during adolescence, findings from adult studies cannot be directly transferred to models of youth depression. Indeed, the role of cognitive biases may be stronger during childhood and early adolescence than it is during adulthood due to enhanced emotional sensitivity during adolescence (Paus et al., 2008) and/or because cognitive biases are an innate mechanism which decreases in value with age (Kindt & Van Den Hout, 2001). A number of cross-sectional studies (e.g. Buhl et al., 2023; Sfärlea et al., 2020) show that cognitive biases characterise youth with MDD (see Platt et al., 2017 for a review). Prospective studies to test whether and how cognitive biases have an impact on the aetiology of youth depression are crucial (Gibb et al., 2009; p. 424), particularly if more effective preventive interventions are to be developed. The CogBIAS study, which followed 504 unselected adolescents from 13 years through to 14.5 and 16 years, found that adolescents who showed an increase in symptoms of depression and anxiety across time also showed increases in negative IB and memory biases (Songco et al., 2020). IB also predicted psychological resilience (as defined by the number of symptoms of internalising disorder relative to the number of negative life events experienced) 12–18 months later (Booth et al., 2022). However, the latter effect was reduced to null when memory biases were included in the multi-variate model, potentially reflecting the overlap between IB and memory biases (e.g. Joormann et al., 2015). Whilst it is possible the findings reflect a stronger predictive role for memory biases, another longitudinal study of unselected adolescents found no evidence that memory biases predicted the severity of later depressive symptoms (Gutenbrunner et al., 2018). One explanation for the heterogeneous findings of these studies of unselected adolescents is the relatively low levels of cognitive vulnerability and depressive symptoms in their participants. Studies with adolescents at increased risk of depression may be better placed to assess the predictive value of cognitive biases in youth depression.
One prospective study found that children of depressed parents who also showed a negative AB were more likely to show heightened cortisol reactivity to stress later on, although the impact on symptoms of depression was not examined (Hayden et al., 2014). Another study of youth aged 9–14 years with an anxiety disorder found that an AB away from threat-related information predicted the severity of symptoms of depression two years later (Price et al., 2016). Similarly, a longitudinal study of children aged 7–10 years with high or low cognitive vulnerability found a significant (but diminishing) relationship between self-reported negative cognitions (not cognitive biases per se) and symptoms of depression 6, 18 and 30 months later in (Cole et al., 2011). Interestingly, in contrast to adult studies, the former study found no evidence that the relationship between cognitive style and depressive symptoms was moderated by stressful life events. In summary, although there are some early indications that cognitive biases prospectively predict the emergence of depressive symptoms in youth, to date no study has investigated whether they predict the onset of depressive disorder.
The Current Study
This study tested whether negative AB and IB prospectively predicted depression 30 months later in children aged 9-14 with no current or previous mental disorder. Children below the age of nine were not included because the tasks required adequate reading skills. Since the incidence of depression increases dramatically around 15 years of age (Hankin et al., 1998), 14 years was selected as the upper age limit. The period of 30 months was chosen for practical reasons and using our clinical judgement. We reasoned that sufficient time should have elapsed that a reasonable proportion of the sample had experienced stressful life events likely to trigger an episode of depression. At the same time, a delay of more than 30 months between testing sessions may have been associated with higher levels of drop-out. In order to maximise variability in depression risk at 30 months, we included children of depressed as well as non-depressed parents. Having a parent who has experienced depression themselves is one of the biggest risk factors for youth depression (Weissman et al., 2006). Furthermore, since we have previously shown that negative cognitive biases are elevated in children of parents with (versus without) depression (e.g. Sfärlea et al., 2019), including high-risk youth increased variability of cognitive bias scores. Since children of parents with (versus without) depression have also been shown to experience more negative life events (Hammen, 2002; Loechner et al., 2020), including high-risk youth enabled this interaction to be tested in our sample. Self-reported symptom severity was used as a continuous measure of depression whereas clinical diagnostic interviews conducted with children and their parents indicated the presence of absence of MDD (and other DSM-IV diagnoses).
A number of unique predictions were made about the findings of the study. Firstly, it was expected that negative IB would prospectively predict depression (the onset of an episode of MDD as well as elevated symptoms of depression) based on previous prospective studies of IB in adults (Everaert et al., 2015; Kleim et al., 2014; Normansell & Wisco, 2017; Rude et al., 2003; Sugita & Yoshimura, 2022). We also expected negative AB to prospectively predict depression based on previous studies of adults (Beevers & Carver, 2003; Sanchez-Lopez et al., 2019; Yaroslavsky et al., 2019) and children (Cole et al., 2011; Hayden et al., 2014; Price et al., 2016). Given that parental depression also predicts offspring anxiety (Weissman et al., 2016) and IB have been found to prospectively predict symptoms of youth anxiety (Henricks et al., 2022), we explored the extent to which cognitive biases in children of depressed parents predicted the onset of anxiety symptoms. Finally, in line with diathesis-stress models of depression (e.g. Goodman & Gotlib, 1999) and previous studies of adults (Beevers & Carver, 2003; Sanchez-Lopez et al., 2019), we expected a stronger link between cognitive biases and depression for youth who experienced more negative life events.
Methods
Study Design and Procedure
The present study was designed as a prospective follow-up to a cross-sectional study on attention and interpretation biases in children of parents with depression (Platt, 2017). Initial findings from the baseline assessment comparing cognitive biases in high- and low-risk children have been published elsewhere (Platt et al., 2022; Sfärlea et al., 2019). The participants included in the original study (T1; May 2016 to May 2017) were invited to participate in the follow-up assessment 30 months (M = 30.1, SD = 1.0) later (T2; November 2018 to November 2019).
All procedures were approved by the ethics committee of the Medical Faculty of the LMU Munich (Projects 441-15 and 18–661). Written informed consent was obtained from all participants and their parents after a comprehensive explanation of the study procedures. Participants had received a reimbursement of €50 per family for participation in T1 and received additional €35 for participation in the follow-up study.
After obtaining written informed consent, diagnostic interviews were conducted with participants and their accompanying parent(s). Afterwards, participants filled out questionnaires. A secondary aim of the study was to investigate the stability of cognitive biases over time therefore the questionnaires were followed by three tasks measuring cognitive biases. These findings are reported elsewhere (Sfärlea et al., in prep).
Participants
Characteristics of the study sample.

Note: Depression symptoms were assessed with the DIKJ; anxiety symptoms were assessed with the STAIC-T; negative life events represent the number of negative life events during the follow-up timespan assessed with CASE. 3
Psychopathology Assessment
Psychiatric diagnoses at T1 and T2 were assessed using a standardised, semi-structured psychiatric interview for children and adolescents (K-DIPS; Schneider et al., 2009). It was conducted with both participants and one of their parents, and composite diagnoses based on both versions were generated. The K-DIPS is a well-established German diagnostic interview that allows diagnosis of a wide range of psychiatric axis I disorders according to DSM-IV (American Psychiatric Association, 2000) with good interrater-reliability (accordance rates of at least 97% were reported for all diagnoses; Neuschwander et al., 2013). The interviews were conducted and evaluated by trained interviewers and interrater-reliability was determined for 20% (T1) or 25% (T2) of the sample by an independent researcher re-rating audio recordings of the diagnostic interviews. Accordance rates for lifetime diagnosis of MDD (pre-defined criterion) were 100%, for both T1 and T2 K-DIPS.
Self-reported depression symptoms of the participants were assessed with the German version of the Children’s Depression Inventory (DIKJ; Stiensmeier-Pelster et al., 2014) and self-reported anxiety symptoms were measured by the trait scale of the German version of the State Trait Anxiety Inventory for Children (STAIC; Unnewehr et al., 1992). Both questionnaires were administered at T1 as well as T2. Reliability of both self-report measures was excellent in our sample at both time-points (DIKJ: Cronbach’s α ≥ .83; STAIC-T: Cronbach’s α ≥ .86).
Life events
Positive and negative life events during the follow-up timespan were assessed at T2 using the Child and Adolescent Survey of Experiences (CASE; (Allen et al., 2012). This is a questionnaire assessing whether particular life events (e.g. ‘I made a good friend’ or ‘my parents split up’) occurred in the child’s life during a particular time period (in this case, the last 30 months). Life events that occurred are then rated as being experienced as positive or negative on a 6-point scale from ‘very pleasant’ to ‘very unpleasant’. Events that were rated as ‘rather pleasant’, ‘pretty pleasant’ or ‘very pleasant’ were counted as positive life events while events rated as ‘rather unpleasant’, ‘pretty unpleasant’ or ‘very unpleasant’ were counted as negative life events. Both the child and parent version of the CASE were administered. As number of negative life events were found to be predictive of depression symptoms (e.g. Loechner et al., 2020) these scores were used as indicators for negative life events in our study.
Cognitive Bias Measures
At T1, multiple measures were used for the assessment of AB and IB 2 (Platt, 2017; Platt, Sfärlea et al., 2022; Sfärlea et al., 2019). For this prospective analysis the measure that had shown the best psychometric properties in previous studies (Buhl et al., 2023; Platt et al., 2022; Sfärlea et al., 2019; 2020) was selected, that is, dwell time on sad faces in a Passive Viewing Task (PVT) as an indicator of AB and behavioural responses in the Scrambled Sentences Task (SST) as an indicator of IB. A meta-analysis identified the SST as a measure which overcomes some of the limitations of self-report measures (e.g. response and demand effects) and has particularly good psychometric properties (Würtz et al., 2022).
Attention Bias
Attention bias (ABs) were assessed by recording eye-movements during a PVT (similar to the task used by (Harrison & Gibb, 2015). Stimuli were coloured photographs of children’s faces displaying prototypical emotional expressions from the NIMH Child Emotional Faces Picture Set (NIMH-ChEFS; Egger et al., 2011). The task comprised 16 trials (corresponding to the minimum trial number suggested for eye-tracking research by Orquin and Holmqvist (2018) in which 2 × 2 stimulus arrays consisting of four photographs of the same model displaying a sad, an angry, a happy and a neutral facial expression (see Figure 1) were presented for 15,000 ms on a computer screen. Participants were instructed to freely view the stimuli with the only requirement being that they had to keep their attention on the screen. During the task, eye-movements were registered with an EyeLink 1000 Plus desktop-mounted eye-tracker (SR Research, 2013). Eye movement events were detected using a velocity and acceleration based saccade detection method with saccades defined as events with a velocity above 30°/s or an acceleration above 8000°/s2 (e.g. Skinner et al., 2018; Waechter et al., 2014). Gaze positions that were stable within 1° of visual angle for at least 100 ms were defined as fixations (in line with, e.g. Duque & Vázquez, 2015). To ensure adequate data quality, eye-tracking data of each participant were visually inspected for systematic calibration errors. Trials in which the total dwell time was less than 75% of the presentation time (due to excessive blinks, missing data or participants not looking at the screen; Skinner et al., 2018) were excluded. Subsequently, participants with less than 70% valid trials (Duque & Vázquez, 2015) and participants with systematic calibration errors were excluded from all analyses involving AB data (n = 3). Mean percentage of dwell time on sad faces was used as a measure for AB as it presented as an acceptable indicator of depression-related ABs in our previous studies (Buhl et al., 2023; Platt, Sfärlea et al., 2022) with Spearman-Brown-corrected split-half reliability of .69 at T1 (Platt et al., 2022). For additional details on the task see Platt et al. (2022) and Buhl et al. (2023). Passive-Viewing Task (PVT) to measure attention bias.
Interpretation Bias
Interpretation Bias (IB) were assessed using a computerised version of the SST (Everaert et al., 2014; Wenzlaff & Bates, 1998). The task involves participants unscrambling six words to form a grammatically correct sentence. Sentences had two possible solutions: one solution was positive (e.g. ‘I am a total winner’) whereas the other was negative (e.g. ‘I am a total loser’). Similar to earlier studies (e.g. Burnett Heyes et al., 2017; Everaert et al., 2014), a cognitive load procedure (recall of a 4-digit number) was included. Whilst performance in the SST is influenced by both automatic and reflective processes, the inclusion of a cognitive load procedure minimises response and demand effects common in self-report measures of IB (Würtz et al., 2022). The stimuli comprised 30 emotional (e.g. ‘total I winner a loser am’) scrambled sentences. Sentences were self-referential and targeted, for example, low mood, low self-esteem and negative thoughts about oneself and the future, which are typical cognitions in depression. Across the stimulus set, target words (the words in each sentence that accounted for the positive or negative solution) were matched for length and frequency in the German language. Word position within each sentence was randomised and whether the positive or negative target word was presented first was counterbalanced. The scrambled sentences were presented on a computer screen and participants were instructed to read the words, mentally form a grammatically correct five-word sentence as quickly as possible, and click on the mouse button as soon as they did so to continue to the response part of the trial. Sentences were presented for a maximum of 8000 ms; if no mouse click occurred during that time the response part was omitted and the next trial began. In the response part, participants were required to build the sentence they had mentally formed via mouse click (see Figure 2 for the trial procedure). Participants’ responses were rated as correct or incorrect and the correct sentences were categorised as positive or negative. Trials in which no grammatically correct sentence was built (time-out or incorrect sentence) were excluded. Two participants with severe reading difficulties that could barely perform the task as well as two participants that were identified as outliers in terms of accuracy (correct sentence rate of two SDs below the mean; Sfärlea et al., 2019) were excluded from all analyses involving IB. IB score was calculated as the proportion of negatively resolved sentences from the total number of correctly resolved emotional sentences (Everaert et al., 2014). Spearman-Brown-corrected split-half reliability at T1 was acceptable (.69; Sfärlea et al., 2019). See Sfärlea et al. (2019; 2020) for more details on the SST. Scrambled Sentences Task (SST) to measure interpretation bias.
Data Analysis
Statistical analyses were conducted with SPSS v25. To investigate our main hypothesis, that is, that cognitive biases predict depression prospectively, we performed two analyses. Firstly, a multiple logistic regression with presence of depression (yes/no; assessed via the diagnostic interview) by T2 as the outcome and AB and IB scores at T1 as predictors. Secondly, a multiple linear regression with self-reported depression symptoms at T2 as outcome and T1 AB and IB scores as predictors. To assess if the results were specific to depression, we repeated the analyses using the same predictors but replacing the onset of MDD with the onset of any mental disorder as the outcome of the logistic regression and the severity of depression symptoms with the severity of anxiety symptoms as the outcome of the linear regression.
To investigate the impact of negative life events on the relationship between cognitive biases and depression we performed moderation analyses using the PROCESS macro for SPSS (v. 4.1; Hayes, 2022), which uses ordinary least squares regression, yielding unstandardised coefficients for all effects. Bootstrapping with 5000 samples and heteroscedasticity consistent standard errors (HC3; Davidson & MacKinnon, 1993) were employed to compute inferential statistics and confidence intervals (CI). Separate analyses were run for AB and IB with T1 bias scores as predictors, T2 depressive symptoms as outcome and number of negative life events as moderator. Due to the only moderate correlation between child and parent reports of negative life events (r = .34), we decided to run separate analyses for child-reported negative life events and parent-reported negative life events.
For the linear regression and moderation analyses the IB scores were transformed using the Johnson transformation (Hemmerich, 2016; Johnson, 1949) in order to meet the assumptions of linear regression (i.e. linearity, homoscedasticity and normality of errors). One participant was identified as an outlier in the linear regression (according to Field, 2013) and thus additionally excluded from the linear regression and moderation analyses.
Results
Sample Characteristics
Of the 80 participants who took part in the T1 assessment, 61 (76%) took part in T2. A post-hoc power analysis revealed that the final sample size (n = 61) had a power of .75 to detect medium effects (R2 = .13) using 2-predictor regression models. The diagnostic interviews revealed that just six participants (9.8%; four high-risk and two low-risk youth) developed at least one mental disorder during the follow-up timespan. Four (6.6%) had experienced an episode of MDD, two (3.3%) developed social phobia, one (1.6%) had a specific phobia and one (1.6%) fulfilled criteria for post-traumatic stress disorder. A description of the sample at T1 and T2 can be found in Table 1.
Youth with high- versus low-risk of depression did not differ at T2 in depression or anxiety symptoms or child-reported negative life events (ts ≤ 1.1; ps > .1). They only differed in parent-reported negative life events with parents reporting significantly more negative life events for high-risk children (M = 4.6, SD = 2.8) than for low-risk children (M = 3.1, SD = 2.2; t55 = 2.2, p = .029). Regression and moderation analyses were therefore conducted across all participants. Exploratorily, analyses were repeated separately for youth with high- versus low-risk. Results of these analyses can be found in the Supplementary Material.
Do AB and IB predict depression at 30 months?
The two logistic regression models predicting onset of major depression (x 2 = 2.9, p = .238, Nagelkerke’s R 2 = .13) and onset of any mental disorder (x 2 = 1.7, p = .430, Nagelkerke’s R 2 = .061) at T2 by AB and IB at T1 were not statistically significant.
Results of the regression analyses predicting T2 depression symptoms as a function of T1 cognitive biases.
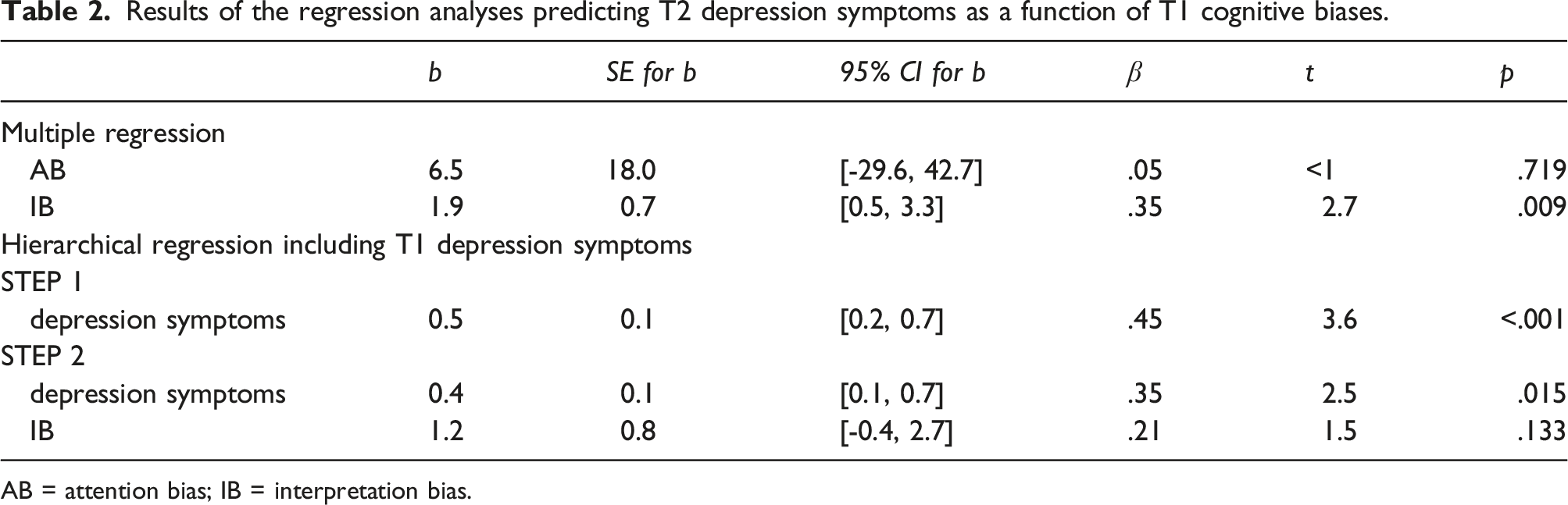
AB = attention bias; IB = interpretation bias.
In order to explore if T1 IB predicted T2 depression symptoms over and above T1 depression symptoms, we performed an additional hierarchical regression in which T1 depression symptoms were included as predictor in the first step and IB score added in a second step. 4 This analysis revealed that T1 depression symptoms accounted for a significant amount of variance (F1,51 = 12.8, p < .001, R 2 = .20) which was not significantly increased by the addition of IB (∆R 2 = .04; p = .133). See Table 2 for details on the predictors.
The linear regression with anxiety symptoms as outcome revealed that T1 AB and IB scores did not explain a significant amount of variance of T2 anxiety symptoms (F < 1, R 2 = .00).
Impact of Negative Life Events
As previously mentioned, due to the only moderate correlation between child and parent reports of negative life events, separate analyses for child- versus parent-reported negative life events were run.
5
Both moderation models with child-reported negative life events were non-significant (AB: F3,52 < 1, R
2
= .13; IB: F3,50 = 1.7, p = .174, R
2
= .13). The moderation model with T1 AB as predictor and parent-reported negative life events as moderator was also non-significant (F3,50 = 2.4, p = .074, R
2
= .10). However, the moderation model with T1 IB as predictor and parent-reported negative life events as moderator was significant (F3,48 = 3.6, p = .021, R
2
= .21). Parent-reported negative life events moderated the effect of T1 IB on T2 depression symptoms significantly (ΔR
2
= .08, F1,48 = 6.0, p = .018, b = 0.7, 95%-CI [0.1; 1.2]) with the relationship between T1 IB and T2 depression symptoms becoming stronger with an increasing number of negative life events. Figure 3 shows a Johnson-Neyman-Plot of this moderation effect (Hemmerich, 2022; Johnson & Neyman, 1936), indicating that the predictive effect of IB on depressive symptoms was significant for ≥ 4 negative life events. Johnson-Neyman-Plot of the moderation effect of parent-reported negative life events on the relationship between IB and depressive symptoms. When the moderator lies outside of the interval [0, 3.68], the effect of IB on depression symptoms is significant, p < .05. Figure created with Hemmerich, W. (2022).
Additional Analyses
The exploratory analyses repeating the regression and moderation analyses separately for high- and low-risk youth indicated that most effects were driven by the former (detailed results in the Supplementary Material).
We also performed exploratory t-tests to investigate if children and adolescents who developed an episode of MDD or any other mental disorder during the follow-up timespan differed in their AB and IB at T1. For the onset of MDD these analyses revealed no differences in AB (t < 1) but a trend regarding IB (t55 = 2.0, p = .050) with children and adolescents who developed an episode of MDD having shown more negative IB at T1 (M = .19, SD = .16) than children and adolescents who did not develop an episode of MDD (M = .09, SD = .09). For the onset of any mental disorder, these analyses revealed no differences for AB (t < 1) or IB (t55 = 1.4, p = .166).
Furthermore, since only 61 of the 80 participants of the T1 sample participated at T2 (i.e. 24% drop-out), we explored whether there was a systematic dropout depending on AB and IB: we compared T1 AB and IB between those who did participate in the follow-up study and those who did not. We found no difference for AB (t < 1) but a significant difference for IB (t21.5 = 2.1, p = .043): those who did not agree to participate in the follow-up study had a significantly more negative IB (M = .18, SD = .15) than those who did participate at T2 (M = .10, SD = .10).
Pearson-correlations between key study variables.

*p < .05; **p < .01; ***p < .001.
Discussion
Summary of Findings
This is the first study to investigate the extent to which cognitive biases prospectively predict the emergence of depression in youth with no mental disorder. Partially supporting our hypotheses, the severity of depressive symptoms (but not the onset of MDD) at 30 months was predicted by negative IB (but not AB). This effect was moderated by negative life events: negative IB only predicted symptoms of depression 30 months later for youth that experienced at least four negative life events during that time. There was no evidence that AB or IB predicted the severity of anxiety symptoms at 30 months.
Interpretation of Findings
Although we observed that youth who had an episode of MDD by T2 showed stronger IB (but not AB) at T1 than youth who did not encounter an episode of MDD, just 6.6% of the children and adolescents in our sample had experienced an episode of MDD 30 months later (9.8% had experienced any mental disorder). This contrasts with our expectations and previous studies. For example, one study found that 48% of high-risk youth experienced MDD within the 33 months after assessment (Beardslee et al., 2013), although this figure may be inflated by the inclusion of high-risk youth who themselves had a history of depression.
The finding that IB predicted later symptoms of depression was in line with our predictions and replicates previous findings in adults (Everaert et al., 2015; Normansell & Wisco, 2017; Rude et al., 2003) as well as adolescents (Songco et al., 2020), although it should be noted one study found no predictive role of IB (Wisco & Harp, 2021). Our findings also supplement experimental (e.g. Mackintosh et al., 2006) and prospective (e.g. Everaert et al., 2015) studies which suggest a causal role of IB in the aetiology of depression. However, it should be noted that a number of alternative pathways may explain the findings. For example, negative IB may have contributed to depression at T1, which in turn predicted depression at T2. Alternatively, IB may be the product of depression, which is why IB did not predict later symptoms of depression when baseline symptoms were taken into account. The latter finding of course demonstrates that previous depression may be a stronger predictor of future depression than IB. However, since IB (in contrast with depressive symptoms) is directly modifiable, it is a relevant predictor worth considering in future experimental studies and clinical trials.
The finding that the association between IB and later depressive symptoms was greater for those who experienced more negative life events replicates studies in adults (Beevers & Carver, 2003; Sanchez-Lopez et al., 2019) and taken together, these findings support diathesis-stress models of depression where it is argued that individuals who have cognitive biases and experience environmental stress have the highest levels of depressive symptoms. It has to be noted, however, that only parent- but not child-reported negative life-events were found to moderate the relationship between IB and later depressive symptoms. This may be due to children and adolescents having difficulties remembering exactly at what time certain events happened and so their report being less objective or due to parents with a history of depression’s particular focus on negative live events with may have led to them over-reporting negative life-events in their children’s lives.
The finding that negative AB did not predict the severity of depressive symptoms at 30 months is surprising, given the findings of previous prospective studies of adults (Beevers & Carver, 2003; Sanchez-Lopez et al., 2019; Yaroslavsky et al., 2019) and children (Hayden et al., 2014; Price et al., 2016). Given previous studies which have shown associations between AB and IB (e.g. Everaert et al., 2014) it was also surprising that we found no correlation between AB and IB. These findings might represent floor-effects in our sample: due to the resilience of our sample (as indicated by the relatively low number of MDD episodes at follow-up), relatively few offspring had a strong negative AB at baseline. Since negative AB is stronger in depressed versus non-depressed youth (Buhl et al., 2023) but does not differ between high- and low-risk youth (Platt, Sfärlea et al., 2022), an alternative explanation is that AB is a consequence rather than risk factor for youth depression. However, a number of methodological differences between our study and previous prospective studies of AB are also worth considering. For example, in the only previous study to prospectively predict the effect of AB on depressive symptoms in youth, participating children had an anxiety disorder (Price et al., 2016). All three studies of adults have included relatively short follow-up periods and measured AB in response to a stressor (Beevers & Carver, 2003; Sanchez-Lopez et al., 2019; Yaroslavsky et al., 2019). It should be noted that at least one other study also has failed to find a predictive role for AB on later depressive symptoms (Johnson et al., 2007). Finally, since the effect size of AB is relatively small, it is possible that our sample size was under-powered to detect AB. Indeed, post-hoc power analysis revealed that the sample size at T2 had a power of .75 to detect medium effects (R2 = .13) using 2-predictor regression models. This is below the standardly accepted power of .80. As such, these findings require replication in larger samples to test the reported models.
Strengths and Limitations
A strength of the study design is the psychometric properties of the measures we used to assess cognitive biases and depression. We complemented self-reported questionnaire measures of depression with validated clinical interviews which showed particularly high inter-rater reliability in this sample. Clinical interviews are generally preferable over self-reported measures of depression, although unfortunately the interpretation of these data in our sample was limited by the low prevalence of MDD. The measures of cognitive bias were selected based on their psychometric properties in previous studies and the superior qualities of the SST have recently been confirmed in a meta-analysis (Würtz et al., 2022). Minor limitations of the tasks used in our study include the fact that we did not collect information on the valence and arousal associated with the stimuli in the PVT and did not measure accuracy of recall in the cognitive load procedure of the SST.
A second strength of the study design is the long follow-up period (30 months; 2.5 years). Whilst many previous studies have investigated the predictive role of cognitive biases on depressive symptoms over periods of days (Yaroslavsky et al., 2019), weeks (Beevers & Carver, 2003) or months (Sanchez-Lopez et al., 2019), very few (Price et al., 2016; Songco et al., 2020) have included such a long follow-up time period. This also enables more valid conclusions to be drawn about the longer-term impact of negative cognitive biases on psychopathology. Future studies with larger samples might consider even longer follow-up periods into late adolescence (15–18 years), particularly if they are investigating unselected samples of youth. A recent meta-analysis suggested that just 2.5% of unselected youth experience an episode of mood disorder by the age of 14 and the peak age of onset for mood disorders is 20.5 years (Solmi et al., 2022).
The main limitations of the study relate to the representativeness of the sample. Firstly, there was evidence of systematic drop-out at T2: the participants who took part were less likely to have a negative IB at baseline than those who did not. This may explain the low number of participants who had developed MDD and other mental disorders by T2: those with a more negative IB presumably also had more depressive symptoms at T1 and were more likely to develop depression or other mental disorders. In addition, the low proportion (13%) of high-risk children who developed mental disorder during the follow-up period indicates they may have been psychologically resilient. This may be because some were recruited via a study of a family- and group-based preventive intervention. Although the majority of high-risk participants in this sample (66%) had not received the intervention by T2, their willingness and desire to participate may reflect their psychological resilience. Whilst these issues of representativeness influence the generalisability of the findings, it is likely that our findings are an underestimate (rather than overestimate) of the true effect size.
Future Studies and Clinical Implications
The strength of the effect of IB on symptoms of depression suggests IB may be a vulnerability factor worth targeting in targeted preventive interventions. Cognitive bias modification of interpretations (CBM-I) has found to be effective at reducing stress reactivity in adults with MDD (Joormann et al., 2015) and symptoms of depression in unselected young adults (Nieto & Vazquez, 2021) as well as being a feasible as a means of preventing relapse in adults discharged from psychiatric treatment (Beard et al., 2021). Although many successful cognitive-behavioural interventions for the prevention of youth depression have included interpretation training elements (Loechner et al., 2018), to date little is known about the unique preventive effect that training IB specifically may have for youth at risk of depression. One ongoing study seeks to test the effects of a cognitive bias modification of interpretation (CBM-I) intervention on stress reactivity in high-risk children (Frommelt et al., 2023). Although other studies have shown cognitive bias modification of attention (CBM-A) to have potential in the prevention of depression (Browning et al., 2012), this study suggests that targeting AB is unlikely to have an effect on risk of depression in youth.
Whilst training IB may be a promising means of preventing youth depression, the findings regarding negative life events suggest that one should not overlook the substantial role that adverse life events play in the aetiology of youth depression. Alongside psychological interventions, public health interventions and political structures to reduce children’s exposure to adverse life events are also of paramount importance.
Summary
This study is the first to test whether cognitive biases in attention and interpretation prospectively predict the onset of depression in youth with no mental disorder. Understanding precisely how known vulnerability factors interact to predict the onset of depression in offspring is important given that existing preventive interventions for children of depressed parents show relatively modest effects (Loechner et al., 2018). In a sample of 61 children and adolescents we found evidence that IB (but not AB) at age 9–14 years predicted depressive symptoms 30 months later. This finding suggests that interventions which modify IB may be worthy candidates for depression prevention, particularly for youth with an elevated risk of negative life events or depression. Whilst this prospective study provides important foundations for investigating the causal role of IB in youth depression, experimental studies which train more benign IB in at-risk youth and measure their effects on depression risk are a necessary next step.
Supplemental Material
Supplemental Material - The role of cognitive biases and negative life events in predicting later depressive symptoms in children and adolescents
Supplemental Material for The role of cognitive biases and negative life events in predicting later depressive symptoms in children and adolescents by Belinda Platt, Anca Sfärlea, Johanna Löchner, Elske Salemink, and Gerd Schulte-Körne in Journal of Experimental Psychopathology
Footnotes
Acknowledgements
We thank Laura Asperud Thomsen, Moritz Dannert, Finja Gerlach, Veronika Jäger, Linda Lukas, Jakob Neumüller, Lisa Ordenewitz, Amanda Sommerhoff, Kornelija Starman-Wöhrle, Ann-Sophie Störmann and Petra Wagenbüchler for their help with participant recruitment and data collection. We thank Keisuke Takano for his suggestions regarding analyses. Furthermore, we thank all families who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the LMU Gender Mentorung Prorgramme, Hans und Klementia Langmatz Stiftung; ‘Förderprogramm für Forschung und Lehre’ of the Medical Faculty of the LMU; 895.
Supplemental Material
Supplemental material for this article is available online.
Notes
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.