
Abstract
Experimental and clinical studies have demonstrated an association between posttraumatic stress symptoms (PTSS) and anger. Expanding upon past research, the current study examined the interactive associations among PTSS, distress tolerance (DT), and anger responding among a sample of 95 trauma-exposed adults. This study used a personalized script-driven imagery procedure to gauge emotional responses. Results from a hierarchical linear regression demonstrated a main effect of PTSS and an interaction between PTSS and DT. Simple slope analyses indicated that PTSS level was unrelated to anger responding among traumatic event-exposed people relatively low in DT, while anger responses were positively correlated with levels of PTSS among those relatively higher in DT. These findings highlight the need for future research to consider DT as well as other emotional vulnerability factors in assessing posttraumatic stress disorder-related anger.
A breadth of research has demonstrated a strong relation between anger and posttraumatic stress disorder (PTSD; Orth & Wieland, 2006). Indeed, anger has been shown to be a key characteristic and treatment challenge among individuals with PTSD (Cahill, Rauch, Hembree, & Foa, 2003; Olatunji, Ciesielski, & Tolin, 2010). While anger is a symptom of PTSD, work has shown that anger is also independent from, but related to, symptoms of posttraumatic stress (Forbes, Creamer, Hawthorne, Allen, & McHugh, 2003). Trauma-related anger has been shown to contribute to significant interpersonal difficulties, substance abuse, and physical health problems among traumatic event-exposed individuals with and without PTSD (Demoja & Spielberger, 1997; Helmers, Posluszny, & Krants, 1994; Jakupcak & Tull, 2005).
Controlled laboratory-based and clinical research has converged to demonstrate that posttraumatic stress symptoms (PTSS) are associated with anger responding (McHugh, Forbes, Bates, Hopwood, & Creamer, 2012; Olatunji et al., 2010). Generally, laboratory-based work and neuroimaging studies have established an association between PTSS and emotional reactivity to trauma-relevant cues (e.g. Etkin & Wager, 2007; Shin et al., 1999; Wolf, Miller, & McKinney, 2009). Recent research using script-driven imagery illustrates this association specifically between PTSS and subjective anger responding (Badour et al., 2011). This work is further supported by longitudinal research of trauma-exposed individuals, which examined anger and PTSS in two data sets of crime victims (N = 282; N = and 218) at various time points. Study 1 was based on four assessments in the first 3 months postassault, while Study 2 examined time points at 5 and 7 months postassault. This research found that PTSS predicts state levels of anger (Orth, Cahill, Foa, & Maercker, 2008). Taken together, the association between PTSS and anger has been established. However, less research has examined factors that may affect the nature of this relation. Considering the substantial negative impact of anger on PTSD treatment efficacy, understanding such factors will help fill a critical gap in the research and inform the optimization of interventions for PTSD (Forbes et al., 2008).
Distress tolerance (DT), defined as the capacity to withstand exposure to aversive emotional or physical states, is a common factor shown to influence affect regulation and appraisal (Simons & Gaher, 2005). Further, DT has been identified as a factor associated with PTSS and emotional reactivity to traumatic event cues. Specifically, low DT was associated with elevated levels of negative affect intensity and greater PTSS (Vujanovic et al., 2013). Thus far, PTSS research has focused primarily on anxiety, physiological arousal, and general negative affect propensity with relatively less work examining this association among specific non-fear-based emotions. However, increased anger and low DT are also found in individuals with major depressive disorder (MDD), and in one recent study, DT strategies were shown to decrease anger reactivity among individuals with and without MDD (Ellis, Vanderlind, & Beevers, 2013). Taken together, this work indicates a potential role of DT in the relation between PTSS and anger responding. Considering the serious consequences associated with trauma-related anger and its negative impact on treatment outcomes, anger is an important treatment target for trauma-exposed individuals (Cahill et al., 2003; Helmers et al., 1994; Jakupcak & Tull, 2005). Therefore, a better understanding of the correlates of trauma-related anger has the potential to inform treatment planning such that people at high risk of reacting to traumatic event cues with anger can be offered anger-focused treatment components. Doing so may help improve treatment outcomes. More specifically, investigating the role of DT may help determine how best to target treatments for individuals with varying levels of DT and PTSS and direct further research in this area.
Expanding upon past research, the current study sought to examine the unique and interactive associations among PTSS, DT, and anger responding to traumatic event cues using an individualized script-driven imagery procedure among a community sample of trauma-exposed adults. We hypothesized that the combination of relatively elevated PTSS and low levels of DT would be associated with the greatest anger response to traumatic event cues as compared to those with lower PTSS and high levels of DT. As an attempt at replication and expansion of previous work, we also examined the relation between PTSS, DT, and anxiety responding. Additionally, we included exploratory specificity analyses for other non-fear-based emotions (i.e., sadness, disgust).
Method
Participants
Participants for the current study were drawn from two experimental psychopathology studies that sought to understand the relation between health behaviors, emotional reactivity, and traumatic event exposure. Participants for both studies were recruited through announcements and postings throughout a mid-sized community in the South Central U.S. Eligibility of interested individuals was determined through an initial phone screening and subsequent on-site evaluation. Of particular relevance to the current analysis, both studies included completion of an individualized script-driven imagery procedure (described in greater detail below).
The sample drawn from the first of these two studies was comprised of 45 traumatic event-exposed adults (M age = 27.36, standard deviation [SD age] = 22.92; 51.1% female). Individuals were included who were at least 18-years-old and had been exposed to a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR)-defined Criterion A traumatic event (American Psychiatric Association [APA], 2000). Individuals were excluded for the following: (1) current or lifetime PTSD, (2) current axis I psychopathology, (3) current use of psychotropic medications, (4) history of sleep disorders, (5) limited mental capacity and inability to provide written informed consent, and (6) suicidality.
The sample drawn from the second study included 77 traumatic event-exposed women (M age = 30.29, SD age = 13.78) who had experienced either a physical or a sexual assault; 20.8% of the sample met diagnostic criteria for PTSD (Badour et al., 2011). Individuals were included who were at least 18 years of age and had exposure to a DSM-IV-TR-defined Criterion A traumatic event (APA, 2000) involving sexual or nonsexual assault. Individuals were excluded for the following reasons: (1) limited mental capacity and inability to provide written informed consent, (2) separate instances of both sexual and nonsexual assault, (3) a non-assault-related traumatic experience was the most distressing traumatic event they had experienced, and (4) experience of any traumatic event within the 30 days prior to participation in the study in order to rule out acute stress disorder, allowing for determination of probable PTSD.
The combined sample consisted of 122 adults with self-reported history of traumatic event exposure. Of the total combined sample (N = 122), data for all relevant variables were gathered from 95 participants (Mage = 27.67, SD = 18.41). This subsample (n = 95) was used for all analyses. Overall, 14.7% (n = 14) met diagnostic criteria for PTSD based on the 1–2 scoring rule on the Clinician-Administered PTSD Scale (CAPS; Weathers, Ruscio, & Keane, 1999). Index trauma type distribution across the sample was as follows: 34.7% nonsexual assault, 31.6% sexual assault, 16.8% accident, 3.2% disaster, 3.2% underage sexual contact, 2.1% combat, and 8.4% other. The racial composition of the sample was as follows: 80.0% Caucasian, 7.4% African American, 4.2% Asian, 3.2% American Indian/Alaska Native, 3.2% multiracial, and 2.1% other; 9.5% identified as Hispanic. In terms of education, 93.7% of the sample completed at least part of college.
Measures
PTSS
The CAPS for DSM-IV (Blake et al., 1995) is a well-established semi-structured clinical interview that is used to determine the presence of traumatic event exposure, characteristics of the traumatic event, and frequency and severity of PTSSs. The CAPS has excellent psychometric properties including convergent and discriminant validity, test–retest and inter-rater reliability, and internal consistency. It is therefore considered one of the gold standards in posttraumatic stress assessment (Weathers, Keane, & Davidson, 2001). For the purposes of the current study, a PTSS score was computed by summing the frequency and intensity scores obtained for the 17 DSM-IV-TR-defined symptoms of PTSD (APA, 2000) on the CAPS. Inter-rater reliability was assessed among a random selection of 30% of the interviews, with the second rater blinded to the first rater’s scores. Inter-rater reliability was 100% for PTSD diagnostic status.
DT
The Distress Tolerance Scale (DTS; Simons & Gaher, 2005) is a 15-item questionnaire that examines the degree to which individuals are able to withstand negative psychological states. More specifically, the DTS measures perceived ability to tolerate emotional distress, subjective appraisal of distress, attention being absorbed by negative emotions, and regulation efforts to alleviate distress. Items are rated on a scale ranging from 1 (strongly agree) to 5 (strongly disagree), with lower scores indicating a tendency to experience psychological distress as intolerable. This measure exhibits good internal consistency as well as convergent and discriminant validity (Simons & Gaher, 2005). The DTS showed good internal consistency in the current sample (α = .89).
Vividness and state levels of emotion
A visual analog scale (VAS) was used to measure self-reported vividness of script-driven images as well as state levels of anger, anxiety, sadness, and disgust. Ratings were made on a VAS that ranged from 0 (no anger/anxiety/sadness/disgust/vividness) to 100 (extreme anger/anxiety/sadness/disgust/vividness). Vividness was assessed as a manipulation check.
Procedures
All procedures were approved by the local Institutional Review Board. Participants were informed of risks, and written informed consent was obtained. The CAPS interview, DTS, and other questionnaires not relevant to the current study were then administered. Laboratory procedures were conducted in an experimental room, with the researcher located in an adjacent room. The researcher was able to communicate with the participant via bidirectional intercom.
Script development
Participants were seated in a private, quiet room and asked to generate two personalized scripts based on autobiographical experiences with the assistance of the experimenter. The scripts included one emotionally neutral experience as well as one traumatic experience identified during the CAPS. Specific script development procedures followed those described in previous work (e.g., Lang, Levin, Miller, & Kozak, 1983; Pitman, Orr, Forgue, de Jong, & Claiborn, 1987). The experimenter then left the room to create an audio recording of the scripts, while the participants were asked to complete questionnaires including demographic information, the DTS, and other questionnaires not relevant to the current project.
Script-driven imagery procedure
All participants were presented with their personalized neutral script first, followed by the traumatic event script. The script-driven imagery procedure included a 30-s quiet baseline period in which participants were asked to close their eyes and prepare for the script presentation, followed by a 30-s script presentation and a 30-s imaginal rehearsal period during which participants were asked to continue imagining the scene depicted in the script as vividly as possible. Participants were then given a 30-s recovery period and a 2-min postscript assessment period that included completing VAS ratings. Upon completion of the script presentation, individuals completed additional tasks not relevant to the current study. Participants were compensated and thanked for their time.
Data analytic approach
Initially, zero-order correlations were conducted across all continuous variables (see Table 1). To test our primary interaction hypothesis, a hierarchical linear regression was conducted using SPSS version 22. This regression model controlled for anger responding to a neutral script and measured the main effects of PTSS and DT on anger responding as well as the interaction term. In Step 1, anger responding to a neutral script was entered as a covariate to control for differences in anger level prior to the traumatic event script-driven imagery procedure. In Step 2, main effects for PTSS and DT were entered simultaneously, with the interaction of PTSS and DT entered at Step 3. The hierarchical linear regression was followed by simple slope analyses to determine the direction of the interaction term (PTSS × DT). A series of additional hierarchical regressions were conducted in the same manner to assess the main and interactive effects of PTSS and DT on other emotional reactions (i.e., anxiety, disgust, and sadness).
Descriptive data and zero-order correlations among continuous variables.
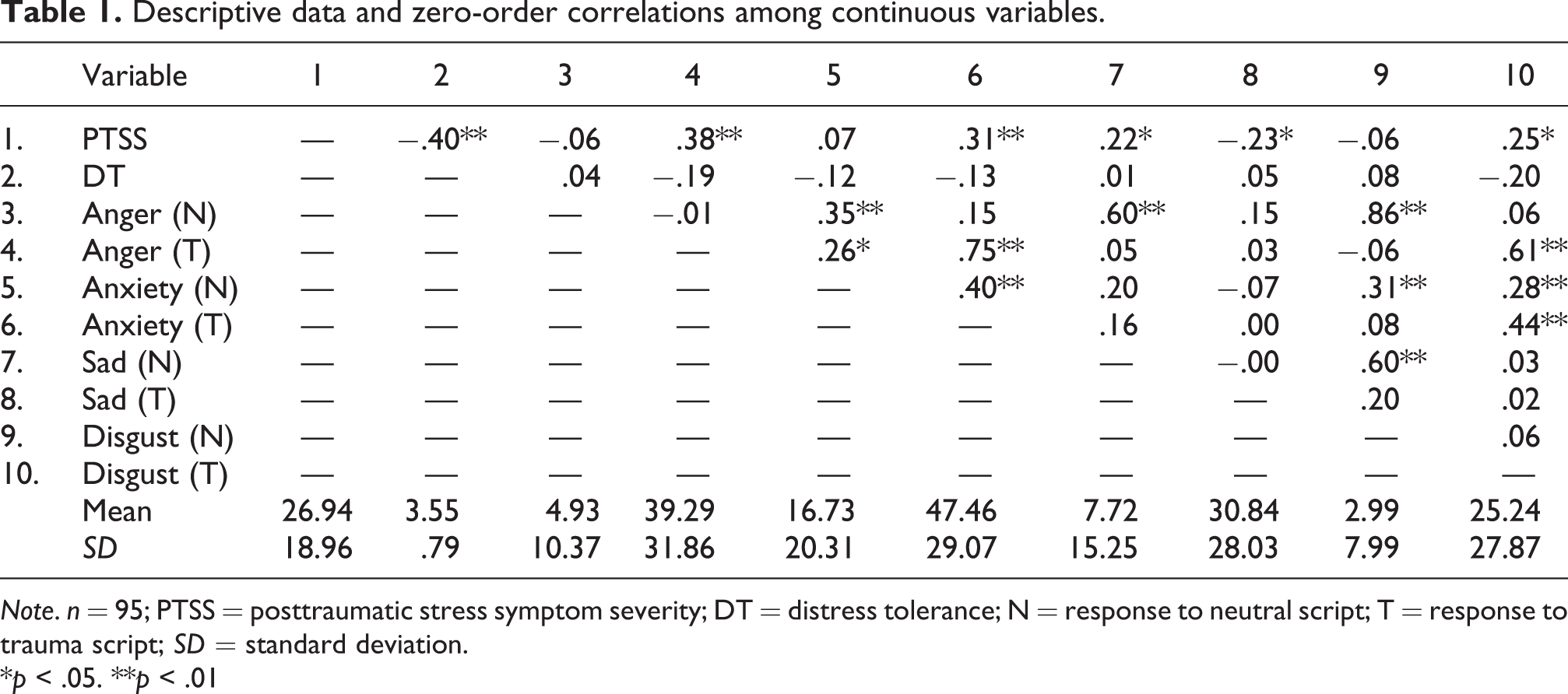
Note. n = 95; PTSS = posttraumatic stress symptom severity; DT = distress tolerance; N = response to neutral script; T = response to trauma script; SD = standard deviation.
*p < .05. **p < .01
Results
Descriptive data
First, correlations among all continuous variables were examined (see Table 1). Correlations demonstrated that PTSS was positively associated with anger, anxiety, and disgust but negatively associated with sadness in response to the trauma script. Associations were also observed between anger, anxiety, and disgust responses to the trauma script. Meanwhile, DT was negatively associated with PTSS but not associated with emotional responses to either the neutral or the traumatic event script. Effect sizes for correlations ranged from moderate to large. Anger, sadness, and disgust responding to a neutral script were not related to anger/sadness/disgust ratings after the traumatic event script. However, anxious response to the neutral script was associated with anxiety ratings after the traumatic event script (r = .40, p < .001).
Manipulation check
Assessments of vividness were obtained immediately following the presentation of the neutral and trauma-relevant script presentation in order to assess the participants’ ability to imagine to script. Overall, results indicated that participants were able to vividly imagine both neutral (M vividness rating = 78.16, SD = 19.95) and trauma scripts (M vividness rating = 83.18, SD = 19.37). Vividness ratings for neutral and trauma scripts were both significantly different from 0, t(94) = 37.57, p < .001; t(94) = 41.41, p < .001, respectively. This level of vividness is consistent with prior work using the script-driven imagery procedure (Olatunji, Babson, Smith, Feldner, & Connolly, 2009).
Additionally, paired-samples t-tests were conducted to compare emotional responses to the neutral and trauma scripts. Anger ratings were significantly higher in response to the trauma script, t(94) = 9.98, p < .001. Anxiety, sadness, and disgust ratings were also significantly higher in response to the trauma script, t(94) = 10.65, p < .001; t(94) = 7.04, p < .001; t(94) = 7.60, p < .001 respectively (see Table 1 for means and SDs).
Primary hypothesis test
A hierarchical linear regression was then conducted to test the primary hypothesis. All continuous predictors were centered prior to entry into the model. At Step 1, F(1, 93) = .00, p = .96, results showed no relation between anger responding to the neutral script and trauma script anger ratings. At Step 2, F(2, 91) = 7.70, p < .001, results demonstrated a positive relation between traumatic event script anger ratings and PTSS (β = .36, p < .001), but not DT (β = −.05, p = .65). At Step 3, F(1, 90) = 5.93, p = .02, an interaction between PTSS and DT was observed (β = .98, p = .02). This model accounted for 19.8% of the variance in traumatic event script anger ratings (see Table 2). Results did not significantly change when neutral script response was removed from the model (see Table 3). In this model, at Step 1, F(2, 92) = 7.76, p < .001, results demonstrated a positive relation between traumatic event script anger ratings and PTSS (β = .36, p < .001), but not DT (β = −.05, p = .65). At Step 2, F(1, 91) = 6.02, p = .02, an interaction between PTSS and DT was observed (β = .98, p = .02).
Results of regression analyses controlling for neutral script response.
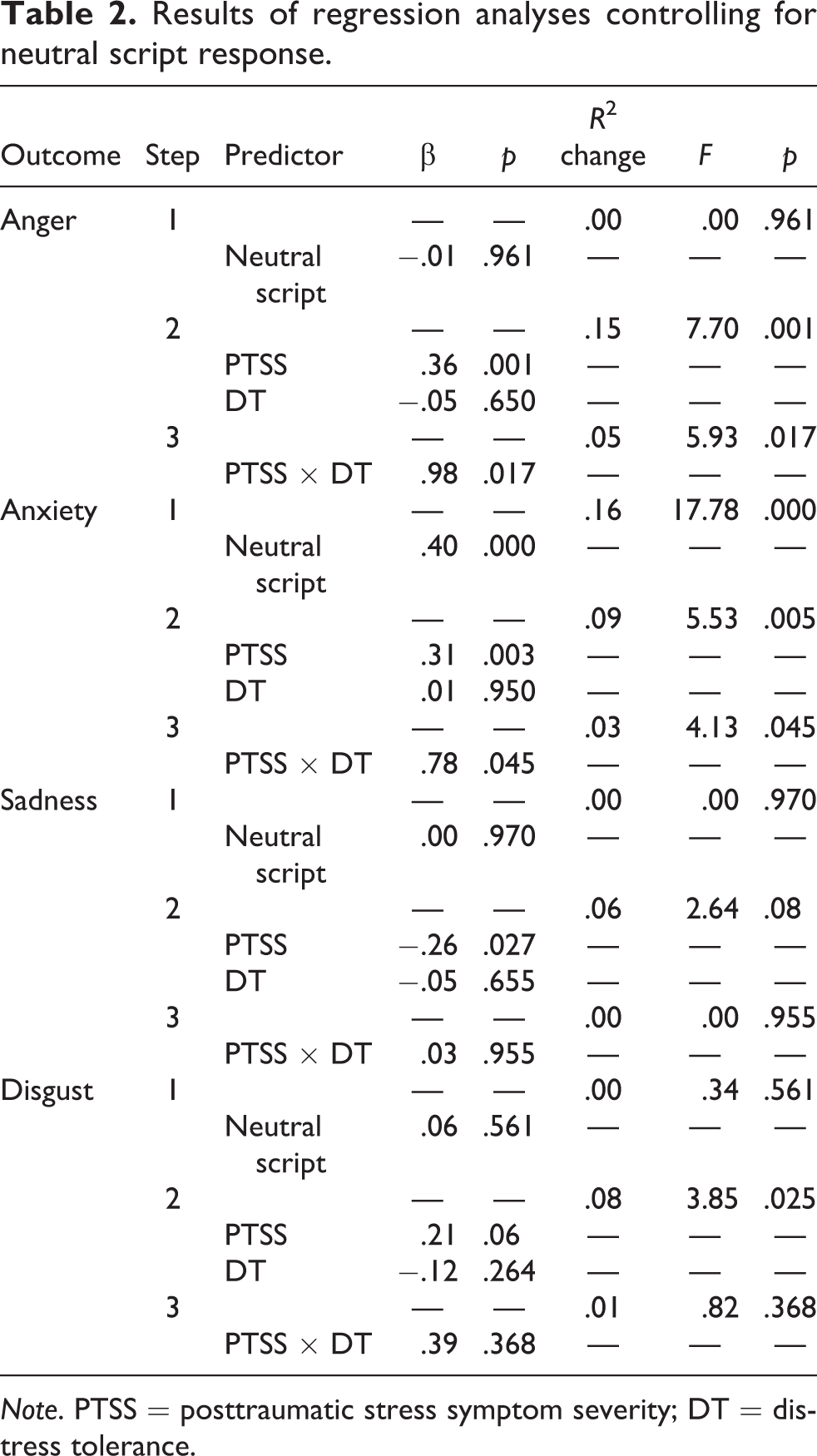
Note. PTSS = posttraumatic stress symptom severity; DT = distress tolerance.
Results of regression analyses without controlling for neutral script response.

Note. PTSS = posttraumatic stress symptom severity; DT = distress tolerance.
To investigate the nature of the interaction term, we conducted simple slope analyses (Aiken, West, & Reno, 1991). High DT (+1 SD) and low DT (−1 SD) were computed, and separate analyses were run among those with high and low DT. Results indicated that the relation between PTSS and anger responding to the trauma script was significant for those relatively higher in DT (β = .67, p < .001) but not for those relatively lower in DT (β = .18, p = .15). Specifically, anger ratings and PTSS positively covaried among people relatively higher, but not lower, in DT (see Figure 1).

Anger responding as a function of posttraumatic stress symptom severity and distress tolerance.
Specificity analysis
Specificity analyses were then conducted to determine whether the observed pattern of results emerges in relation to other emotional reactions (i.e., anxiety, disgust, and sadness). Three additional hierarchical linear regressions were conducted assessing the relations among PTSS, DT, anxiety, disgust, and sadness responses to the trauma script (see Table 2). Similar to the anger-focused regression analysis, the results demonstrated positive associations between PTSS and traumatic event script anxiety ratings (β = .31, p < .001), as well as between PTSS and traumatic event script sadness ratings (β = .20, p = .03), but no main effect of DT. Meanwhile, no main effects were observed for traumatic event script disgust ratings. An interaction of PTSS and DT was observed in the traumatic event script anxiety model (β = .78, p = .05), but not in relation to trauma script sadness or disgust ratings. Simple slope analyses indicated a pattern identical to that of anger, in which the relation between PTSS and anxiety responding to the trauma script was significant for those with relatively higher DT (β = .85, p < .001) but not for those with relatively lower DT (β = .26, p = .15). Finally, these results did not change when neutral script responses were removed from the respective models (see Table 3).
Discussion
The current study sought to expand upon past research by examining the unique and interactive associations of PTSS and DT with anger responding to traumatic event cues. Partially consistent with hypotheses, we found elevated PTSS was associated with greater anger reactions to traumatic event cues. However, counter to hypotheses, the conditional effect of PTSS on anger responding to the traumatic event script was only observed among people relatively higher in DT. Specificity analyses indicated a consistent pattern of findings in terms of anxiety responding, in which PTSS was associated with anxiety reactions to traumatic event cues among individuals with relatively higher DT. Meanwhile, PTSS was not associated with anxiety reactions to traumatic event cues among individuals with relatively low DT. Examination of the simple slope analyses (see Figure 1) suggests that, among individuals relatively higher in DT, PTSS was positively associated with anger and anxiety. Although a main effect was found for PTSS on sadness responding, there were no interactions between PTSS and DT in association with either sadness or disgust responding to the traumatic event script. This indicates that the interactive relations among DT, PTSS, and emotion responding are specific to anger and anxiety.
These findings suggest, in part, that symptoms of posttraumatic stress are associated with anger reactivity to traumatic event cues. This is consistent with previous work showing increased emotional reactivity to trauma cues among individuals high in PTSS (Badour et al., 2011; Etkin & Wager, 2007; Shin et al., 1999; Wolf et al., 2009). The fact that this was true particularly among individuals with relatively high DT is a unique addition to the literature. One possible explanation for this interaction may be that when traumatic event cues are presented in the laboratory they are experienced as relatively uncontrollable. Individuals in a controlled setting may perceive being relatively unable to escape or engage in behaviors that they would typically use to distract themselves from the traumatic event cues, despite the fact the procedure could be discontinued. In other words, experimental demand characteristics likely resulted in the perception that trauma cues were relatively uncontrollable. Individuals with high DT are generally inclined to accept and manage negative emotions. However, as noted above, people with relatively elevated levels of PTSS experience strong emotional reactions to laboratory-presented traumatic event cues. Meanwhile, as evidenced in treatment retention research, people lower in DT may typically rely on escape behaviors for regulating distress they do not believe they can tolerate (Daughters et al., 2005; Tull, Gratz, Coffey, Weiss, & McDermott, 2013). In the laboratory, when the escape option is perceived as relatively inaccessible, the distress experienced (in this case anger and anxiety) is exacerbated among people lower in DT. Therefore, for individuals with relatively low DT, anger and anxiety responses are not associated with PTSS levels. Meanwhile, emotional response to traumatic event cues varies with PTSS among individuals with high DT. This explanation is consistent with research documenting that laboratory-based uncontrollable emotion elicitations elicit stronger emotional reactions than controllable emotion elicitations (Zvolensky, Eifert, Lejuez, & McNeil, 1999). Given this explanation relies on perceived control, which was not measured in the current study, research is now needed to examine this and potentially other mechanisms that may underlie the pattern observed here.
The current findings suggest targeting either PTSS or DT alone may not optimally address anger or anxiety. Indeed, research and clinical work among military veterans with PTSD demonstrates that high levels of anger result from various regulatory deficits within specific domains as well as the activation of “survival mode” functioning which supersedes normal cognitive processing and enhances anger reactions (Chemtob, Novaco, Hamada, Gross, & Smith, 1997; Novaco & Chemtob, 2002). Therefore, additional factors such as emotion regulation deficits and associative memory networks, in which general dysphoria activates anger-related feelings and memories, may need to be targeted in order to reduce anger (Taft, Vogt, Marshall, Panuzio, & Niles, 2007; Tull, Barrett, McMillian, & Roemer, 2007). Future research measuring these factors as possible mechanisms of action in exposure-based treatments would be useful in understanding how emotion regulation and associative memory are associated with DT-related emotional reactivity.
Finally, the demonstration of specificity to anger and anxiety, when combined with previous research, suggests that elevated emotional arousal may be particularly important to consider. For reasons that may resemble the primary results, PTSS is associated with increased anxiety responding only among those with relatively high DT. Indeed, according to the warning signal model of intrusive memories in PTSD, individuals faced with reminders of traumatic events experience elevated physiological arousal in the form of a “fight-or-flight” response, which is central to anger and anxiety-based reactions (Ehlers et al., 2002). The relation between PTSS and comparably negatively valenced emotional reactions (e.g., sadness) that are characteristically lower in arousal did not appear to be associated with DT levels. Taken together, it is possible that DT plays a larger role in the emotional arousal elicited by traumatic event cues than the emotional valence elicited by those cues. Replication of the study described here that adopts a dimensional approach to emotion assessment (e.g., Self-Assessment Manikin; Bradley & Lang, 1994) is needed to directly test this hypothesis.
Although these findings are preliminary, they support initial clinical considerations, such as how to tailor treatments for varying combinations of PTSS and DT. For example, our results would suggest that individuals who are relatively high in DT and endorse elevated PTSS may be more likely to respond to traumatic event cues with anger. This has important treatment implications as research has shown that anger does not habituate like anxiety (McHugh et al., 2012). While several studies have shown some efficacy of exposure and desensitization treatment for anger habituation, anger is generally less responsive to intervention than anxiety in individuals with PTSD (Cahill et al., 2003; Grodnitzky & Tafrate, 2000; O’Donnell & Worell, 1973). Additionally, research shows that state anger may interfere with fear extinction (Foa, Riggs, Massie, & Yarczower, 1995). For this reason, specifically targeting anger responding among those with elevated DT and elevated PTSS may be important. Meanwhile, our results suggest that among individuals relatively lower in DT, anger responses are not associated with PTSS levels. Therefore, regardless of PTSS levels, clinicians may benefit from assessing anger reactivity among people with relatively low DT.
These findings should be considered in the light of the following limitations. First, the sample was comprised of predominantly female, Caucasian, traumatic event-exposed individuals with a small percentage meeting diagnostic criteria for PTSD. Future studies would benefit from replicating this work among a more diverse group of individuals with more severe PTSD. Second, general levels of anxiety, depression, and other sample characteristics were not measured for this study. Future research would benefit from the addition of measures related to general mental health characteristics to better understand the generalizability of the current results as well as have the opportunity to examine these factors as additional variables that may influence the current pattern of results. Third, mean anger and anxiety responses are relatively low, a limitation likely related to the use of a laboratory setting and imagined stimulus. While the script-driven imagery procedure is a strong laboratory analog for measuring emotional reactions to traumatic-event cues (e.g. Pitman et al., 1987), future work would benefit from extending and replicating this work within a clinical setting. Finally, emotion ratings were limited to a single-item response; which limits our understanding of the individual’s cognitions and behavioral reaction tendencies. Future work may benefit from more thoroughly measuring emotional responses, particularly anger, through measures such as the Multidimensional Anger Inventory (Siegel, 1986).
Overall, this was the first study to directly examine the interaction between PTSS and DT on anger responding to traumatic event cues as well as anxiety, sadness, and disgust responding. The interactive effect demonstrates that, among those relatively higher in DT, anger responses are positively correlated with PTSS. The same pattern of results was observed for anxiety, implicating elevated arousal as a potential factor in this relation. Further research is needed to test mechanisms underlying this pattern of results as well as to examine the impact of DT on anger and anxiety in PTSD treatment. In general, future studies should consider DT and other emotional vulnerability factors in assessing PTSD-related anger responding.
Footnotes
Author’s Note
Danielle M. Morabito is also affiliated with Florida State University, USA.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The views expressed here do not necessarily represent those of the National Institutes of Health, Department of Veterans Affairs, or the U.S. government. Dr. Babson is now an employee of Jazz Pharmaceuticals, with stock and/or options in the company. The views expressed in this presentation do not reflect those of Jazz Pharmaceuticals and are solely the authors. Nothing in this presentation represents official Jazz policy or procedures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institute of Mental Health grants F31 MH-081402 (Babson) and F31 MH-092994 (Badour). This work was also supported by a Department of Veterans Affairs Clinical Science Research and Development grant CX001023 (Babson) and by an Office of Research on Women’s Health and National Institute on Drug Abuse Mentored Clinical Scientists Development Award grant K12 DA-035150 (Badour).