
Abstract
Background:
Researchers have examined intolerance of uncertainty (IU) and negative beliefs about worry (NBW) in emotional disorders. However, the distinct relationships of IU and NBW remain unclear. We examined IU and NBW across emotional disorders, controlling for overlapping symptoms. We also explored prospective and inhibitory IU.
Methods:
A sample of 565 undergraduates completed measures of IU and NBW, as well as measures of generalized anxiety, depression, social anxiety, panic, post-traumatic stress, obsessive-compulsive, and illness anxiety disorder symptoms. Regression analyses were used to determine which factors were uniquely associated with symptoms of each disorder.
Results:
Both IU and NBW were associated with generalized anxiety and social anxiety disorder symptoms. IU was also associated with obsessive-compulsive disorder symptoms and negatively associated with panic disorder symptoms. NBW was also associated with depression. Neither IU now NBW were associated with post-traumatic stress or illness anxiety disorders. Prospective and inhibitory IU also had differential associations with the emotional disorders.
Conclusions:
Our results indicate that IU and NBW, while transdiagnostic, are differentially associated with emotional disorder symptoms. Our results also support the discriminant validity of prospective and inhibitory IU.
Keywords
Introduction
Intolerance of uncertainty (IU) and negative beliefs about worry (NBW) have been found to contribute to a variety of emotional disorders, including generalized anxiety (McEvoy & Mahoney, 2011; Penney et al., 2013), major depression (Saulnier et al., 2019; Spada et al., 2008), social anxiety (Carleton et al., 2010; McEvoy & Perini, 2009), panic (Carleton et al., 2014; Cucchi et al., 2012), post-traumatic stress (Boelen et al., 2016; Roussis & Wells, 2006), obsessive-compulsive (Cucchi et al., 2012; McEvoy & Mahoney, 2011), and illness anxiety disorders (Bailey & Wells, 2015; Wright et al., 2016). Both IU and NBW are considered transdiagnostic risk and maintenance factors for emotional disorder symptoms (Carleton, 2016; McEvoy & Mahoney, 2013; Ryum et al., 2017; Shihata et al., 2016). However, research has not yet clearly elucidated the potential differentiating relationships of IU and NBW with specific sets of emotional disorder symptoms.
IU and NBW across emotional disorders
IU
IU is understood as a cognitive, emotional, and behavioral reaction to uncertainty (Freeston et al., 1994). IU has been recently defined as “an individual’s dispositional incapacity to endure the aversive response triggered by the perceived absence of salient, key, or sufficient information, and sustained by the associated perception of uncertainty” (Carleton, 2016, p. 31). As discussed by Shihata et al. (2018; see also Bottesi et al., 2019; Hale et al., 2016), following the development of the 12-item version of the Intolerance of Uncertainty Scale (IUS-12; Carleton et al., 2007), researchers began exploring the proposed IU subfactors of prospective IU and inhibitory IU.
Prospective IU refers to approach-oriented responses resulting from IU, such as cognitive anticipation and evaluations of future uncertainties (Hong & Lee, 2015; Shihata et al., 2018). Associations between prospective IU and various emotional disorders are thought to result from worry about some uncertain future event, which activates maladaptive behaviors (Fetzner et al., 2014; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011). For example, in relation to illness anxiety disorder, an individual might be concerned about contracting a serious medical condition in the future and might engage in increased body checking and reassurance seeking behaviors due to prospective IU. Inhibitory IU refers to avoidance-oriented responses resulting from IU, including avoidance or behavioral inhibition (Hong & Lee, 2015; Shihata et al., 2018). Associations between inhibitory IU and emotional disorders are attributed to an individual’s tendency to engage in avoidance behaviors in the face of uncertainty (Fetzner et al., 2013; McEvoy & Mahoney, 2011). For example, an individual with social anxiety disorder might avoid social gatherings and meeting new people due to inhibitory IU.
There is accumulating evidence of discriminant validity for prospective and inhibitory IU. Prospective IU generally appears to be most associated with generalized anxiety disorder and obsessive-compulsive disorder (Hong & Lee, 2015; Jacoby et al., 2013; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011). Inhibitory IU generally appears to be most associated with depression, social anxiety disorder, and panic disorder (Boelen & Lenferink, 2018; Boelen et al., 2016; Carleton et al., 2010, 2013, 2014; Hong & Lee, 2015; Jensen et al., 2016; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011; Saulnier et al., 2019; Whiting et al., 2014). However, there have been equivocal results. For example, researchers have also found inhibitory IU to be associated with generalized anxiety disorder and obsessive-compulsive disorder (Jacoby et al., 2013; Mahoney & McEvoy, 2012b). Similarly, post-traumatic stress disorder and illness anxiety disorder have each been associated with both prospective IU and inhibitory IU (Boelen et al., 2016; Fetzner et al., 2013, 2014; Raines et al., 2019; Wright et al., 2016).
One proposed reason for the lack of consistent results has been the use of the IUS-12 prospective and inhibitory subscales. Several recent studies have found that a bifactor model of IU yields the best fit, wherein overall trait IU accounts for the majority of variance in IUS-12 scores (Bottesi et al., 2019; Coranacchio et al., 2018; Hale et al., 2016; Lauriola et al., 2016; Saulnier et al., 2019; Shihata et al., 2018; Yao et al., 2020). As discussed by Shihata et al. (2018), it has been suggested that only the IUS-12 total score should be used in IU-related research, rather than the prospective and inhibitory subscale scores. However, while the aforementioned articles raise valid concerns about the IUS-12 prospective and inhibitory subscales, it is important to note it is not necessarily the case that the constructs of prospective IU and inhibitory IU are invalid. Saulnier et al. (2019) have argued that there is enough evidence of discriminatory validity between prospective IU and inhibitory IU to continue to examine the IUS-12 prospective and inhibitory subscales. The argument to continue to examine prospective IU and inhibitory IU as separate constructs aligns with the conclusions of Yao et al. (2020); that if the purpose of a study is to examine how prospective and inhibitory IU differentially relate to psychopathology, then the use of the IUS-12 prospective and inhibitory subscales is acceptable.
Beyond the psychometric properties of the IUS-12, other factors might also have contributed to the inconsistent results obtained when examining prospective and inhibitory IU. We propose that the following factors might have also led to inconsistent results: the use of small sample sizes, examining only one or two symptom types within a single study, and not including other variables related to prospective and inhibitory IU that might also play a role in the development and maintenance of multiple emotional disorders. Therefore, in the current study, we used a large sample, measured the symptoms of multiple emotional disorders, and included another transdiagnostic factor: NBW.
NBW
NBW are conceptualized as beginning with an individual’s metacognitive appraisal of their worry, whereby the person engages in worry about their worry, also known as meta-worry (Bailey & Wells, 2015; Cucchi et al., 2012; Wells, 2009; Wells & Carter, 1999, 2001). Specifically, the individual believes they are unable to control their worries and that their worries might cause damage to their body and/or mind (Wells, 2009). This negative appraisal of worry might result in an attentional bias toward threat-related information (Fergus et al., 2013; Wells & Carter, 1999, 2001), which perpetuates the worry process and results in maladaptive behaviors, such as avoidance or reassurance seeking.
NBW have been primarily associated with generalized anxiety disorder (Hirsch et al., 2013; Penney et al., 2013; Ruscio & Borkovec, 2004; Wells & Carter, 1999, 2001) and are usually conceptualized as a specific vulnerability for generalized anxiety disorder. However, while NBW have been demonstrated to play a larger role in generalized anxiety disorder than other emotional disorders (Spada et al., 2008; Wells & Carter, 2001), research has also shown NBW to be associated with depression (Nordahl et al., 2019; Spada et al., 2008; Wells & Carter, 2001), social anxiety disorder (McEvoy et al., 2009; McEvoy & Perini, 2009), panic disorder (Cucchi et al., 2012; Wells & Carter, 2001), post-traumatic stress disorder (Roussis & Wells, 2006), obsessive-compulsive disorder (Cucchi et al., 2012; Wells & Cartwright-Hatton, 2004; Wells & Papageorgiou, 1998), and illness anxiety disorder (Bailey & Wells, 2015; Kaur et al., 2011). Longitudinal research has also indicated that NBW play a role in the development of anxiety and paranoia over time (Ryum et al., 2017; Sun et al., 2019). NBW have also been associated with a predisposition to visual hallucinations (Morrison et al., 2002). Further, of the subscales on the Metacognitions Questionnaire-30 (MCQ-30; Wells & Cartwright-Hatton, 2004), which is considered the gold standard measure of metacognitive beliefs (Thielsch et al., 2015), the NBW subscale has been found to be the main contributor to both anxiety and depression (Nordahl et al., 2019; Spada et al., 2008). Therefore, NBW can be considered to be a transdiagnostic factor across emotional disorders, similar to IU (Hirsch et al., 2013; Koerner et al., 2015; McEvoy & Mahoney, 2013).
Unfortunately, like the prospective and inhibitory IU literature, the research examining NBW is not without limitations. As mentioned, most studies have focused on the links between NBW and generalized anxiety disorder, without examining a range of symptoms. As well, many studies have relied upon small samples. Further, while research has examined IU and NBW together in emotional disorders, no studies have examined NBW alongside prospective and inhibitory IU specifically.
The present study
Previous research examining IU and NBW has consistently demonstrated a strong positive correlation between the constructs (Britton et al., 2019; Khawaja & McMahon, 2011; Koerner et al., 2015; Ruggiero et al., 2012; van der Heiden et al., 2010; Voon & Phillips, 2015). Researchers have found that IU and NBW together mediate the relationship between neuroticism and repetitive negative thinking (McEvoy & Mahoney, 2013) and that worrying leads to heightened IU and NBW (Britton et al., 2019). NBW have also been shown to both mediate and moderate the association between IU and worry (Ruggiero et al., 2012; Voon & Phillips, 2015), though Thielsch et al. (2015) found that NBW predicted daily worry, while IU did not. Regarding specific disorders, Khawaja and McMahon (2011) found that both IU and NBW were associated with generalized anxiety disorder, social anxiety disorder, and obsessive-compulsive disorder. Likewise, Koerner et al. (2015) found that both IU and NBW were related to generalized anxiety disorder severity, while van der Heiden et al. (2010) found that both IU and NBW mediate the relationship between neuroticism and generalized anxiety disorder, as well as between neuroticism and depression.
To date, IU and NBW have not been examined together across a range of emotional disorders within a single study. Researchers have argued for a broader examination of emotional disorder symptoms within individual studies, as identifying factors that are predictive of symptoms across disorders is hindered when only a limited scope of emotional disorders are examined in a study (McEvoy & Mahoney, 2011). Further, no research has examined the associations between NBW and emotional disorders while also including prospective IU and inhibitory IU. Research examining both NBW and prospective and inhibitory IU is needed, as considering prospective IU and inhibitory IU alongside NBW could enhance our understanding of how the three factors relate to one another and to emotional disorder symptoms.
The current study was designed to explore the independent contributions of IU and NBW in emotional disorder symptoms in a university student sample. Specifically, IU and NBW were examined in relation to generalized anxiety, depression, social anxiety, panic, post-traumatic stress, obsessive-compulsive, and illness anxiety disorder symptoms. To clearly articulate which factors of IU and NBW were uniquely associated with each set of symptoms, we controlled for overlapping symptoms across the emotional disorders. Previous research supporting the dimensional nature of IU (Carleton et al., 2012) and NBW (Ruscio & Borkovec, 2004) provides justification for examining IU and NBW with a nonclinical sample. Moreover, researchers have suggested that using clinical samples might attenuate associations between variables, while range restrictions are not as significant of a concern with nonclinical data (McEvoy et al., 2019). We also repeated our analyses using the prospective and inhibitory IUS-12 subscale scores.
Method
Participants
The present study received ethics approval from the university’s research ethics board. A nonclinical sample of 565 undergraduate university students was recruited. The sample was primarily Caucasian (58%) and female (77%), with a mean age of 21.46 years (SD = 5.66). No inclusion or exclusion criteria were utilized. Demographic characteristics of the sample are reported in Table 1.
Demographic characteristics of the sample.

Note. Percentages do not always add up to 100% due to missing data.
Measures
12-item Intolerance of Uncertainty Scale (IUS-12)
The IUS-12 is a 12-item self-report questionnaire that requires individuals to indicate the extent to which statements pertaining to IU are characteristic of them (Carleton et al., 2007). The IUS-12 can be scored as a total score, and the 7-item prospective IU (IUS-PRO) and 5-item inhibitory IU (IUS-INH) subscales can be scored separately. Prospective IU is represented in items such as “I always want to know what the future has in store for me,” whereas inhibitory IU is represented in items such as “when it’s time to act, uncertainty paralyzes me.” Scores on the IUS-PRO range from 7 to 35, scores on the IUS-INH range from 5 to 25, and scores on the full scale range from 12 to 60. The IUS-12 possesses strong psychometric properties and is valid for use in nonclinical samples (Carleton et al., 2007).
Metacognitions Questionnaire-30 (MCQ-30)
The MCQ-30 is a 30-item self-report measure of metacognition comprised of five subscales: (a) NBW, (b) cognitive confidence, (c) cognitive self-consciousness, (d) positive beliefs about worry, and (e) beliefs about the need to control thoughts (Wells & Cartwright-Hatton, 2004). Each subscale includes six questions where individuals are asked to indicate the extent to which they either agree or disagree with statements that reflect their beliefs. Scores on each subscale range from 6 to 24. For the purposes of the present study, only the NBW subscale (MCQ-NBW) was used in the analyses. NBW are represented in items such as “I cannot ignore my worrying thoughts.” The MCQ-30 demonstrates excellent psychometric properties and is valid for use in nonclinical samples (Wells & Cartwright-Hatton, 2004).
Generalized Anxiety Disorder Questionnaire-IV (GADQ-IV)
The GADQ-IV is a 9-item self-report measure of symptoms of generalized anxiety disorder (Newman et al., 2002). The GADQ-IV consists of five yes/no items, one checklist item, one fill-in-the-blank item, and two Likert-type scale items. Total scores for the GADQ-IV range from 0 to 12. The GADQ-IV displays strong psychometric properties and is valid for use in nonclinical samples (Newman et al., 2002).
Inventory of Depression and Anxiety Symptoms (IDAS)
The IDAS is a 64-item self-report questionnaire consisting of 12 subscales: (a) General Depression (IDAS-DEP), (b) Social Anxiety (IDAS-SA), (c) Panic (IDAS-PD), (d) Traumatic Intrusions (IDAS-PTSD), (e) Suicidality, (f) Lassitude, (g) Insomnia, (h) Appetite Loss, (i) Appetite Gain, (j) Ill Temper, (k) Dysphoria, and (l) Well-Being (Watson et al., 2007). For the purposes of the present study, only the IDAS-DEP, IDAS-SA, IDAS-PD, and IDAS-PTSD subscales were used in the analyses. The IDAS-DEP subscale includes 21 items, with scores ranging from 21 to 105. The IDAS-SA subscale includes 5 items, with scores ranging from 5 to 25. The IDAS-PD subscale includes 8 items, with scores ranging from 8 to 40. Lastly, the IDAS-PTSD subscale includes 4 items, with scores ranging from 4 to 20. The IDAS demonstrates excellent psychometric properties and is valid for use in nonclinical samples (Watson et al., 2007).
Obsessive-Compulsive Inventory—short version (OCI-R)
The OCI-R is an 18-item self-report questionnaire designed to assess symptoms of obsessive-compulsive disorder (Foa et al., 2002). Total scores on the OCI-R range from 0 to 72. The OCI-R displays strong psychometric properties and is valid for use in nonclinical samples (Foa et al., 2002).
Short Health Anxiety Inventory (SHAI)
The SHAI is an 18-item self-report measure of health anxiety (Salkovskis et al., 2002). Total scores on the SHAI range from 0 to 54. The SHAI possesses strong psychometric properties and is valid for use in nonclinical samples (Abramowitz et al., 2007).
Procedure
All measures were formatted into an online survey using Qualtrics, an online survey platform, and were made available to undergraduate psychology students. Potential participants self-selected to complete the study through an online research portal. All participants read an online consent form, after which they were directed to complete a demographics questionnaire, followed by the IUS-12, MCQ-30, GADQ-IV, IDAS, OCI-R, and SHAI, in a randomized order. Consent was implied by participants continuing on to complete the survey after having the opportunity to read the consent form. Participants were directed to an online debriefing form after completing the questionnaires. All participants received a 2% psychology course credit for their participation.
Statistical analyses
Descriptive statistics of scales and subscales, as well as Cronbach’s α coefficients for each scale and subscale, were calculated. Pearson product-moment (r) correlations were then calculated between all scales and subscales. Hierarchical regression analyses were then conducted to identify the specific contributions of IU and NBW. Two hierarchical linear regressions were modeled for symptoms of each emotional disorder, with either IU total scores or prospective IU and inhibitory IU subscale scores entered in Step 1 and NBW scores in Step 2. In Step 3, scores for the other emotional disorders were entered. Given the number of analyses conducted, a more stringent α level of .025 was used for all analyses. The α adjustment to .025 reduces the probability of making Type 1 errors related to multiple testing without unnecessarily inflating the probability of Type 2 errors (Frane, 2015). Using a desired power level of .80 and an α level of .025, post hoc power analysis determined that the smallest effect size able to be detected for the most complex model, using a sample size of 565, is f 2 = .028.
Results
Means, standard deviations, and Cronbach’s α coefficients for all scales and subscales are reported in Table 2. All Cronbach’s α coefficients were within the acceptable range (.70 ≤ α ≤ .95; Tavakol & Dennick, 2011). Pearson-product moment (r) correlations revealed that all scales and subscales were correlated at the zero-order level (ps < .001) and are reported in Table S1 of the Supplementary Materials. The correlations indicate significant overlap across emotional disorder symptoms. IU total, prospective IU, inhibitory IU, and NBW scores significantly correlated with symptoms of each emotional disorder, as well as with each other.
Means, standard deviations, and internal consistencies.

Note. IUS = intolerance of uncertainty total score; IUS-PRO = prohibitory intolerance of uncertainty; IUS-INH = inhibitory intolerance of uncertainty; MCQ-NBW = negative beliefs about uncontrollability and danger of worry; GADQ-IV = generalized anxiety symptoms Questionnaire-IV; IDAS-DEP = depression symptoms; IDAS-SA = social anxiety symptoms; IDAS-PD = panic symptoms; IDAS-PTSD = traumatic intrusions; OCI-R = obsessive-compulsive symptoms; SHAI = health anxiety.
Seven hierarchical linear regression analyses were conducted with scores for specific emotional disorder symptoms entered into the model as the dependent variable, with IU total scores entered in Step 1, NBW scores in Step 2, and the symptom scores for all remaining emotional disorder symptoms in Step 3 (see Table 3). Each hierarchical linear regression analysis was repeated using prospective IU scores and inhibitory IU scores in Step 1 instead of IU total scores (see Table 4). For example, when symptoms of generalized anxiety (GADQ-IV) were entered as the dependent variable, IU total scores were entered in Step 1, NBW scores were entered in Step 2, and scores for depression (IDAS-DEP), social anxiety (IDAS-SA), panic (IDAS-PD), post-traumatic stress (IDAS-PTSD), obsessive-compulsive (OCI-R), and illness anxiety (SHAI) disorder symptoms were entered in Step 3. This analysis was then repeated, with IU total scores being substituted for prospective IU and inhibitory IU scores on Step 1.
Summary of regression analyses using total IU and NBW scores.
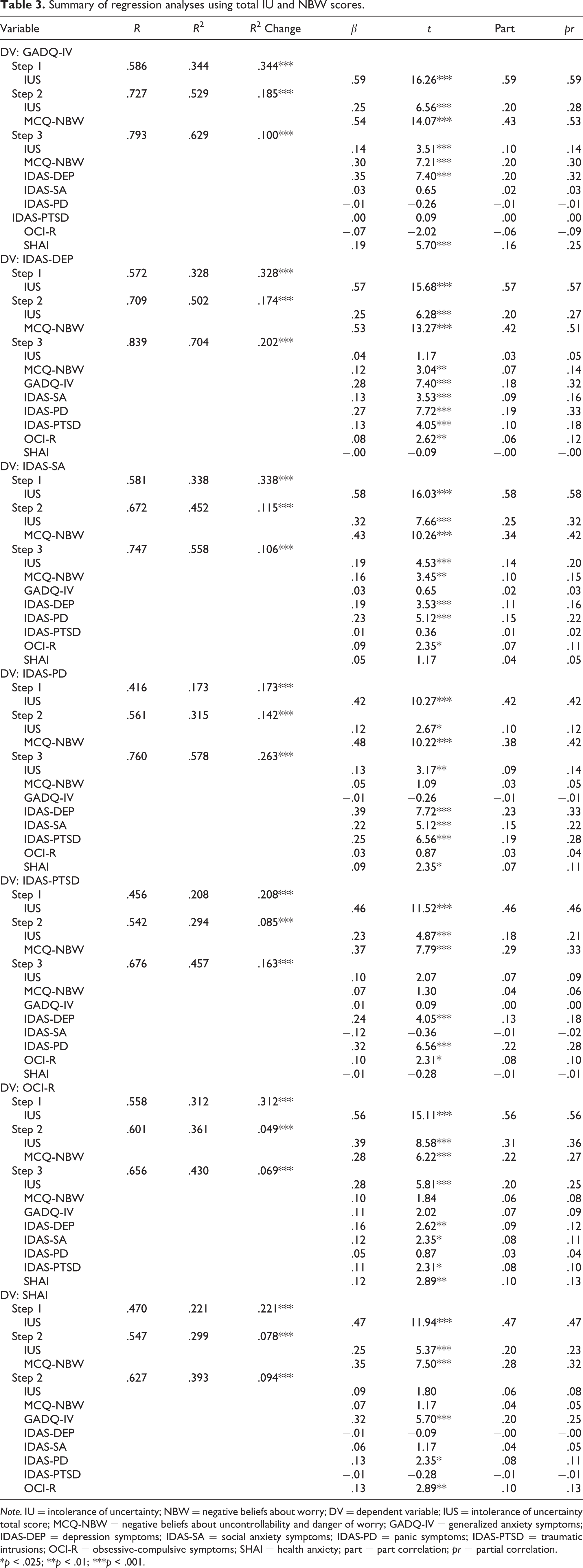
Note. IU = intolerance of uncertainty; NBW = negative beliefs about worry; DV = dependent variable; IUS = intolerance of uncertainty total score; MCQ-NBW = negative beliefs about uncontrollability and danger of worry; GADQ-IV = generalized anxiety symptoms; IDAS-DEP = depression symptoms; IDAS-SA = social anxiety symptoms; IDAS-PD = panic symptoms; IDAS-PTSD = traumatic intrusions; OCI-R = obsessive-compulsive symptoms; SHAI = health anxiety; part = part correlation; pr = partial correlation.
*p < .025; **p < .01; ***p < .001.
Summary of regression analyses using prospective IU, inhibitory IU, and NBW scores.
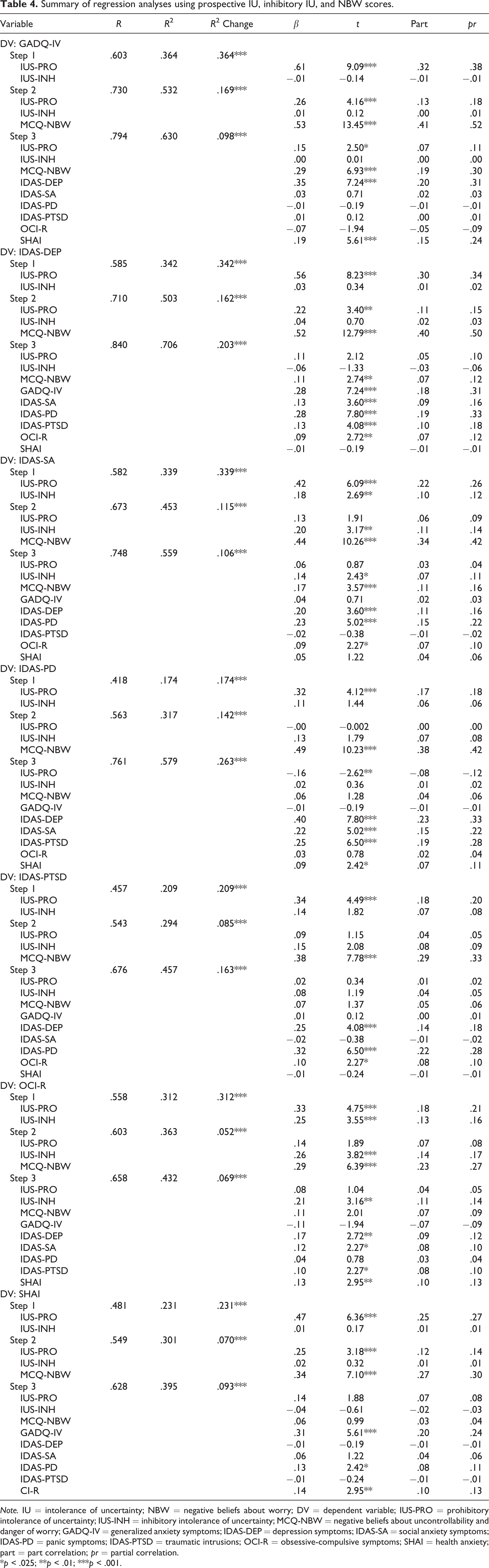
Note. IU = intolerance of uncertainty; NBW = negative beliefs about worry; DV = dependent variable; IUS-PRO = prohibitory intolerance of uncertainty; IUS-INH = inhibitory intolerance of uncertainty; MCQ-NBW = negative beliefs about uncontrollability and danger of worry; GADQ-IV = generalized anxiety symptoms; IDAS-DEP = depression symptoms; IDAS-SA = social anxiety symptoms; IDAS-PD = panic symptoms; IDAS-PTSD = traumatic intrusions; OCI-R = obsessive-compulsive symptoms; SHAI = health anxiety; part = part correlation; pr = partial correlation.
*p < .025; **p < .01; ***p < .001.
With GADQ-IV scores as the dependent variable, both IU total and NBW scores accounted for a significant amount of variance in generalized anxiety symptoms (see Table 3). Step 1 accounted for 34.4% of the variance in GADQ-IV scores, F(1, 504) = 264.24, p < .001, and Step 2 accounted for an additional 18.5% of variance, ΔF(2, 503) = 197.82, p < .001. In addition to IU total and NBW scores, IDAS-DEP and SHAI scores significantly accounted for variance in GADQ-IV scores in Step 3. Step 3 accounted for an additional 10.0% of the total variance in GADQ-IV scores, ΔF(6, 497) = 22.42, p < .001. When examining prospective IU, inhibitory IU, and NBW scores, prospective IU scores and NBW scores significantly accounted for variance in GADQ-IV scores in addition to IDAS-DEP and SHAI scores (see Table 4). Step 1 accounted for 36.4% of the variance in GADQ-IV scores, F(2, 503) = 143.75, p < .001, while Step 2 accounted for an additional 16.9% of the variance, ΔF(1, 502) = 180.91, p < .001. Step 3 accounted for an additional 9.8% of the total variance in GADQ-IV scores, ΔF(6, 496) = 21.95, p < .001.
With IDAS-DEP scores as the dependent variable, both IU total and NBW scores accounted for a significant amount of variance in depression symptoms in Step 2 (see Table 3). Step 1 accounted for 32.8% of the variance in IDAS-DEP scores, F(1, 504) = 245.73, p < .001, and Step 2 accounted for an additional 17.4% of variance, ΔF(1, 503) = 176.18, p < .001. In addition to NBW scores, GADQ-IV, IDAS-SA, IDAS-PD, IDAS-PTSD, and OCI-R scores significantly accounted for variance in IDAS-DEP scores in Step 3, while IU total scores became nonsignificant. Step 3 accounted for an additional 20.2% of the total variance in IDAS-DEP scores, ΔF(6, 497) = 56.61, p < .001. Similarly, when examining the contributions of prospective IU, inhibitory IU, and NBW scores, NBW scores significantly accounted for variance in IDAS-DEP scores in addition to the comorbid emotional disorder symptoms (see Table 4). Prospective IU scores were significant in Steps 1 and 2, but not in Step 3. Step 1 accounted for 34.2% of the variance in IDAS-DEP scores, F(2, 503) = 130.55, p < .001, while Step 2 accounted for an additional 16.2% of variance, ΔF(1, 502) = 163.46, p < .001. Step 3 accounted for an additional 9.8% of the total variance in IDAS-DEP scores, ΔF(6, 496) = 57.04, p < .001.
With IDAS-SA scores as the dependent variable, IU total and NBW scores accounted for a significant amount of variance in social anxiety symptoms (see Table 3). Step 1 accounted for 33.8% of the variance in IDAS-SA scores, F(1, 504) = 256.94, p < .001, and Step 2 accounted for an additional 11.5% of variance, ΔF(1, 503) = 105.17, p < .001. In addition to IU total and NBW scores, IDAS-DEP, IDAS-PD, and OCI-R scores significantly accounted for variance in IDAS-SA scores in Step 3. Step 3 accounted for an additional 10.6% of the total variance in IDAS-SA scores, ΔF(6, 497) = 19.91, p < .001. When examining prospective IU, inhibitory IU, and NBW scores, inhibitory IU scores and NBW scores significantly accounted for variance in IDAS-SA scores in addition to IDAS-DEP, IDAS-PD, and OCI-R scores (see Table 4). Step 1 accounted for 33.9% of the variance in IDAS-SA scores, F(2, 503) = 128.88, p < .001, while Step 2 accounted for an additional 11.5% of variance, ΔF(1, 502) = 105.18, p < .001. Step 3 accounted for an additional 10.6% of the total variance in IDAS-SA scores, ΔF(6, 496) = 19.89, p < .001.
With IDAS-PD scores as the dependent variable, IU total and NBW scores accounted for a significant amount of variance in panic symptoms in Step 2 (see Table 3). Step 1 accounted for 17.3% of the variance in IDAS-PD scores, F(1, 504) = 105.46, p < .001, and Step 2 accounted for an additional 14.2% of variance, ΔF(1, 503) = 104.43, p < .001. IDAS-DEP, IDAS-SA, IDAS-PTSD, and SHAI scores, as well as IU total scores, accounted for significant variance in IDAS-PD scores in Step 3. Step 3 accounted for an additional 26.3% of the total variance in IDAS-PD scores, ΔF(6, 497) = 51.49, p < .001. Notably, while NBW scores became nonsignificant, IU total scores exhibited a significant negative association with IDAS-PD scores in Step 3. The finding that IU total scores changed from a positive to negative association with IDAS-PD scores from Step 2 to Step 3 indicated potential variance suppression in the relationship between IU and IDAS-PD scores by the inclusion of the symptoms of other emotional disorders. One known indicator of a suppression effect is when the inclusion of additional independent variables changes the direction of the association between one independent variable and the dependent variable (Tzelgov & Henik, 1991). A similar pattern emerged when examining prospective IU, inhibitory IU, and NBW scores (see Table 4).
Prospective IU scores significantly accounted for variance in PD scores in Step 1, while only NBW scores accounted for significant variance in IDAS-PD scores in Step 2. However, prospective IU scores were significantly negatively associated with IDAS-PD scores in Step 3, while neither inhibitory IU nor NBW scores were associated with IDAS-PD scores in Step 3. The finding that prospective IU scores were significantly negatively associated with IDAS-PD scores in Step 3 again indicated that one or more of the emotional disorder symptom scores entered in Step 3 were having a suppression effect (Beckstead, 2012; Tzelgov & Henik, 1991). Step 1 accounted for 17.4% of the variance in IDAS-PD scores, F(2, 503) = 53.10, p < .001, while Step 2 accounted for an additional 14.2% of variance, F(1, 502) = 104.67, p < .001. Step 3 accounted for an additional 26.3% of the total variance in IDAS-PD scores, F(6, 496) = 51.63, p < .001.
Additional regression analyses were conducted to explore which factors might have caused the potential suppression effect that occurred with the IU total and prospective IU scores. These analyses, which are not reported here in the sake of brevity, indicated that the inclusion of multiple IDAS subscale scores, though particularly the IDAS-SA scores, may have increased the absolute value of the beta weights for the IU total and prospective IU scores from Step 2 to Step 3. Further, the inversion of the beta weights for the IU total and prospective IU scores appeared to be primarily due to the inclusion of both IDAS-DEP and IDAS-SA scores in Step 3. However, it should be noted that while the increased and inversed beta weights for the IU total and prospective IU scores were found to be statistically significant, other indicators of suppression were not evident (e.g., part correlations larger than regression coefficients; partial correlation with opposite directions of association in comparison to part correlations; Akinwande et al., 2015; Beckstead, 2012). Further, regarding IU total scores specifically, the increased association between IU total scores and IDAS-PD scores from Step 2 to Step 3 was small (Δβ = 0.01). A larger increase in the absolute value of the beta weight would be expected with a clear suppression effect (Thompson & Levine, 1997; Tzelgov & Henik, 1991).
With IDAS-PTSD scores as the dependent variable, both IU total and NBW scores accounted for a significant amount of variance in post-traumatic stress symptoms in Step 2, but not Step 3 (see Table 3). Step 1 accounted for 20.8% of the variance in IDAS-PTSD scores, F(1, 504) = 132.61, p < .001, and Step 2 accounted for an additional 8.5% of variance, ΔF(1, 503) = 60.72, p < .001. Step 3 accounted for an additional 16.3% of the total variance in IDAS-PTSD scores, ΔF(6, 497) = 24.93, p < .001. IDAS-DEP, IDAS-PD, and OCI-R scores significantly accounted for variance in IDAS-PTSD scores. When examining prospective IU, inhibitory IU, and NBW scores, only prospective IU scores significantly accounted for variance in IDAS-PTSD scores in Step 1, only NBW scores significantly accounted for variance in IDAS-PTSD scores in Step 2, and neither variable accounted for significant variance in Step 3 (see Table 4). Step 1 accounted for 20.9% of the variance in IDAS-PTSD scores, F(2, 503) = 66.57, p < .001, while Step 2 accounted for an additional 8.5% of variance, ΔF(1, 502) = 60.49, p < .001. Step 3 accounted for an additional 16.3% of the total variance in IDAS-PTSD scores, ΔF(6, 496) = 24.83, p < .001.
With OCI-R scores as the dependent variable, both IU total and NBW scores accounted for a significant amount of variance in obsessive-compulsive symptoms in Step 2 (see Table 3). Step 1 accounted for 31.2% of the total variance in OCI-R scores, F(1, 504) = 228.20, p < .001, and Step 2 accounted for an additional 4.9% of the variance in OCI-R scores, ΔF(1, 503) = 38.71, p < .001. IU total scores, IDAS-DEP, IDAS-SA, IDAS-PTSD, and SHAI scores significantly accounted for variance in OCI-R scores in Step 3, while NBW scores became nonsignificant. Step 3 accounted for an additional 6.9% of the total variance in OCI-R scores, ΔF(6, 497) = 10.07, p < .001. When examining prospective IU, inhibitory IU, and NBW scores, inhibitory IU scores significantly accounted for variance in OCI-R scores in addition to the comorbid emotional disorder symptoms (see Table 4). NBW scores were significant in Step 2, but not Step 3. Step 1 accounted for 31.2% of the variance in OCI-R scores, F(1, 503) = 113.89, p < .001, while Step 2 accounted for an additional 5.2% of variance, ΔF(1, 502) = 40.81, p < .001. Step 3 accounted for an additional 16.3% of the total variance in OCI-R scores, ΔF(6, 496) = 10.05, p < .001.
With SHAI scores as the dependent variable, both IU total and NBW scores accounted for a significant amount of variance in illness anxiety symptoms in Step 2, but not Step 3 (see Table 3). Step 1 accounted for 22.1% of the variance in SHAI scores, F(1, 504) = 142.64, p < .001, and Step 2 accounted for an additional 7.8% of variance, ΔF(1, 503) = 56.17, p < .001. Step 3 accounted for an additional 9.4% of the total variance in SHAI scores, ΔF(6, 497) = 12.79, p < .001. GADQ-IV, IDAS-PD, and OCI-R scores significantly accounted for variance in SHAI scores. When examining prospective IU, inhibitory IU, and NBW scores, prospective IU scores and NBW scores significantly accounted for variance in SHAI scores in Step 2, but not Step 3 (see Table 4 ). Step 1 accounted for 23.1% of the variance in SHAI scores, F(1, 504) = 75.52, p < .001, and Step 2 accounted for an additional 7.0% of variance, ΔF(1, 502) = 50.39, p < .001. Step 3 accounted for an additional 9.3% of the total variance in SHAI scores, ΔF(6, 497) = 12.76, p < .001.
Since our main analyses included IU and NBW scores in Step 1, it is possible that the IU and NBW scores would not have accounted for significant variance in the dependent variables if the other emotional disorder symptoms had been controlled for in Step 1. To confirm that IU total and NBW scores, or prospective IU, inhibitory IU, and NBW scores, accounted for significant variance in the dependent variables above and beyond the overlapping symptoms, we reran all of the previous analyses with emotional disorder symptoms in Step 1 and IU total or subscale scores and NBW in Step 2 (see Supplementary Materials, Tables S2 and S3). When GADQ-IV, IDAS-DEP, IDAS-SA, IDAS-PD, or OCI-R scores were entered as dependent variables, IU total and NBW scores, or prospective IU, inhibitory IU, and NBW scores, accounted for a significant increase of approximately 1–6% in explained variance beyond the other emotional disorder symptoms that were controlled for in Step 1. Since all of the variables are included in Step 2 of the reversed analyses, the specific associations between IU total scores, prospective IU and inhibitory IU scores, and NBW scores are identical to the results shown in Step 3 in Tables 3 and 4. Step 2 of the reversed analyses was not significant for IDAS-PTSD scores and SHAI scores since, as indicated Tables 3 and 4. IU total, prospective IU, inhibitory IU, and NBW scores were not uniquely related to post-traumatic stress disorder and illness anxiety disorder symptoms once the other symptoms were included.
Discussion
To our knowledge, our study is the first to examine the unique associations of both IU and NBW across several emotional disorder symptoms while controlling for symptom overlap. Our study is also the first to examine prospective IU and inhibitory IU alongside NBW. Together, IU and NBW accounted for approximately 50% of the variability in generalized anxiety disorder and depression symptoms, 45% of the variability in social anxiety disorder symptoms, 36% of the variability in obsessive-compulsive symptoms, and approximately 30% of the variability in panic disorder, post-traumatic stress disorder, and illness anxiety disorder symptoms. Both IU and NBW accounted for significant unique variance in each of the emotional disorders, which supports the transdiagnostic nature of both IU and NBW (Carleton, 2016; McEvoy & Mahoney, 2013). However, once we accounted for symptom overlap and utilized prospective IU and inhibitory IU, more specific associations emerged.
Aligning with previous research, both IU (Boelen & Reijntjes, 2009; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011) and NBW (Hirsch et al., 2013; Penney et al., 2013) were associated with generalized anxiety disorder symptoms, even when controlling for symptom overlap. When examining the magnitude of the relationships between each factor and generalized anxiety disorder symptoms, it is clear that NBW are more strongly associated with generalized anxiety disorder symptoms. Therefore, our study converges with prior research that indicates that while NBW is transdiagnostic, it does appear to be particularly associated with generalized anxiety disorder (Spada et al., 2008; Wells & Carter, 2001), even when IU is accounted for (Khawaja & McMahon, 2011; Koerner et al., 2015; Ruggiero et al., 2012; Thielsch et al., 2015; van der Heiden et al., 2010; Voon & Phillips, 2015). The association between NBW and generalized anxiety disorder symptoms also supports Wells’s (1995, 2009) metacognitive model of generalized anxiety disorder, which argues that NBW and meta-worry are the driving factors in the development and maintenance of generalized anxiety disorder.
While not contributing as strongly, IU was also associated with generalized anxiety disorder symptoms. Since inhibitory IU was not associated with generalized anxiety disorder symptoms in our study, it appears that prospective IU largely accounts for the relationship between IU and generalized anxiety disorder symptoms, which corroborates with the conclusions of prior research (Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011). The association between IU and generalized anxiety disorder symptoms offers partial support for Dugas’s IU model of generalized anxiety disorder (Dugas et al., 1998; Dugas & Koerner, 2005), which argues that IU is a central factor that leads to impairment and distress in generalized anxiety disorder. As individuals high in prospective IU appear to desire a predictable future as a means to avoid uncertainty (Hong & Lee, 2015), it is not surprising that prospective IU is related to generalized anxiety disorder symptoms, given that worry is used in an attempt to solve future potential problems (Gladstone & Parker, 2003).
Both IU and NBW were associated with depression symptoms when no other emotional disorder symptoms were included. However, once the other emotional disorder symptoms were controlled, IU was no longer associated with depression symptoms. Likewise, while prospective IU was associated with depression symptoms initially, it was no longer associated with depression symptoms once the other emotional disorder symptoms were included. The result that IU was no longer associated with depression once the other emotional disorder symptoms were controlled was unforeseen, given that research has consistently associated IU with depression (Boelen & Lenferink, 2018; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011; Saulnier et al., 2019). However, the previous studies did not control for as many emotional disorder variables as in the present study while also including NBW. NBW accounted for most of the variance in depression symptoms in Step 2 of the regression equations and continued to be associated with depression symptoms in Step 3.
Both IU and NBW were associated with social anxiety symptoms, even when the other emotional disorder symptoms were included. An association between NBW and social anxiety symptoms supports existing research (McEvoy et al., 2009; McEvoy & Perini, 2009). The results that NBW were associated with both depression and social anxiety disorder symptoms, in addition to generalized anxiety disorder symptoms, support the argument that NBW should be considered a transdiagnostic factor amongst anxiety and depression disorders (Nordahl et al., 2019; Spada et al., 2008). The associations between NBW and depression, social anxiety, and generalized anxiety disorder symptoms also provide support for Wells’s (2009) proposed cognitive attentional syndrome (CAS). The CAS is defined by excessive worry and rumination, where the individual is often trapped in self-focused negative repetitive thoughts, which can give rise to attentional bias toward threat related information (Fergus et al., 2013; Wells & Carter, 1999, 2001). It appears that NBW might be a foundational belief that drives the CAS within generalized anxiety disorder, depression, and social anxiety disorder.
Although NBW was associated with social anxiety disorder symptoms, IU retained a stronger association with social anxiety symptoms once the other symptoms were controlled. When IU was separated into prospective IU and inhibitory IU, only inhibitory IU was associated with social anxiety symptoms. Again, our results support the existing research that IU, particularly inhibitory IU, is associated with social anxiety symptoms (Boelen & Lenferink, 2018; Carleton et al., 2010; Hong & Lee, 2015; Mahoney & McEvoy, 2012a, 2012b; McEvoy & Mahoney, 2011; Whiting et al., 2014). It appears that IU might be a driving factor in the avoidance and behavioral inaction apparent in social anxiety disorder, which could be particularly true for performance-related social anxiety (Carleton et al., 2010; Whiting et al., 2014).
Aligning with the existing research, both IU (Boelen & Reijntjes, 2009; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011) and NBW (Cucchi et al., 2012; Wells & Cartwright-Hatton, 2004; Wells & Papageorgiou, 1998) were associated with obsessive-compulsive disorder symptoms when no other emotional disorder symptoms were included. However, NBW was no longer associated with obsessive-compulsive disorder symptoms once the other emotional disorder symptoms were controlled. IU retained a significant association with obsessive-compulsive disorder symptoms, and separating IU into prospective IU and inhibitory IU revealed that only inhibitory IU contributed to the relationship. While obsessive-compulsive disorder is usually associated with prospective IU (McEvoy & Mahoney, 2011), some researchers have also found links between inhibitory IU and obsessive-compulsive disorder (Boelen & Lenferink, 2018; Jacoby et al., 2013; Mahoney & McEvoy, 2012b). Results of the current study lend support to inhibitory IU being associated with symptoms of obsessive-compulsive disorder and are consistent with the idea that individuals with obsessive-compulsive disorder symptoms and high inhibitory IU might become behaviorally paralyzed or “stuck” when faced with uncertainty (Hong & Lee, 2015; Jacoby et al., 2013).
The most surprising result was that when emotional disorder symptoms were controlled for, IU, and specifically prospective IU, was negatively associated with panic disorder symptoms. The increased beta weights, as well as the change in direction, for IU and prospective IU with panic disorder symptoms indicated potential suppression effects. If the negative association between IU and panic disorder symptoms is due to suppression effects, this would indicate that that result does not represent the true relationship between IU and panic disorder symptoms. Suppression effects in multiple regression arise when the inclusion of an independent variable enhances the predictive value of another independent variable with the dependent variable of interest, through “suppressing” irrelevant variance that is not associated with the dependent variable (Thompson & Levine, 1997). Generally, sources of suppression are identified through examining beta weights, directionality of associations, and part/partial correlations of independent variables hierarchically with the inclusion of each other independent variable separately (Akinwande et al., 2015). Suppression effects are not common in psychological research, and sources of suppression become increasingly difficult to identify in multiple regression analyses, especially with the inclusion of multiple independent variables, such as in the current study (Thompson & Levine, 1997; Tzelgov & Henik, 1991). In the current study, the potential suppression in the association of IU with panic disorder symptoms may have been due to a combination of independent variables, particularly depression and social anxiety scores, both of which were IDAS subscales. However, clearly definitive indicators of suppression, as discussed by Thompson and Levine (1997) and Tzelgov and Henik (1991), were not evident, so the present analyses were retained.
Generally, past research has shown positive associations between general IU and panic disorder (Carleton et al., 2014; Mahoney & McEvoy, 2012a), with inhibitory IU being specifically associated with panic disorder (Carleton et al., 2013, 2014; McEvoy & Mahoney, 2011). However, a negative association between IU and startle response in an uncertain situation has been previously documented (Nelson & Shankman, 2011). Yet, further research revealed the negative association appeared to be attributable to inhibitory IU, while prospective IU had a positive association with startle response in an uncertain situation (Nelson et al., 2016). It might be possible that a negative association between IU and panic disorder symptoms can only be found once other emotional disorder symptoms are controlled for, though as previously stated, the negative association might be due to suppression rather than being indicative of the true relationship between IU and panic disorder symptoms. Further exploration of the relationship between IU and panic disorder, with the influence of other emotional disorders removed, is needed. If the negative association is replicated, it could indicate that by attempting to anticipate future negative events, individuals with high prospective IU might be able to successfully decrease their chances of experiencing anxious arousal or panic attacks, though this is clearly speculative. While initially associated with panic disorder symptoms, NBW was no longer significantly associated with panic disorder symptoms upon inclusion of the other symptoms.
For symptoms of both post-traumatic stress disorder and illness anxiety disorder, both IU and NBW did not account for unique variance once the other emotional disorder symptoms were included. While previous research has indicated that post-traumatic stress disorder and illness anxiety disorder are associated with both prospective IU and inhibitory IU (Boelen et al., 2016; Fetzner et al., 2013, 2014; Raines et al., 2019; Wright et al., 2016) and NBW (Bailey & Wells, 2015; Roussis & Wells, 2006), these studies have tended to include few measures of other emotional disorder symptoms. Therefore, the apparent associations between IU and NBW with post-traumatic stress disorder and illness anxiety disorder might be due to mutual associations with the other emotional disorders. Additional studies that control for potential contamination by the other emotional disorder symptoms while examining the relationships between IU and NBW with post-traumatic stress disorder and illness anxiety disorder are warranted.
Overall, the results of our current study highlight the distinct associations between IU and NBW with emotional disorder symptoms. Our results also contribute to the existing body of literature demonstrating that prospective and inhibitory aspects of IU differentiate emotional disorder symptoms and are meaningfully different constructs (Boelen & Lenferink, 2018; Bottesi et al., 2019; Fetzner et al., 2013, 2014; Hong & Lee, 2015; Jensen et al., 2016; Mahoney & McEvoy, 2012a; McEvoy & Mahoney, 2011; Raines et al., 2019; Shihata et al., 2018; Wright et al., 2016). Further, our results demonstrate the importance of considering NBW in addition to IU when examining relationships with emotional disorders and support the idea that NBW are both transdiagnostic and specific across various emotional disorders (Khawaja & McMahon, 2011; Koerner et al., 2015; van der Heiden et al., 2010).
While our results indicate that IU and NBW have differential relationships with emotional disorder symptoms, Hong and Cheung (2015) found that conceptually distinct cognitive factors, including IU, ruminative style, and anxiety sensitivity, appear to be variations of a broader transdiagnostic cognitive vulnerability that is associated with emotional disorders. Based on Hong and Cheung’s (2015) conclusions, it could be possible that NBW are another component of the proposed transdiagnostic cognitive vulnerability. However, according to Wells’s (2009) self-regulatory executive function model, metacognitive beliefs (i.e., beliefs about one’s thought process) form a separate, overarching, system from one’s cognitive beliefs (i.e., day-to-day thoughts about the self, others, and the world). Therefore, metacognitive beliefs such as NBW might be part of a transdiagnostic factor that is separate from the types of cognitive beliefs underlying the transdiagnostic cognitive vulnerability articulated by Hong and Cheung (2015). Additional research is needed to determine the relationship between IU and NBW. Longitudinal research would assist in clarifying if IU leads to NBW, if NBW leads to IU, or if there is a reciprocal relationship between the two.
In addition to having implications for research, the results of the present study are clinically relevant. While researchers have begun to elucidate prospective and inhibitory IU in the treatment of specific emotional disorders (Stevens et al., 2017), the results of the current study also highlight potential differentiating and contributing factors that might be of clinical importance across multiple disorders. For instance, in addition to targeting NBW in the treatment of social anxiety disorder, individuals might benefit from exposure and behavior-based therapies targeting the avoidance associated with inhibitory IU. Conversely, when treating generalized anxiety disorder, individuals might benefit from cognitive-based therapies targeting NBW and appraisals of future uncertainties associated with prospective IU. Further, while recently developed transdiagnostic treatment protocols have been shown to decrease IU (Boswell et al., 2013) and negative metacognitive beliefs (Callesen et al., 2019), it would be interesting to examine whether creating a transdiagnostic treatment protocol specifically targeting both IU and NBW would improve outcomes.
Limitations
Limitations of our study include the use of a nonclinical sample and the cross-sectional design. Since we utilized a nonclinical sample, the extent to which conclusions drawn from our study generalize to a clinical population is unclear. The present study did, however, include measures that have been validated for use in nonclinical samples. Additionally, researchers have argued the use of large undergraduate student samples to be appropriate in understanding emotional disorders (Asmundson et al., 2012; Tull et al., 2008). Further research should be conducted to examine the specific longitudinal relationships between IU and NBW and emotional disorders, as the cross-sectional nature of the current study cannot determine how IU and NBW contribute to the development and maintenance of the symptoms of emotional disorders.
Additional limitations of the current study concern the selected measures of emotional disorder symptoms. For instance, some of the measures of emotional disorders used in the present study have evidenced a factor structure where general scores are composed of varying subsets of symptoms. For example, the SHAI has demonstrated a factor structure including “Illness Likelihood,” “Illness Severity,” and “Body Vigilance” (Abramowitz et al., 2007), while the OCI-R has demonstrated factors including “Checking,” “Hoarding,” and “Neutralizing” (Foa et al., 2002), which were not considered for the purposes of our study. Examining specific factors of emotional disorders might have yielded alternative results. A related limitation concerns the length of some of the measures. For example, the IDAS-SA subscale includes only 5 items, while the IDAS-PTSD subscale includes only 4 items. More comprehensive questionnaires might have also led to differing conclusions. Despite the identified limitations, the psychometric properties of the SHAI, OCI-R, IDAS-SA, and IDAS-PTSD provide support for the use of the scores examined in our study.
Another limitation stems from ongoing debate regarding whether only the IUS-12 total score should be used or if scores from the prospective and inhibitory IU subscales are acceptable (Hale et al., 2016; Saulnier et al., 2019; Shihata et al., 2018; Yao et al., 2020). While some researchers have found substantial support for a bifactor model for the IUS-12 and have argued that only the total score should be retained for research purposes (Hale et al., 2016; Shihata et al., 2018), other researchers have argued that differentiating the prospective and inhibitory aspects of IU provides clinically relevant and meaningful information and can continue to be explored (Boelen & Lenferink, 2018; Hong & Lee, 2015; Saulnier et al., 2019; Yao et al., 2020). We retained the prospective and inhibitory IU subscales of the IUS-12 for the purposes of the current study given the theoretical and empirical support to do so, while choosing to also report the results for the IUS-12 total score. However, there have been significant concerns raised about the item selection process and content validity of the IUS-12, and Hong and Lee (2015) proposed a revised 18-item version of the IUS (IUS-18) to address the concerns. Additional studies examining the psychometric properties and validity of the IUS-12 and IUS-18 have significant implications for both future research designs and our theoretical understanding of IU.
The potential suppression effects that were found in the negative associations of IU with panic disorder symptoms present a final limitation. Often, suppression situations in psychological research fail to be replicated (Tzelgov & Henik, 1991). Therefore, the results of the current study in relation to the negative associations of IU with panic disorder symptoms should be interpreted with caution.
Conclusion
Overall, our results provide further evidence that the transdiagnostic factors of IU and NBW have unique differential associations to emotional disorders. While IU was associated with generalized anxiety disorder, social anxiety disorder, and obsessive-compulsive disorder symptoms, and negatively associated with panic disorder symptoms, NBW was associated with generalized anxiety disorder, depression, and social anxiety disorder symptoms. The results of our study also further demonstrate the value of considering the two-factor model of IU of prospective IU and inhibitory IU. Lastly, our results emphasize the importance of separating and controlling for overlapping symptoms across disorders.
Supplemental material
IUNB_Publication_SupplementaryTables(JEP)_Revision2 - Differentiating the roles of intolerance of uncertainty and negative beliefs about worry across emotional disorders
IUNB_Publication_SupplementaryTables(JEP)_Revision2 for Differentiating the roles of intolerance of uncertainty and negative beliefs about worry across emotional disorders by Alexander M. Penney, Geoffrey S. Rachor and Kendall A. Deleurme in Journal of Experimental Psychopathology
Footnotes
Authors’ note
The data sets generated and/or analyzed during the current study are not publicly available due to ethics restrictions but are available from the corresponding author, Alexander M. Penney, on reasonable request.
Acknowledgments
We would like to thank Shelby Werezak and Christine O’Brien for their assistance in data cleaning and analyses during preliminary analyses and dissemination. We would also like to thank our peer reviewers for their insightful comments that led to substantial revisions to our initial manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The present study was reviewed and approved by MacEwan University’s Research Ethics Board (File No: 100228).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.