
Abstract
Emotion dysregulation, including higher baseline emotional intensity and emotional reactivity (i.e., increased magnitude of change in emotional responding) is theoretically central to Borderline Personality Disorder (BPD). However, little research has examined which specific emotions individuals with BPD experience emotion dysregulation in. Interpersonal problems also theoretically drive emotion dysregulation in BPD. However, whether interpersonal problems elicit emotion dysregulation for some specific emotions but not others is unclear. This study aimed to assess whether interpersonal problems moderate the relationship between (1) baseline emotional intensity and (2) emotional reactivity in BPD across six specific emotions (i.e., sadness, disgust, fear, shame, guilt, and anger). Borderline Personality Disorder (n = 30) and healthy control (HC; n = 30) groups reported their interpersonal problems at baseline and their emotions before and after listening to a laboratory stressor. For the BPD (but not HC) group, higher interpersonal problems were associated with greater baseline sadness, disgust, fear, shame, and guilt. Across groups, higher interpersonal problems were associated with greater sadness, fear, guilt, and anger, but not disgust, reactivity. Higher interpersonal problems were associated with higher shame reactivity specifically for those with BPD. Targeting interpersonal problems may reduce heightened baseline emotional intensity and emotional reactivity for those with BPD, particularly for shame reactivity in BPD.
Keywords
Introduction
Borderline Personality Disorder (BPD) is a life-threatening disorder that impacts approximately 1.6% of the international population (Ellison et al., 2018). Approximately 90% of people with BPD report engaging in self-injurious behavior (Goodman et al., 2017) and research has found that approximately 6% of those with BPD die by suicide (Temes et al., 2019). Leading theories of BPD suggest that all BPD symptoms are directly or indirectly accounted for by emotion dysregulation (ED; Linehan, 1993), or purport that emotion disruption is a central component of the disorder (Sauer-Zavala & Barlow, 2014; Selby & Joiner, 2009). Linehan (1993) suggests that ED is comprised of disruptions in both emotional processing and difficulty regulating emotions. Disrupted emotional processes in ED include heightened baseline emotional intensity, heightened sensitivity to emotional stimuli, heightened emotional reactivity (i.e., larger increases in emotion from baseline following emotional stimuli), and a slow return to baseline (i.e., slower decreases to baseline following emotional stimuli; Linehan, 1993). Although all of these emotional processes have been studied in BPD (e.g., Chapman et al., 2015; Daros et al., 2018; Elices et al., 2012; Gratz et al., 2010; Scheel et al., 2013), baseline emotional intensity and emotional reactivity have understandably received the most empirical attention. Indeed, heightened emotional reactivity is a diagnostic criterion of BPD that elicits high distress and impairment across multiple domains (e.g., interpersonal, occupational), and is therefore an explicit treatment target in BPD interventions APA, 2022), warranting a high degree of empirical scrutiny. Moreover, many emotion dysregulation components including emotional reactivity inherently require the assessment of baseline emotional intensity, increasing its prevalence in ED research. As well, heightened baseline emotional intensity and emotional reactivity are associated with elevations in BPD symptoms (Gratz et al., 2008). Therefore, identifying what individual characteristics modulate these emotional processes and can be targeted in BPD treatments is imperative to reducing ED in BPD, thereby optimizing treatment outcomes. Recent theories illustrate that interpersonal problems (e.g., relationship conflict, problematic communication between individuals with BPD and their significant others) exacerbate emotional reactivity in BPD (e.g., Fitzpatrick et al., 2021; Fruzzetti & Fantozzi, 2008). Since interpersonal problems are suggested to contribute to the development and maintenance of BPD symptoms such as emotional reactivity (e.g., Dixon-Gordon, Yiu et al., 2013), targeting them in treatment may accordingly enhance treatment response. The present study will therefore empirically test whether interpersonal problems influence baseline emotional intensity and emotional reactivity in BPD.
Baseline emotional intensity and emotional reactivity
Although some studies suggest that BPD and control groups do not differ in baseline emotional intensity (e.g., Elices et al., 2012), several studies suggest that individuals with BPD exhibit elevated baseline emotional intensity compared to healthy and clinical controls across multiple emotion domains, including self-report (e.g., Ebner-Primer et al., 2007; Gratz et al., 2010), parasympathetic emotion indices such as respiratory sinus arrhythmia (e.g., Feliu-Soler et al., 2013; Kuo et al., 2016; Kuo & Linehan, 2009), and sympathetic emotion indices such as skin conductance responses (e.g., Ebner-Primer et al., 2007; Kuo & Linehan, 2009). However, there remains some variability with respect to whether and which specific emotions comprising baseline emotional intensity are heightened in BPD. For example, studies have specifically highlighted that BPD involves elevations in baseline disgust, shame, guilt, anxiety, annoyance, anger, and sadness, but not boredom, and mixed results regarding positive emotions, relative to control groups (Ebner-Priemer et al., 2007; Jacob et al., 2008; Scheel et al., 2013). These findings suggest that most, but not necessarily all, specific emotions may be elevated at baseline in BPD.
Research on emotional reactivity in BPD is more equivocal. Some studies suggest that BPD and high BPD symptoms involve heightened self-reported and sympathetic activity (e.g., heart rate, skin conductance response) indicative of heightened emotional reactivity compared to HCs and those with low BPD symptoms (e.g., Chapman et al., 2015; Dixon-Gordon, Yiu et al., 2013; Ebner-Priemer et al., 2005; Rosenthal et al., 2016), but other studies do not (e.g., Dixon-Gordon et al., 2015; Gratz et al., 2019; Kuo & Linehan, 2009). Data on emotional reactivity in BPD may be mixed given that those with the disorder may exhibit emotional reactivity of specific emotions, but not others. For example, Chapman et al., (2015) examined emotional reactivity to a social rejection stressor versus a frustrating math task and found that those with higher BPD symptoms experienced significantly higher shame reactivity (but not irritability or hostility) during the frustrating math task and significantly higher hostility reactivity (but not irritability or shame) in the social rejection condition compared to controls. Those with high BPD (compared to low BPD) features also reported significantly higher upset, fear, and hostility reactivity following a fear inducing stimulus (Chapman et al., 2013), yet groups did not differ significantly in guilt, shame, nervousness, distress, irritability, or jittery emotional reactivity. Furthermore, in a study by Reichenberger et al. (2017), those with BPD and HCs were presented with interpersonal videographic stimuli in which actors presented rejecting, neutral, or appreciative sentences and were asked to report on specific emotions before and after the stimuli. Findings showed that those with BPD experienced a decrease in pleasant emotions and an increase in anger, anxiety, embarrassment, contempt, guilt, sadness, and feelings of disapproval/rejection following negative interpersonal stimuli, as well as a decrease in pride, happiness, feelings of approval, and attraction/love following positive interpersonal stimuli compared to the control group.
Taken together, these findings suggest that heightened emotional reactivity in BPD may not be pervasive but rather emotion-specific, and that emotionally specific reactivity may vary depending on the induction used to elicit it. However, much of this research measures baseline emotional intensity and emotional reactivity as a general negative emotional composite (e.g., Dixon-Gordon, Gratz et al., 2013; Elices et al., 2012; Rosenthal et al., 2016), which may obfuscate these emotion-specific effects. Additional research is needed to disentangle which specific emotions involve heightened baseline emotional intensity and emotional reactivity in BPD. Elucidating which emotions are most intense at baseline and more likely to increase following emotionally evocative stimuli (i.e., reactivity) will better inform which emotions require targeting, and when (e.g., at rest, or following a stressor), in BPD treatments.
Interpersonal problems and borderline personality disorder
In addition to varying across specific emotions, baseline emotional intensity and emotional reactivity may vary in BPD according to specific individual characteristics. Such unaccounted for variability may account for the mixed findings in the emotional reactivity literature. Most notably, BPD is characterized by interpersonal problems—an individual characteristic that may influence emotion dysregulation difficulties and, if unaccounted for, may result in mixed ED findings in the disorder. Interpersonal problems in BPD include volatile relationships and a fear of abandonment, and research has found that relationships of those with BPD are characterized by more conflict, dissatisfaction, and dissolution compared to those of controls (e.g., Bouchard et al., 2009; Hill et al., 2008; Hill et al., 2011; Lazarus & Cheavens, 2017).
Linehan’s Biosocial Model (1993) suggests that invalidating interpersonal relationships transact with biological vulnerabilities to dysregulate emotional processes overtime to elicit ED. Thus, interpersonal problems may not only be a consequence of ED but rather one of ED’s causal factors. Fruzetti and Fantozzi (2008) extended Linehan’s Biosocial Model (1993) to couples wherein one member has BPD and postulate that people with BPD often inaccurately express their emotions. As a result, partners may invalidate the emotional experience of their loved one with BPD, leading to conflict, destructive behaviors, and invalidation, further exacerbating ED over time. More recently, Fitzpatrick et al. (2021) posited that interpersonal problems may reciprocally interact with disrupted emotional processes in BPD, thereby exacerbating one another over time and leading to other BPD symptoms (e.g., self-injury). This theory is particularly explicit in emphasizing the role of interpersonal problems not only as a causal but also maintenance, factor of ED in BPD.
Together, these theories indicate that individual variability in interpersonal problems may influence the extent to which people with BPD become emotionally dysregulated, whereby those with more interpersonal problems may exhibit higher baseline emotional intensity and emotional reactivity compared to those with fewer interpersonal problems. Indeed, a growing body of research suggests that interpersonal problems and ED are related in those with BPD and high BPD symptoms (e.g., Barnow et al., 2009; Chapman et al., 2015; Dixon-Gordon, Yiu et al., 2013). Notably, studies suggest that heightened emotional reactivity in BPD may be specific to interpersonal stimuli, such that those with BPD or high BPD features exhibit heightened emotional reactivity in response to interpersonal stressors compared to non-interpersonal ones (e.g., Limberg et al., 2010; Sauer et al., 2014). For example, Sauer et al. (2014) found that people with BPD had significantly higher emotional reactivity compared to both HCs and those with Major Depressive Disorder in response to sexual abuse and interpersonally-themed images, but not self-injurious/suicidal behavior or trauma-themed images. Furthermore, a study by Limberg et al. (2010) showed that stimuli depicting rejection and abandonment elicited greater physiological reactivity from patients with BPD compared to HCs. Conversely, there were no significant differences between groups in heightened physiological reactivity for survival threat, neutral, or pleasant (e.g., relaxation) stimuli. These studies suggest that ED processes like emotional reactivity may be particularly salient in the context of interpersonal stress. Moreover, as higher general distress and mental health problems are associated with poorer interpersonal functioning (e.g., McConnell et al., 2016; Segrin et al., 2015; Whitley et al., 2016), baseline emotional intensity and interpersonal problems are also likely to be associated. Accordingly, individuals with BPD with higher interpersonal problems may be more likely to exhibit worse ED than those with lower interpersonal problems.
Although research suggests that interpersonal stressors may be more likely to elicit ED in those with BPD than non-interpersonal ones, the moderating effect of one’s own level of interpersonal problems—rather the extent to which an emotion induction is interpersonal versus not—is yet to be tested. Such information is important because, unlike the qualities of an external stressor, interpersonal problems represent a meaningful clinical target that could be addressed in treatment to reduce ED and improve BPD treatment outcomes. Accordingly, Dixon-Gordon, Yiu et al. (2013) found that higher interpersonal dysfunction mediated the positive relationship between BPD features and sympathetic emotional reactivity, but not self-reported emotional reactivity. However, no research to our knowledge has examined whether interpersonal problems moderate baseline emotional intensity or emotional reactivity in those with BPD diagnoses, or whether the effects of interpersonal problems on baseline emotional intensity and emotional reactivity are emotion-specific in BPD. Research suggests that specific emotions (e.g., shame, embarrassment, jealousy, and guilt) may be more interpersonally linked than other emotions given that they require feedback (i.e., thoughts, feelings, and behaviors) from other people (Hareli & Parkinson, 2008). Baseline emotional intensity and emotional reactivity of “social emotions” such as shame and guilt may therefore be particularly heightened for individuals with BPD who have high interpersonal problems. However, this remains an open empirical question.
Aims of the present study
Building on these empirical gaps, this study uses data collected as part of a larger experimental study that examined emotional processes in BPD (Fitzpatrick et al., 2019) to examine (1) whether interpersonal problems moderate the relationship between group (i.e., BPD and HCs) and baseline emotional intensity across specific emotions (i.e., shame, guilt, anger, disgust, fear, and sadness), and (2) whether interpersonal problems moderate the relationship between group and emotional reactivity across the same specific emotions (see Figure 1, for overview of study and research questions). Given the reviewed literature (e.g., Chapman et al., 2015; Fitzpatrick et al., 2021; Gratz et al., 2010; Hareli & Parkinson 2008; Sauer et al., 2014), we hypothesized that individuals with BPD who have higher levels of interpersonal problems would exhibit higher levels of baseline emotional intensity and emotional reactivity in response to social emotions of guilt and shame specifically, but not necessarily other emotions (i.e., anger, disgust, fear, and sadness), compared to HCs. Visual depiction of study design.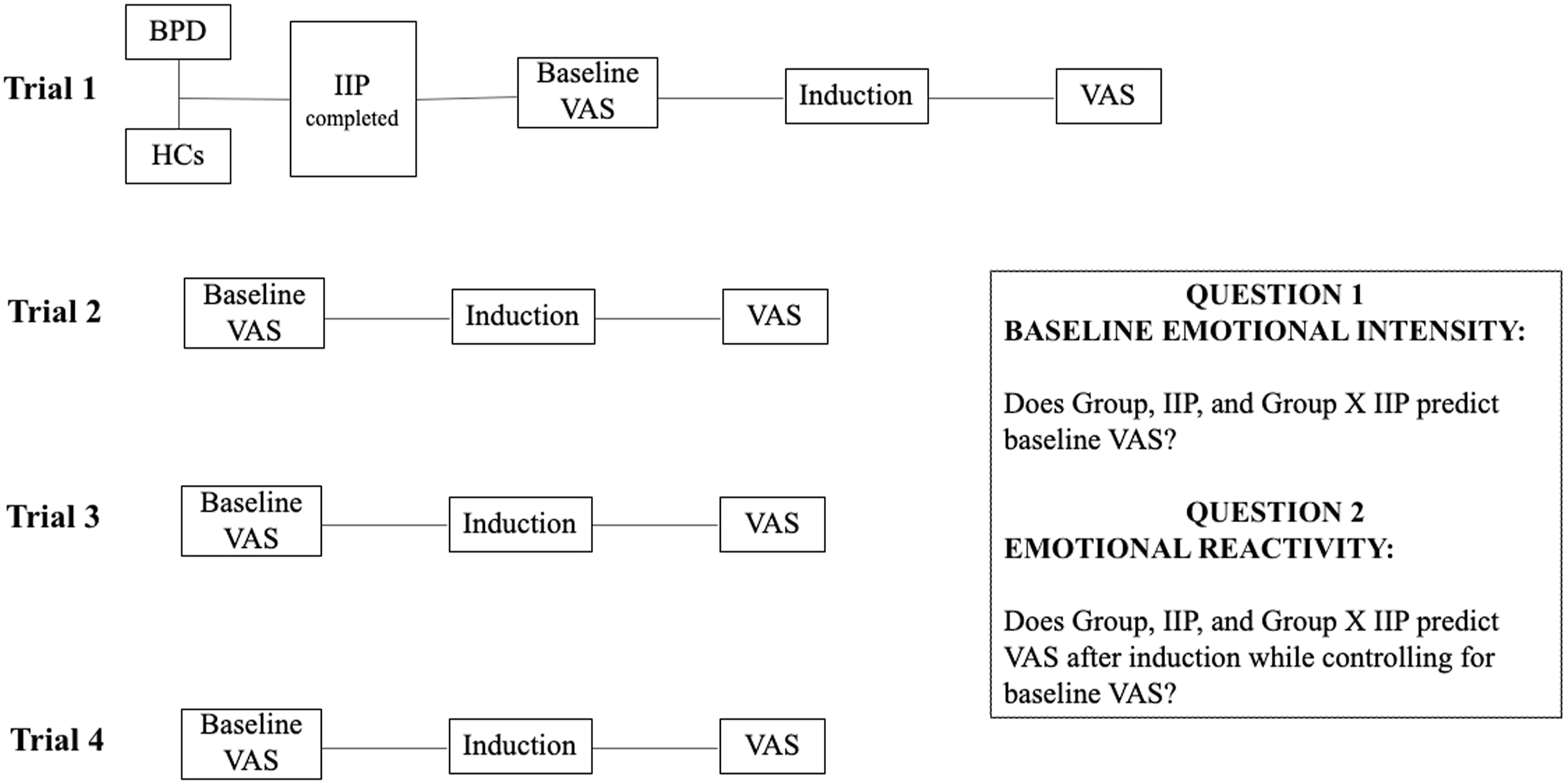
Method
The current project is a secondary data analysis drawn from a parent study that examined self-reported and physiological emotion processes in individuals with BPD and HCs. Recruitment procedures and additional sample characteristics (e.g., demographic and diagnostic comorbidities) from the parent study are presented elsewhere (Fitzpatrick et al., 2019) procedures germane to current analyses are delineated below.
Participants
Participants were 30 female (86.7%) and male (13.3%) adults, between 18 and 60 years old who met diagnostic criteria for BPD and 30 age- (i.e., within 5 years) and sex-matched HCs (i.e., 86.7% females and 13.3% males). All prospective participants were excluded if they reported current psychological disorders that obstructed participation (i.e., severe psychotic-spectrum disorders, Bipolar I Disorder, current alcohol or substance dependence). Given that the parent study involved psychophysiological measurement, participants were also excluded if they reported taking scheduled psychiatric medications other than selective serotonin reuptake inhibitors or other medications that influence physiology (e.g., beta-blockers), or if they reported having medical conditions (e.g., epilepsy), that may interfere with participation. All participants provided verbal and written informed consent.
The Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders-IV-TR (SCID-IV-TR; First et al., 1996) was administered to examine presence of what were formerly regarded as “Axis I” disorders. Borderline Personality Disorder diagnoses were assessed by the International Personality Disorder Examination—BPD Module (IPDE-BPD; Loranger et al., 1994). There were six Bachelors- or MA-level assessors in total administering assessments under the supervision of a licensed clinical psychologist. Inter-rater reliability between assessors and a gold-standard assessor ranged from a Prevalence and Bias Adjusted Kappa (Byrt et al., 1993) of 0.67 (indicating substantial agreement) to 1.00, with the average being 0.97 (indicating almost perfect agreement; Landis & Koch, 1977). HC participants were excluded if they (1) endorsed presence of any current psychiatric diagnoses; (2) met the self-injurious behavior BPD criterion; or (3) met four or more BPD criteria.
Procedures
Individuals who expressed interest in the study were briefly screened via phone or online assessment administered or reviewed by trained research assistants, respectively. Individuals who appeared eligible following this brief assessment were invited to come into the laboratory to undergo informed consent procedures and eligibility psychodiagnostic screening assessments (i.e., the SCID-IV-TR and the IPDE-BPD Module). Individuals who were deemed eligible were then invited to complete a series of self-report questionnaires and participate in a within-subjects experiment.
The experiment consisted of four trials in which participants underwent baseline, emotion induction, and emotion regulation blocks (see Figure 1, for overview of experimental paradigm). First, participants underwent five-minute baselines wherein they sat quietly in front of a computer without the presentation of stimuli. Then, participants were administered the emotion induction. In the emotion induction block, participants listened to one of four emotionally evocative scripts and were instructed to imagine that they were the protagonist as vividly as possible. These scripts focused on the death of one’s mother, a betrayal of one’s romantic partner with one’s best friend, a hit-and-run car accident, and the death of a dog and were previously piloted and shown to evoke negative emotions (See Fitzpatrick et al., 2019, for more information). Out of the four trials, two emotion induction blocks required participants to label their current emotions by typing them into the computer while example emotions appeared on the screen (e.g., sad, happy, neutral, ashamed, guilty; see Fitzpatrick et al., 2019 for more details regarding this condition). In the remaining two trials, participants were asked to describe objects that they imagined when listening to the emotion inducing scripts. The order of script presentation and its pairing with labeling versus object conditions was counterbalanced across participants. The parent study investigated the differential influence of these blocks on emotional reactivity and regulation processes, and readers are directed there for a review of those analyses (Fitzpatrick et al., 2019). An emotion regulation block followed the induction and required participants to use two strategies (i.e., mindfulness or reappraisal) to regulate their emotions. The emotion regulation block is not a focus of the present study and was not included in present analyses. They repeated these trials four times, with distinct combinations of emotion induction scripts, labelling/object prompts during the induction, and emotion regulation strategies during the emotion regulation block. Participants completed visual analogue scales (VAS) to report their experience of specific emotions (see below for more information) after the baseline, emotion induction, and emotion regulation blocks within each trial (12 VAS administrations total, 9 of which are relevant to the present study). Generalized estimating equations showed that the order of the baselines (i.e., the first, second, third, or fourth baseline) did not predict the level of emotional intensity ratings from each baseline (ps ranged from .185 to .948) and this effect (or lack thereof) was not moderated by group (ps ranged from .109 to .821).
Measures
The inventory of interpersonal problems-32 (IIP-32; Horowitz et al., 2000)
The IIP-32 is a 32-item self-report questionnaire that examines types and severity of interpersonal problems. Individuals are asked to rate how distressing each item has been on a scale from 0 (not at all) to 4 (extremely). The IIP-32 is also comprised of eight subscales (i.e., domineering/controlling, vindictive/self-centered, cold/distant, socially inhibited, nonassertive, overly accommodating, self-sacrificing, and intrusive/needy). The total score of the IIP-32, which consists of the sum of all eight subscale scores, was used for analysis in this study. The IIP-32 has demonstrated high interscale correlations (Bailey et al., 2018), and adequate validity and test-retest reliability (r = .78; Horowitz et al., 2000). The internal consistency for the present sample was high (α = .94).
Visual analogue scales
Participants self-reported their experience of specific emotions (i.e., sadness, fear, shame, anger, disgust, and guilt) before and after the induction (see below) from 0 (not at all) to 100 (very). Visual analogue scales are a common and reliable index of mental states (McCormack et al., 1988). Baseline emotion was measured by examining the VAS ratings following the four baseline blocks. Emotion induction was measured by examining the VAS ratings following the four emotion induction blocks, after controlling for the VAS ratings of the emotion that occurred following the baseline blocks.
Data analytic strategy
Study questions were tested using generalized estimating equations (GEE; Burton et al., 1998; Hubbard et al., 2010), which is a semi-parametric longitudinal data analytic method that optimizes statistical power by including participants with missing data. Baseline emotional intensity and emotional reactivity analyses were run separately, and statistical models were also run separately for each specific emotion outcome (i.e., sadness, disgust, fear, shame, anger, and guilt). This yielded 12 total analyses. For baseline analyses, specific emotion ratings provided immediately after the baseline phases across the four trials were entered as the outcome. Group, interpersonal problems, and group x interpersonal problem interactions were entered as predictors. For the emotional reactivity analyses, specific emotion ratings provided immediately after the induction phases were entered as the outcome. Baseline emotional intensity provided immediately before the induction phase (i.e., after the baseline phase) were entered as covariates. Group, interpersonal problems, and group × interpersonal problems interactions were entered as predictors. Continuous predictors were grand-mean centered. Inspection of the distributional form of study variables suggested that the baseline specific emotion variables were positively skewed (skew statistics ranged from 1.91 to 3.02 across specific emotions). Therefore, one unit was added to these variables which were then log transformed (base 10) prior to entering them into analyses as outcomes. The specific emotion variables following the induction exhibited less skew (skew statistics ranged from −.08 to 1.24 across specific emotions) and were therefore not transformed prior to being entered into analyses. For each analysis, exchangeable, autoregressive, and unstructured covariance structures were considered, and the model with the lowest quasiliklihood information criterion (QIC) was retained. Familywise error corrections were not employed given concerns that they may distort results (e.g., Armstrong, 2014).
Results
Means (standard deviations) of specific emotions across blocks, groups, and orders of presentations.

Note. HCs, healthy controls; BPD, borderline personality disorder.
Baseline Emotional Intensity
Generalized estimating equations analyses examining the moderating effects of interpersonal problems on baseline emotions across groups.

Note. Baseline emotion outcome variables are log transformed (base 10) with one unit added to them. Significant effects relevant to primary study outcomes are bolded.
Emotional reactivity
Generalized estimating equations analyses examining the moderating effects of interpersonal problems on emotional reactivity across groups.

Note. Significant effects relevant to primary study outcomes are bolded.
Discussion
The present study examined whether 1) interpersonal problems moderate the relationship between group (i.e., BPD vs. HC) and baseline emotional intensity across distinct emotions (i.e., shame, guilt, anger, disgust, fear, and sadness) and 2) whether interpersonal problems moderate the relationship between group and emotional reactivity across these distinct emotions.
Baseline emotional intensity
With respect to baseline emotional intensity, higher interpersonal problems were associated with higher sadness, disgust, fear, shame, and guilt, but not anger, for individuals with BPD only. In contrast to our hypothesis, these findings suggest that the association between interpersonal problems and baseline emotional intensity in BPD are not specific to social emotions such as shame and guilt (Hareli & Parkinson, 2008). Perhaps interpersonal problems impact overall emotional health, leading to a global increase in negative emotional intensity in BPD. Indeed, social support is robustly associated with emotional wellbeing (e.g., Gallagher & Vella-Brodrick, 2008; Lakey & Orehek, 2011). Accordingly, interpersonal problems may lead to deteriorated relationships and social support, in turn leading to chronically elevated distress. This may be especially true for individuals with BPD, who are more vulnerable to experiencing distress in response to interpersonal problems (Gratz et al., 2013). For example, individuals with BPD exhibit elevated rejection sensitivity (Berenson et al., 2016). Rejection sensitivity has been defined as a cognitive-affective processing disposition involving a tendency to anticipate, attend to, and react strongly towards rejection stimuli (Downey & Feldman, 1996). Given that BPD is associated with elevated rejection sensitivity in general, and especially in response to interpersonal stressors, (e.g., Berenson et al., 2016), individuals with BPD may be more prone to elevated emotional distress in response to interpersonal problems that may elicit rejection sensitivity.
Alternatively, chronically elevated emotion may also impact other relational processes in BPD, particularly communication, reciprocally causing more interpersonal problems (Fruzzetti & Fantozzi, 2008; Gottman, 1993). Indeed, Fruzzetti and Fantozzi (2008) theorize that difficulties with expressing emotion in BPD may perpetuate conflict in relationships because significant others respond to inaccurately expressed emotions (e.g., anger) rather than their partner’s initial, unexpressed emotions (e.g., shame). Hence, while interpersonal problems may lead to chronically intense emotions in BPD, they may also be reciprocally caused by chronically intense emotions (both social and non-social) through difficulties modulating or expressing them.
Unlike other baseline emotions in BPD, interpersonal problems were not associated with baseline anger intensity across groups. Perhaps the effects of interpersonal problems on anger intensity varies according to whether anger is directed towards the self or others. Specifically, several items on the IIP-32 may predict higher self-directed anger, but lower other-directed anger (e.g., difficulties asserting oneself), while other items may predict the inverse. The lack of precision with respect to measuring the directionality of anger and the specific types of interpersonal problems that may impact it may obfuscate potential relationships between these variables.
Emotional reactivity
With respect to emotional reactivity, individuals with BPD and HCs with higher interpersonal problems demonstrated greater sadness, fear, guilt, and anger, but not disgust, reactivity. Individuals with interpersonal problems may specifically exhibit heightened reactivity across these emotions following interpersonally themed stressors, like the ones used in the present study. Exposure to such stimuli may elicit memories and emotions associated with pre-existing interpersonal problems, thereby exacerbating emotion reactivity across multiple emotions. Additionally, elevated interpersonal problems (e.g., loneliness; Holt-Lunstad et al., 2015) suggest limited access to social support. Indeed, increased social support offers resilience to stress (Ozbay et al., 2007), and buffers against elevations in negative emotion following stressful events (e.g., Atienza et al., 2001; Mackin et al., 2016). Thus, reduced social support may result from higher interpersonal problems and account for elevated reactivity across the observed emotions. Finally, the influence of interpersonal problems on emotional reactivity across emotions (except for disgust) may also be accounted for by a third variable (e.g., reduced capacity to regulate one’s own emotions, distress tolerance, disturbances in identity, and substance use), which may elicit both interpersonal problems and heightened emotional reactivity.
However, unlike other emotions, disgust reactivity was not moderated by interpersonal problems in BPD or HC groups. Disgust may be particularly likely to be elicited in response to threats of contamination or related stimuli (e.g., germs; physiological injury; Davey, 2011), rather than to events that occur in the presence of, or in response to, others. Disgust may therefore be less influenced by interpersonal problems than the other examined emotions. Also, as a discrete emotion state specifically linked to disgusting stimuli, it may not have been evoked by the interpersonally themed stressors in the present study. Low disgust reactivity in general would have prevented the examination of its relationship to interpersonal problems.
Shame reactivity specific to those with borderline personality disorder
Importantly, this study also demonstrated that, for individuals with BPD and not HCs, higher interpersonal problems were associated with higher shame reactivity specifically. Compared to other emotions, shame is particularly interpersonally linked given that it requires feedback from others (e.g., thoughts, feelings, and behaviors; Hareli & Parkinson, 2008). Linehan’s Biosocial Model (1993) posits that BPD develops in the context of an invalidating interpersonal rearing environment, emphasizing that a child’s emotional experiences are not treated as valid responses to events. Relatedly, BPD is also associated with heightened childhood emotional abuse (e.g., Bornovalova et al., 2005; Gratz et al., 2008). This invalidating interpersonal and developmental context may lead individuals with BPD to perceive themselves to be “bad,” or “shameful,” in response to interpersonal problems (e.g., conflict, invalidation). Such a pattern may become particularly ingrained for those with BPD who are higher in interpersonal problems—and thus have more exposure to the association between interpersonal stressors and shame—over time.
In addition to this developmental context, shame also elicits several behaviors in response to distress that may lead to interpersonal problems in BPD specifically. For instance, in response to shame, individuals can be motivated to withdraw, hide, or isolate themselves from others (e.g., Haidt, 2003; Keltner & Harker, 1998). The experience of shame can therefore obstruct healthy communication, vulnerability, and connection with others, perhaps further exacerbating interpersonal problems in BPD. Therefore, while higher interpersonal problems may predict elevated shame reactivity, such increases in shame following distress may reciprocally worsen interpersonal problems. This may be particularly true for those with BPD given that they are particularly likely to engage in emotion-driven behaviors (e.g., Sauer-Zavala et al., 2020).
Finally, contrary to our hypothesis, interpersonal problems did not differentially moderate emotional reactivity of guilt in BPD versus HCs. Although both shame and guilt can be considered social emotions; they may have differential associations with interpersonal problems in BPD. Some studies indicate that BPD features are associated with higher levels of shame, but lower levels of guilt (Peters & Geiger, 2016; Schoenleber & Berenbaum, 2012). Shame may also be more likely to be elicited following distress associated with self-oriented thoughts, while guilt may instead emerge in response to other-oriented interactions (e.g., conflict). Thus, the invalidating environment (Linehan, 1993) may be more likely to make individuals with BPD focus their attention on themselves in response to interpersonal distress, instead of on their overt behaviors, leading to elevated shame reactivity, but not guilt. Interpersonal problems, which also characterize the invalidating environment, may further fuel this pattern. Conversely, guilt may only occur in response to specific contexts wherein an individual has done something “wrong,” which may not have been captured by the laboratory stressors utilized in the present work. Additionally, in BPD, chronic interpersonal problems may exacerbate shame in response to stressors, while acute interpersonal problems (e.g., arguments)—which were not measured in this study—may activate guilt and subsequently motivate individuals to repair relational ruptures (e.g., Estrada-Hollenbeck & Heatherton, 1998). In summary, interpersonal problems in BPD appear be uniquely associated with shame, which may be activated following negative self-thoughts, but not guilt, which interpersonal problems may be related to in the specific context of interpersonal interactions.
Limitations and future directions
This study has several limitations to note. First, a self-report global measure of interpersonal problems was used, which fails to reveal whether distinct interpersonal problems (e.g., frequent conflict, difficulties with assertiveness) moderate specific emotions (e.g., anger) at baseline and emotional reactivity. Thus, future work should examine if distinct facets of interpersonal problems are associated with specific baseline emotions and emotional reactivity. Second, interpersonal problems may be associated with anger at baseline, as well as disgust reactivity, but these effects may be less detectable in the context it was measured (e.g., anger may be less intense in the absence of a direct interpersonal stressor). Future research may thus require ecological momentary assessment or daily diary study designs to optimally elucidate the relationship between interpersonal problems on specific emotions on baseline emotional intensity and emotional reactivity in BPD. Third, a self-report measure was used to assess baseline emotional intensity and emotional reactivity. Given that research suggests that the subjective emotion measures are particularly discrepant for those with BPD relative to physiological measures (e.g., Kuo et al., 2016), it is advised that future work examine the relationship between interpersonal problems and baseline emotional intensity and emotional reactivity using physiological indices (e.g., heart rate, skin conductance response). Fourth, while this study examined several common and distinct negative emotions, it did not examine the relationship between interpersonal problems on specific positive emotions at baseline or in response to distress. Given that positive emotions physiologically downregulate negative emotion (Tugate & Frederickson, 2004), examining whether interpersonal problems are related to positive emotions, and whether positive emotions mediate the relationship between interpersonal problems and negative emotions at baseline and in response to distress, reflects a fruitful path of future inquiry. Fifth, given that trait difficulties in regulating emotions may both elicit interpersonal problems and the ED components measured in this study, future researchers are encouraged to investigate whether interpersonal problems mediate the relationship between trait difficulties regulating one’s emotions and emotional reactivity. In addition to the above limitations, this study contained a small sample size, which can reduce statistical power, thus limiting the generalizability of the findings (Polit & Beck, 2010). Therefore, these results warrant replication with larger samples.
Clinical implications and conclusions
Despite these limitations, this study is the first to examine whether interpersonal problems moderate the relationship between BPD and baseline emotional intensity and emotional reactivity across specific emotions. These findings suggest that targeting interpersonal problems in BPD interventions may reduce baseline intensity of negative emotions broadly (except anger). This work also suggests that for BPD and HCs, reducing interpersonal problems may also improve sadness, fear, guilt, and anger, but not disgust, following a stressor.
In sum, clinicians are advised that, when working with clients with BPD, elevated interpersonal problems may signal higher sadness, disgust, fear, shame, and guilt at baseline, as well as sadness, fear, guilt, anger, and shame reactivity, the last of which may be unique to BPD. Targeting interpersonal problems in BPD when elevated may reduce such elevated emotions. This study also highlights the need for clinicians to be proficient in assessing shame reactivity and shame-related problems in those with BPD who have interpersonal problems. Importantly, individuals with BPD who have interpersonal problems may be particularly reactive with shame. Targeting interpersonal problems may be essential in BPD specifically to reduce elevations in shame following a stressor.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The following grants supported this work: The Canadian Institutes of Health Research (CIHR) Frederick Banting and Charles Best Canada Graduate Scholarship Doctoral Award [grant number 201210GSD-304038-229817], The Harry Rosen Stress Institute Award, Toronto, ON; and the Ontario Mental Health Foundation Studentship Award, Toronto, ON.
Ethical approval
This work was given ethics approval by a local ethics review committee.
Informed consent
All participants underwent informed consent procedures.