
Abstract
We investigate the impact of maternal ethnic–racial identity on child internalizing trajectories in immigrant and U.S.-born Latinx families. Data from N=1,076 Latinx mothers’ reports at child ages 1, 3, 5, and 9 years were used. For children of U.S.-born mothers, but not immigrant mothers, greater levels of maternal ethnic–racial identity were associated with lower levels of internalizing symptoms at age 3, yet attenuated decreases in internalizing symptoms over time. Thus, mother’s ethnic–racial identity was a protective factor for children at preschool age but became less protective through school age. Our results suggest that incorporating ethnic–racial identity elements, particularly for U.S.-born mothers of toddlers to preschoolers, may be an important consideration when designing interventions for Latinx families.
Ethnic and racial minorities in the USA, such as Latino/a/x (hereafter referred to Latinx) populations, often experience additional stressors not shared by their White counterparts that increase their likelihood of experiencing depression and/or anxiety symptoms (Cano et al., 2016; Perez et al., 2008). A strong ethnic–racial identity, however, is one factor that may buffer against negative psychological effects that ethnic–racial minorities face, as research with adults and adolescents has shown that strong ethnic–racial identity relates to better psychological outcomes (Rivas-Drake, Seaton, et al., 2014; Umaña-Taylor et al., 2014). On the other hand, parental, and especially maternal, characteristics (i.e., depression and anxiety) have been shown to increase children’s internalizing (anxiety/depression) symptoms (Beardslee et al., 2011; Goodman et al., 2011; Kingston et al., 2018). Yet, the degree to which maternal ethnic–racial identity influences children’s psychological outcomes is unknown. Identifying the role of maternal ethnic–racial identity in children’s mental health development addresses a potentially important opportunity for intervention in a traditionally underserved population, that is, Latinx ethnic minorities.
The current study addresses this gap in the literature by examining the potential impact of maternal ethnic–racial identity on children’s internalizing trajectories. We focus on Latinx mothers for the current investigation, as the Latinx population is the largest minority group in the U.S., with 1 in 4 children being Latinx (Murphey et al., 2014), and represents an opportunity to characterize the protective factors for this often-underserved population. In addition, we examine the potential moderating role of immigrant status of the mothers, as prior research suggests that the first- and second-generation immigrants view ethnic–racial identity differently (Almeida et al., 2016; Perez et al., 2008). Lastly, we explore potential mediators (maternal depression, parenting) of the effect of maternal ethnic–racial identity on child internalizing, as these maternal factors have previously been shown to affect child psychopathology (Wiggins et al., 2014, 2015).
Ethnic–racial identity
Ethnic–racial identity is an important component of healthy development for ethnic and racial minority individuals (Umaña-Taylor et al., 2014). Earlier, scholars distinguished between one’s ethnic identity (which referred to one’s feelings of belonging to a particular ethnic group) and one’s racial identity (pertaining to one’s identification with their racial group). Not seeing clear distinctions and observing many overlapping qualities, scholars, in more recent years, have combined the two, referring to ethnic–racial identity (Umaña-Taylor et al., 2014). This broader label is more encompassing and more accurately reflects the experiences of many ethnic–racial minorities. More thorough descriptions of the ethnic–racial identity construct have been previously published (e.g., Umaña-Taylor et al., 2014). For the scope of this article, and based on the measure used to assess the construct, we define ethnic–racial identity as the degree to which one identifies with and participates in one’s ethnic–racial group.
Prior research has shown that ethnic–racial identity often serves as a protective factor for Latinx populations in the U.S. (Brittian et al., 2015; Gonzales-Backen et al., 2017; Rivas-Drake, Seaton, et al., 2014). Most of what is known about ethnic–racial identity’s buffering aspects comes from research with adolescents and young adults, since those developmental periods are considered important for identity exploration (Rivas-Drake, Seaton, et al., 2014). There are consistent patterns between strong ethnic–racial identity and adaptive outcomes during adolescence and young adulthood (Rivas-Drake, Seaton, et al., 2014). For example, studies show that strong ethnic–racial identity is a protective factor against depression and anxiety in young adulthood and adolescence (Brittian et al., 2015; Rivas-Drake, Syed, et al., 2014) and serves an important role for overall psychosocial adjustment for youth of color (Gonzales-Backen et al., 2016; Rivas-Drake, Syed, et al., 2014). A more emergent literature with preschool-age Latinx children is finding similar protective aspects of ethnic–racial identity (Serrano-Villar & Calzada, 2016). It should be noted that although much of the research points to a protective nature of ethnic–racial identity, some studies do not find ethnic–racial identity improves psychosocial outcomes (Kiang et al., 2006; Le et al., 2009; Schwartz et al., 2007). Of note, prior studies did not trace the developmental timing of either ethnic–racial identity or psychological constructs, leaving open the question as to whether ethnic–racial identity may have differing effects on psychopathology symptoms across development.
Importantly, there seem to be differences between immigrants and U.S.-born ethnic/racial minority individuals in terms of their experiences with ethnic–racial identity in the larger, mainstream U.S. society (Lee, 2005; Perez et al., 2008; Yoo & Lee, 2009). Second-generation ethnic–racial minorities are individuals from a particular ethnic–racial group who were born in the U.S. to one or more immigrant parents. Second-generation individuals have greater awareness of poor and differential treatment from the majority culture than their first-generation counterparts (i.e., foreign-born immigrants) (Almeida et al., 2016; Arellano-Morales et al., 2015; Perez et al., 2008; Wiley et al., 2012), which may contribute to such differences with ethnic–racial identity. One explanation is that U.S.-born minorities are in a better position to recognize their status of “other” in the larger, mainstream American society, which immigrants often are not able to identify as easily (Perez et al., 2008). This can translate into U.S.-born ethnic–racial minorities having greater awareness of their own ethnic–racial identity due to this differential treatment. Thus, ethnic–racial identity may serve as a protective factor against feelings of otherness and unfair treatment because ethnic–racial minorities feel the need to belong to their group, given that they are “othered” by the mainstream majority group (Baldwin-White et al., 2017). On the other hand, since many U.S.-born minorities are better able to identify discrimination, greater ethnic–racial identity may not as clearly be a positive thing for them, as greater ethnic–racial identity may be associated with more unfair treatment (Lee, 2005; Yoo & Lee, 2009). While the complexity of ethnic–racial identity is still being understood, what is clear from both of these lines of research is that immigrant status must be considered, as U.S.-born individuals perceive or experience ethnic–racial identity differently compared to immigrants.
Maternal characteristics and child internalizing symptoms
In addition to prior work showing that ethnic–racial identity is important for psychosocial outcomes, at least for adults/adolescents, parental—particularly maternal—characteristics are among the strongest predictors of child psychosocial outcomes, including internalizing symptoms in early- to middle-childhood. This is true for mothers in the general population (Beardslee et al., 2011; Kuckertz et al., 2017; Wiggins et al., 2015) as well as Latinx mothers (Zeiders et al., 2016). Thus, to understand and effectively treat child symptoms, it will be important to characterize the maternal traits and behaviors that may contribute to child outcomes. Previous studies have shown that maternal depression, anxiety, as well as a variety of other maternal characteristics (e.g., education, socioeconomic status, etc.) contribute to child internalizing symptoms (Beardslee et al., 2011; Wiggins et al., 2015) and may be mediated by parenting behaviors (Kuckertz et al., 2017; Wiggins et al., 2015). Of note, these previous studies showed that maternal influences may vary across children’s development. For example, Wiggins et al. (2014) showed that maternal characteristics were less influential on children’s psychopathology symptoms in middle childhood versus toddlerhood. Thus, a developmental approach, which considers trajectories across multiple time points, will be important in investigating maternal influences of ethnic–racial identity on children.
Many studies suggest that maternal ethnic–racial identity affects children’s psychological outcomes. Specifically, when mothers devote effort to cultural socialization, their children are more likely to explore their own ethnic–racial identity (Juang & Syed, 2010; Knight et al., 2017) and subsequently demonstrate higher overall self-efficacy (Knight et al., 2017). This effect of maternal ethnic socialization on child psychological outcomes was documented not only in Latinx adolescents (Knight et al., 2017) but also Latinx children as young as 5 years old (Derlan et al., 2017). Although previous studies showed that ethnic–racial identity buffers one’s own depression and anxiety in adults, and a large literature showing that maternal characteristics have great influence on children, no study has yet examined the impact of maternal ethnic–racial identity on child psychopathology. It may be that mothers’ ethnic–racial identity affects their mental health and/or parenting, which in turn affects children’s internalizing symptoms.
The current study
Our goal was to investigate the impact of mothers’ ethnic–racial identity on their children’s internalizing symptoms. We characterized immigrant and U.S.-born Latinx mothers’ ethnic–racial identity in relation to child internalizing symptom trajectories from preschool age (i.e., age 3) to school age (i.e., age 9). Based on previous research, we hypothesized that maternal ethnic–racial identity would serve as a protective factor for child internalizing symptoms. Moreover, we expected that the protective nature of maternal ethnic–racial identity would be stronger for children of U.S.-born versus immigrant mothers. As a secondary goal, we also explored potential mediators of the relationship between maternal ethnic–racial identity and internalizing symptoms, including maternal depression and parenting.
Method
Participants and procedures
Data for this study came from the Fragile Families and Child Wellbeing Study (Reichman et al., 2001), a large, longitudinal, population-based study of predominantly low-income children born between 1998 and 2000 in 18 large U.S. cities. The participants were recruited by approaching families after the child’s birth at hospitals in major urban centers with populations >200,000. This sample contained representation from all segments of the population and was enriched for risk for child psychopathology by oversampling nonmarital births. The overarching goal of the Fragile Families and Child Wellbeing Study was to examine the role of the social and family environment on child development. The present study used data from mother (primary caregiver) in-home and phone interviews at child ages 1, 3, 5, and 9 years. Of the 4,898 families recruited at birth, 1,333 (27%) mothers self-identified as Latino or Hispanic. Little over half of the mothers (59%) were born in the U.S. Those mothers who were born elsewhere had lived in the U.S. on average 26 years (SD = 6.97). Questionnaires were available in English and Spanish.
Of the overall sample from the current study, N = 1,076 (81%) completed the ethnic–racial identity measure at child age 1 and had at least one time point of child symptom data and thus were included in analyses. Child symptom data were collected on 70%, 73%, and 68% of children of Latinx mothers with ethnic–racial identity data at ages 3, 5, and 9; because of this, we used the expectation maximization algorithm to address missing data (see “Analytic plan” section). The structure of missing data patterns was the same for immigrant and U.S.-born mothers. Maternal education was related to number of time points missing for child internalizing (χ2 = 21.89, df = 1, p = .009) but not for child gender (χ2 = 4.33, df = 1, p = .228) or maternal age (F 3,1328 < 1). Subsequent analyses nevertheless controlled for sociodemographic characteristics. Sample characteristics are available in Table 1.
Sample characteristics and descriptive statistics for study variables.
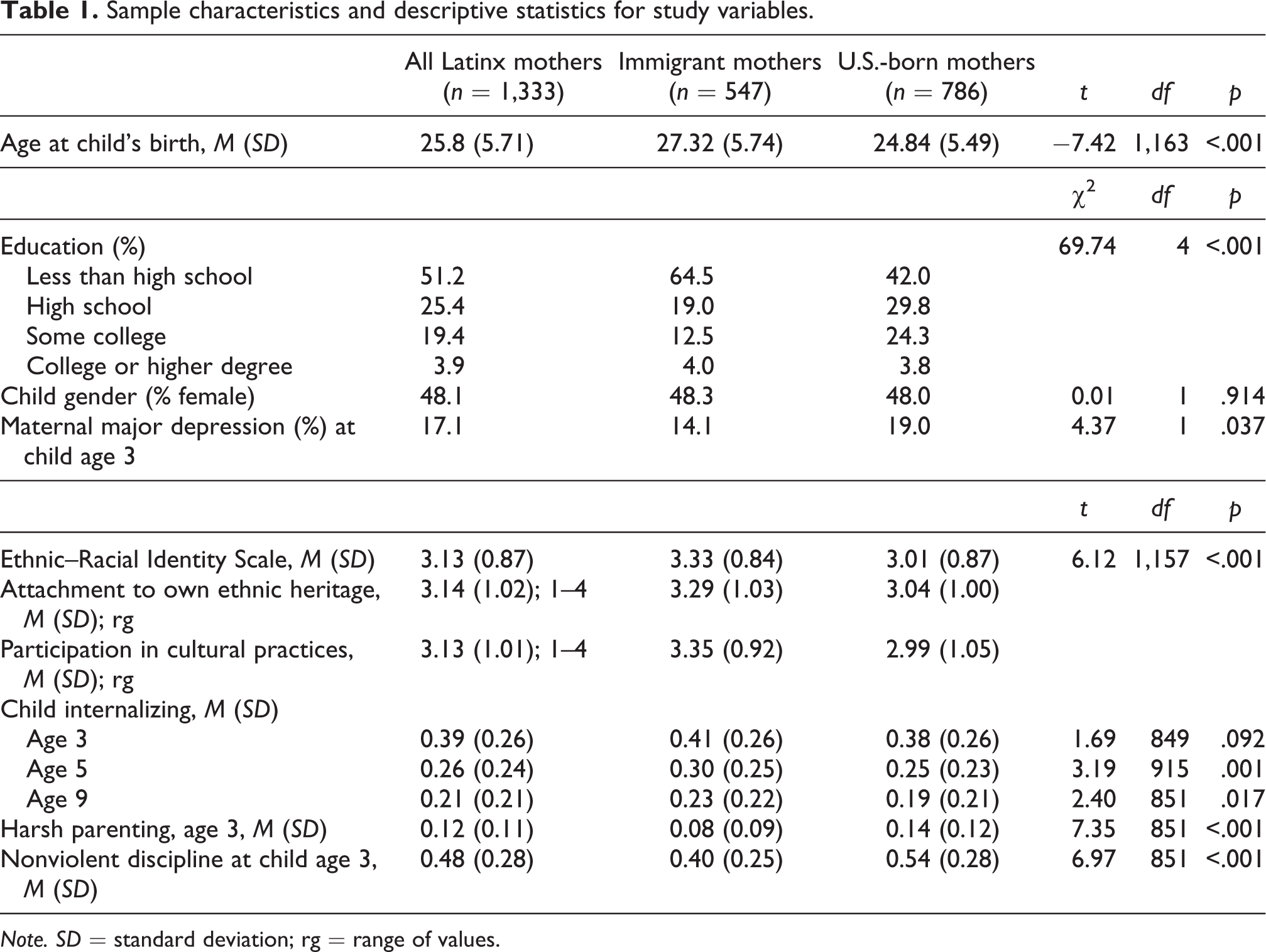
Note. SD = standard deviation; rg = range of values.
Measures
Child internalizing symptoms
Internalizing symptoms were assessed using the Child Behavior Checklist (CBCL). The CBCL/2-3 (toddler) version (Achenbach, 1992) was collected at age 3, CBCL/4-18 (Achenbach, 1991) at age 5 (the current school-age version at the time), and CBCL/6-18 (Achenbach & Rescorla, 2001) (the most recent version) at age 9. The internalizing subscale was utilized (Cronbach’s αs = .75, .75, and .84 for 16, 23, and 21 items at ages 3, 5, and 9, respectively). Mothers were asked to respond on a 0–2 scale with anchors of “never true,” “sometimes or somewhat true,” or “very true or often true” to statements querying child symptoms (e.g., “unhappy, sad, or depressed”). This scale has been widely used to assess child behavior symptoms and has been previously used with Latinx families (Hungerford et al., 2015; Mendoza et al., 2017; Yildirim & Roopnarine, 2015). Mean item scores were computed to represent the subscale at each age, and thus, the overall internalizing subscale ranged from 0 to 2. Although different versions of the CBCL were administered across ages, the constructs that they measure are similar; moreover, the CBCL/2-3 (toddler) version includes modifications to probe these symptoms in a developmentally appropriate manner. To remain consistent with the CBCL/2-3 and CBCL/4-18, and as done previously (Kuckertz et al., 2017; Wiggins et al., 2015), we used the internalizing subscale (anxious/depressed, withdrawn/depressed) without somatic symptoms for the CBCL/6-18 (age 9).
Ethnic–racial identity
The Fragile Families and Child Wellbeing Study administered 2 items from the Multigroup Ethnic Identity Measure (MEIM; Phinney, 1992), asking each mother to indicate the amount of attachment toward her ethnic heritage and the amount of participation in cultural practices of one’s own group, such as special food, music, or customs. These items both load strongly on the underlying “ethnic–racial identity” factor (Phinney, 1992) but also represent subscales “ethnic–racial identity search/cognitive component” and “affirmation, belonging, commitment/affective component” (Roberts et al., 1999). Answer choices ranged from 1 (strongly disagree) to 4 (strongly agree). We averaged the 2 items into an overall ethnic–racial identity score, which yielded a Cronbach’s α of .61. Having only 2 items available for the scale is certainly a limitation (see “Discussion” section). However, this scale was used in conjunction with the large, population-based, longitudinal sample, which mitigated the effects of the reliability score.
Maternal depression
The Composite International Diagnostic Interview—Short Form (Kessler, Andrews, Mroczek, Ustun, & Wittchen, 1998) was administered over the phone and was utilized to assess maternal major depressive episode in the past year at child age 3. Criteria were based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (American Psychiatric Association, 2000). Mothers were assigned a caseness score of 1 or 0, indicating a probable or non-probable case for major depression, based on whether they had reported at least 2 weeks of depressive symptoms lasting at least half the day. This scale has been previously validated with Latinx populations (De Luca et al., 2018; Salas-Wright et al., 2015).
Parenting
The Parent Child Conflict Tactics Scales (Straus, Hamby, Finkelhor, Moore, & Runyan, 1998;) were completed by the mother to assess frequency of a variety of parenting practices in the past year. Data from age 3 were used for this study. This measure includes harsh parenting, comprised of psychological aggression (e.g., shouted at child, called child names) and physical assault (e.g., spanked child, shook child) (Wiggins et al., 2015). The measure also includes nonviolent discipline (e.g., explained why something was wrong, took away privileges) and neglect (e.g., not able to get child food they needed) subscales (Wiggins et al., 2015). Yearly chronicity scores were calculated, which represent a percentage of maximum score for each scale ranging from 0 to 1 (Straus et al., 1998). The scale has been previously used with Latinx populations (Martin et al., 2012; Yildirim & Roopnarine, 2015). Cronbach’s α in the current study for harsh parenting was .74 and nonviolent discipline was .73. Due to a strong floor effect, we did not include the neglect subscale in our analyses.
Analytic plan
Primary goal: Assess impact of ethnic–racial identity in immigrant and second-generation mothers on child internalizing trajectories
To accomplish our primary goal, we utilized growth mixture modeling with known classes (immigrant vs. U.S.-born mothers) and maternal ethnic–racial identity predicting intercept and slope of internalizing symptoms. This model compared the impact of maternal ethnic–racial identity on intercepts (representing internalizing at age 3) and slopes (representing degree of change in internalizing over time) for children of immigrant versus U.S.-born mothers. To address potential effects of attrition, we controlled for the characteristics related to missingness and other demographic variables: maternal age at birth of child, maternal socioeconomic status (operationalized as maternal education: “less than high school,” “high school,” “some college,” “college or higher degree”), and child gender. Moreover, we modeled the data with the preferred method for data that are missing at random (McCartney et al., 2006), in Mplus 8 (Muthen and Muthen, Los Angeles, California, USA) using the expectation maximization algorithm to obtain maximum likelihood estimates with robust standard errors. We considered multiple indices (root mean square of approximation [RMSEA] and confirmatory fit index [CFI]) to confirm acceptable model fit, as these indices are more appropriate for large samples than typical χ2 tests (Bentler & Bonnet, 1980; Fan, Thompson, & Wang, 1999). RMSEA < .08 and CFI > .90 indicate acceptable model fit, and RMSEA < .06 and CFI > .95 indicate excellent model fit (Hu & Bentler, 1999).
Secondary goal: Explore potential mediators of the relationship between maternal ethnic–racial identity and internalizing symptoms
To accomplish our secondary objective, we estimated the indirect effects of maternal depression, harsh parenting, and nonviolent discipline on the relationship between maternal ethnic–racial identity and preschool age internalizing, using bootstrapped confidence intervals in Mplus 8. Because our results (see below) identified early childhood as the period when maternal ethnic–racial identity effects are the strongest as a protective factor for child internalizing, we focused these secondary mediation analyses on this period, including mediators and child internalizing at age 3 and maternal ethnic–racial identity at age 1. Moreover, because our results (see below) identified effects of ethnic–racial identity on child internalizing in U.S.-born mothers only, these analyses were restricted to this set of participants. As we tested three potential mediators (i.e., maternal depression, harsh parenting, and nonviolent discipline), we used a Bonferroni-corrected α value .0167 (.05/3) to determine significance of the indirect total effects in the model.
Results
Primary goal: Examine the impact of ethnic–racial identity in immigrant and U.S.-born mothers on child internalizing symptom trajectories
Fit indices indicated excellent fit for the two-group (immigrant vs. U.S. born) known class model for internalizing growth, including the ethnic–racial identity regressor (RMSEA = .038, CFI = .96). Controlling for maternal ethnic–racial identity, children of immigrant mothers compared to U.S.-born mothers evidenced similar initial levels of internalizing at age 3 (i.e., estimate for intercept, immigrant mothers: B = .526; U.S.-born mothers: B = .497; p > .05). Moreover, both groups demonstrated significant overall decreases in internalizing symptoms over time from ages 3 to 9 (i.e., estimate for slope, immigrant mothers: B = −.136; U.S.-born mothers, B = −.133, both p < .001), controlling for maternal ethnic–racial identity, and the rate of overall decrease did not differ between the two groups (p > .05).
The two-group model additionally identified effects of maternal ethnic–racial identity on trajectories of internalizing symptoms for children of U.S.-born, but not immigrant, mothers (Figure 1). That is, for children of U.S.-born mothers, greater levels of maternal ethnic–racial identity were associated with lower levels of internalizing symptoms at age 3 (B = −.049, p < .001) yet attenuated decreases in internalizing symptoms over time (B = .028, p < .001). By contrast, maternal ethnic–racial identity did not have any bearing on initial levels of internalizing (B = −.019, p > .05) nor on changes in internalizing over time (B = .004, p > .05) for children of immigrant mothers. All effects controlled for maternal age, education, and child gender.

Trajectories of internalizing for children of U.S.-Born Latinx mothers vary by maternal ethnic–racial identity. Note. Low ethnic–racial identity = 1, high ethnic–racial identity = 4.
Secondary Goal: Explore potential mediators of the relationship between maternal ethnic–racial identity and early childhood (age 3) internalizing symptoms
Within the U.S.-born mother group, in which ethnic–racial identity was a protective factor at child age 3, the mediation models for the relationship between maternal ethnic–racial identity and child internalizing via maternal depression, harsh parenting, and nonviolent discipline each showed acceptable overall model fit (see Table 2). However, the indirect effect of each of the potential mediators was not significant after correction.
Mediation models.a

a Potential mediators of the effect of maternal ethnic–racial identity on child internalizing at age 3.
Discussion
The goal of our study was to explore the links between maternal ethnic–racial identity and child internalizing symptoms. Our findings indicate that ethnic–racial identity in nonimmigrant, U.S.-born mothers is a protective factor for child internalizing during the preschool age (i.e., stronger maternal ethnic–racial identity was related to less internalizing at age 3) but becomes less protective for children as they progress from preschool to school age (i.e., stronger maternal ethnic–racial identity was associated with less sharp decreases in internalizing from age 3 to 9). Maternal ethnic–racial identity had an effect on child internalizing above and beyond mother’s education and age, as well as child’s gender, and this link between maternal ethnic–racial identity and child internalizing emerged for U.S.-born, but not immigrant, mothers.
Our findings in Latinx mothers and children have clinical implications for those designing interventions for diverse families and may serve as a model for research on ethnic–racial identity and child outcomes in other minority groups. In particular, our work suggests that maternal ethnic–racial identity may be an important component to consider in interventions for minority groups. Indeed, creating interventions that are specific to population’s needs carries many benefits. Much of the research on child psychopathology is based on White, middle class families or does not explicitly investigate race/ethnicity or components of race/ethnicity such as ethnic–racial identity. Latinx families have experiences and needs that may be different from those of the mainstream majority families. Therefore, designing interventions that address the specific needs of minority populations is essential in ensuring that those needs are met and that those interventions can lead to beneficial psychosocial outcomes for ethnic minority children and their families. Although it will be important to replicate and extend our findings, our research indicates that, to be most effective for children of minorities, and particularly U.S.-born Latinx families, a consideration of maternal ethnic–racial identity may be necessary for interventions.
Our findings moreover indicate that maternal ethnic–racial identity can serve as a protective factor during early stages of developmental period, but its protective effects decrease as the child grows into school age. These findings suggest that the degree to which ethnic–racial identity is a positive aspect might vary by the child’s developmental stage. It may be that when children are very young, stronger maternal ethnic–racial identity leads to more resources, as the mother can rely on her community for help. However, as the child grows older, greater levels of maternal ethnic–racial identity may cause friction, or a sense of “otherness” in the child, as the child interacts with a greater variety of people (e.g., at school) and may experience discrimination or differential treatment due to race/ethnicity. It is also likely that the impact of mother’s identity is strongest when child is young since this is the time period when children tend to spend most of their time with their primary caregiver. Once children become a little bit older, they are likely spending more time with other individuals in their environment (e.g., teachers, peers) who might influence their identity development. Thus, while our findings indicate the importance of maternal ethnic–racial identity, they do not support designing interventions with a blanket increase in maternal ethnic–racial identity. Rather, our findings suggest that the developmental period of the child should also be considered to ensure optimal child psychosocial outcomes. In addition, future research will be necessary to characterize the degree to which the child’s level of ethnic–racial identity over development—and thus the agreement or discrepancy in mother–child ethnic–racial identity—may influence psychosocial outcomes.
Importantly, the protective nature of maternal ethnic–racial identity was found among U.S. born but not immigrant mothers. This finding is in line with previous research, which has demonstrated that experiences of discrimination and racism are most salient and apparent to U.S.-born minorities (Arellano-Morales et al., 2015; Perez et al., 2008). Here, too, maternal ethnic–racial identity may play a greater role in their children’s well-being because the effects of discrimination associated with ethnic–racial identity are more salient as well. This reinforces the importance of assessing immigrant status in both ethnic–racial identity and psychopathology studies in minority individuals. Moreover, it suggests that interventions that include an ethnic–racial identity component may be most effective for U.S.-born minority groups, and at least U.S.-born Latinx families.
In our secondary analyses, our aim was to explore potential mechanisms through which maternal ethnic–racial identity impacts child’s well-being. This exploration was based on prior findings that child internalizing is related to parenting practices and maternal depression (Beardslee et al., 2011; Goodman et al., 2011; Kingston et al., 2018; Wiggins et al., 2015). Our models suggested that these factors did not significantly mediate effects of maternal ethnic–racial identity on child internalizing at age 3. However, we did not include fine-grained characterization of parent–child interactions surrounding ethnic–racial identity (e.g., conversations about ethnicity between mother and child, ethnic–racial identity transmission from mother to child), which are the most likely mediators of maternal ethnic–racial identity on child internalizing. Future research focusing on such measures may wish to build on our findings to identify mediators.
Limitations
These findings should be interpreted in the light of certain limitations of the study. First, maternal reports were used for both measures, which increases the risk of inflated relationships among variables due to shared method variance. Despite this risk, mother reports of child symptoms may be based on greater time observing the child, as mothers are overwhelmingly the primary caretakers during the toddlerhood to middle childhood period (though mothers do see their child less after the child starts school).
Although the benefit of using this sample was the large sample size from a nation-wide study, the overall nation-wide study only administered an abbreviated scale used to assess ethnic–racial identity, which was derived from the longer version of the MEIM scale. This abbreviated scale has limited reliability due to the reduced number of items (2). The low Cronbach’s α moreover limits the maximum correlation of racial-ethnic identity with other variables in our model and thus makes it harder to detect significant relationships. As such, while we were able to detect the influence of maternal racial-ethnic identity on child internalizing, it is possible that our mediation analyses were not significant due to the limited reliability of our ethnic–racial identity measure. Moreover, this brief measure likely does not capture the complexity and the nuanced variations of ethnic–racial identity for Latinx mothers. For example, although our approach in grouping Latinx/Hispanic participants is in line with prior studies (Gonzales-Backen et al., 2017; Serrano-Villar & Calzada, 2016), culture and racial make-up vary across Latinx/Hispanic countries—and indeed, may even reflect the degree to which U.S.-born participants saw themselves as “American.” (This may be a possible explanation for why early maternal ethnic–racial identity was protective for children, in addition to our explanation that stronger racial-ethnic identity allows one to access more resources from the community.) Indeed, ethnic–racial identity is quite complex and can change over time depending on such factors as developmental stage and one’s experiences (Syed & Azmitia, 2010; Umaña-Taylor et al., 2015). Future research would benefit from a more thorough assessment of the construct over multiple time points, which would allow for exploration of the effects of change of maternal ethnic–racial identity on child internalizing trajectories. In addition, more in-depth assessment of the immigrant experience of mothers (such as English language proficiency, acculturation/assimilation, etc.) would be important to get a more accurate picture of one’s identity. Lastly, it should be noted that these data were collected in late 1990s early 2000s; the political climate in our country surrounding ethnic–racial issues has shifted over time, and current sociopolitical factors can play an important role in shaping one’s identity.
Another limitation is that the ethnic–racial identity of the child was not assessed in this study. Previous studies have examined ethnic–racial identity among preadolescent/adolescent children (Derlan et al., 2017; Serrano-Villar & Calzada, 2016), yet validated measures for ethnic–racial identity in early childhood do not exist. Future work would benefit from a detailed, longitudinal assessment of child and mother ethnic–racial identity to further characterize the influences of this construct within the dyad.
Finally, because maternal education (but not other sociodemographic factors) was related to missingness for child internalizing, it is possible that missing data may have affected our results. As such, we controlled for sociodemographic factors related to missingness and used recommended method for data missing at random (robust even to half of the data missing—we had data from 68% to 73% of participants) (McCartney et al., 2006). Nevertheless, results should be taken tentatively.
Conclusions
Our results suggest that maternal ethnic–racial identity may serve as a protective factor for child internalizing symptoms and thus should be taken into account when designing interventions for diverse populations, particularly children of Latinx mothers born in the U.S. Moreover, the role of maternal ethnic–racial identity as a protective factor seems to be strongest when children are very young (preschool age), as the benefits of having a mother with strong ethnic–racial identity are attenuated as the child grows into school age (9 years), when maternal influence may be lessened. Thus, as our results indicate that child internalizing is sensitive to the developmental timing of maternal ethnic–racial identity, early interventions that capitalize on strengthening maternal ethnic–racial identity when children are in preschool age are likely to have the greatest impact.
Footnotes
Acknowledgments
The authors would like to thank the Eunice Kennedy Shriver National Institute of Child Health and Human Development as well as a consortium of private foundations for their support of the Fragile Families and Child Well-Being Study. They gratefully acknowledge research assistants Jacob Biglow and Yonca Cam, both of San Diego State University, in helping to prepare this manuscript, and Marcela Raffaelli, PhD, of University of Illinois, for feedback on a draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development through grants R01HD36916, R01HD39135, and R01HD40421, as well as a consortium of private foundations for their support of the Fragile Families and Child Well-Being Study.