
Abstract
Rumination (negative thinking about the past) and worry (anxious apprehension) are two forms of repetitive thinking associated with psychopathology. Prior research indicates that rumination and worry have both distinct and overlapping features, but the extent to which there are separable groups of individuals who engage in rumination, worry, or both has yet to be examined. We used latent profile analysis, a person-centered statistical technique, to examine profiles of repetitive thinkers in two samples (ns = 635 and 755). In both studies, profiles emerged of individuals who rarely ruminate or worry (low repetitive thinkers), individuals who primarily ruminate (ruminators), individuals who primarily worry (worriers), and individuals who frequently ruminate and worry (high repetitive thinkers). In Study 2, a fifth profile of average repetitive thinkers also emerged. Across both samples, high repetitive thinkers showed the highest levels of depression and anxiety symptoms, followed by worriers and ruminators, and then by low repetitive thinkers. In Study 2, the average repetitive thinkers fell below the ruminators and worriers but above the low repetitive thinkers. Thus, there are distinct groups of ruminators and worriers, but individuals who engage in both rumination and worry exhibit the worst outcomes. As such, these findings support adopting a person-centered approach to better understand repetitive thinking styles.
Introduction
Rumination and worry are two forms of repetitive thinking that have received a great deal of attention in the literature (Muris, Roelofs, Meesters, & Boomsma, 2004; Nolen-Hoeksema, Wisco, & Lyobomirsky, 2008; Segerstrom, Tsao, Alden, & Craske, 2000; Watkins, 2008). Rumination entails thinking about one’s distress, and the causes and consequences of that distress, in a passive and repetitive way without moving into active problem-solving (Nolen-Hoeksema et al., 2008). Worry consists of anxious apprehension or uncontrollable thoughts about future threats (Borkovec, 1994). Rumination and worry share a number of critical features: Both are self-focused, passive, repetitive thinking styles that are associated with negative emotions and symptoms of psychopathology (Nolen-Hoeksema et al., 2008; Segerstrom et al., 2000; Siegle, Moore, & Thase, 2004). That said, these two processes differ in terms of their thought content and time orientation (Ehring & Watkins, 2008; McLaughlin, Borkovec, & Sibrava, 2007; Nolen-Hoeksema et al., 2008). The content of ruminative thought frequently consists of themes of self-worth and loss, whereas the content of worry typically centers on themes of possible threat. In addition, rumination is primarily past-oriented and worry is primarily future-oriented (Segerstrom et al., 2000; Watkins, Moulds, and Mackintosh, 2005). Although this distinction is not absolute—it is possible to worry about the implications of past events and ruminate about possible future “consequences” of depressive symptoms (Nolen-Hoeskema et al. 2008; Segerstrom et al., 2000)—within-subjects comparisons have found that rumination is significantly more past-focused than worry, and that worry is significantly more future-focused than rumination (Watkins et al., 2005). The focus on past losses in rumination is consistent with the emotion of sadness and symptoms of depression (Nolen-Hoeksema et al., 2008), whereas the focus on future threat in worry is consistent with the emotion of anxiety and the presence of anxiety disorders, most notably generalized anxiety disorder (GAD; American Psychiatric Association, 2013).
Almost everyone ruminates about their distress or worries about their future occasionally, and infrequent use tends to be well within the range of normal functioning. However, some people tend to engage in these repetitive thinking styles habitually, and it is this habitual use that is thought to lead to functional impairment and longer lasting presentations of depression or anxiety (Watkins & Nolen-Hoeksema, 2014). The tendency to engage in rumination or worry remains relatively stable over time, with measures of both constructs demonstrating high test–retest reliabilities (Meyer, Miller, Metzger, & Borkovec, 1990; Nolen-Hoeksema & Morrow, 1993; Nolen-Hoeksema, Morrow, & Fredrickson, 1993; Stöber, 1998). Therefore, there are individual differences in the tendency to use rumination or worry. What is less clear is whether there are particular types of individuals who tend to ruminate more than they worry, or individuals who tend to worry more than they ruminate. In other words, are there distinct groups of ruminators and worriers? Additionally, it remains unclear whether particular types of individuals engage in both rumination and worry excessively. If rumination and worry reflect a common core process, it could be the case that most ruminators also tend to worry, and most worriers also ruminate much of the time. That is, there may just be two types of people: those who perseverate on the negative and those who do not (Ehring & Watkins, 2008; Watkins, 2008). Some prior research using factor analysis and structural equation modeling suggests that rumination and worry are best modeled as a single, underlying “repetitive thought” latent variable (Segerstrom et al., 2000; Siegle et al., 2004), whereas others indicate that they load onto different factors (Muris et al., 2004). However, these studies have used “variable-centered” approaches to data analysis, such as factor analysis and structural equation modeling, where the goal is to discover associations between variables that are thought to be common across individuals. This approach can be contrasted with “person-centered” analyses that have the goal of identifying subgroups within the population. To our knowledge, no prior studies have used person-centered statistical techniques to examine whether there are distinct groups of ruminators and worriers.
If there are distinct groups of ruminators and worriers, this would allow us to compare these two groups on functional correlates, such as symptoms of psychopathology. An area of great interest has been the extent to which rumination and worry represent specific versus overlapping processes in relation to depression and anxiety symptoms. If rumination and worry are specific risk factors for depression and anxiety respectively, we might expect ruminators to show elevated levels of depression relative to worriers, and for worriers to show elevated levels of anxiety relative to ruminators. We might also expect individuals who both ruminate and worry to show high levels of both depression and anxiety. However, evidence is mounting that rumination and worry are both transdiagnostic risk factors for depression and anxiety (i.e., are associated with increased risk for both depression and anxiety symptoms; McEvoy, Watson, Watkins, & Nathan, 2013; McLaughlin & Nolen-Hoeksema, 2011; Nolen-Hoeksema et al., 2008; Nolen-Hoeksema & Watkins, 2011; Olatunji, Naragon-Gainey, & Wolitzky-Taylor, 2013). Therefore, ruminators and worriers may show similar levels of depression and anxiety to each other, and higher levels of both depression and anxiety relative to individuals who do not tend to engage in repetitive thinking.
The purpose of these studies was to examine distinct styles of repetitive thinking and their association with depression and anxiety symptoms using latent profile analysis (LPA). LPA is a person-centered statistical technique used to identify unobserved subgroups of individuals within a population. Specifically, we were interested in whether separate subgroups of ruminators and worriers would be identified. Given prior findings that rumination and worry have both distinct and overlapping features, we predicted that four latent profiles would emerge: a group who rarely ruminate or worry (low repetitive thinkers), a group who primarily ruminate (ruminators), a group who primarily worry (worriers), and a group who both ruminate and worry (high repetitive thinkers). We also planned to examine group differences in symptoms of depression and anxiety among the subgroups of individuals who demonstrated different repetitive thinking profiles. We predicted that high repetitive thinkers would show the highest symptom levels, followed by the ruminators and worriers, and then by the low repetitive thinkers. Further, we predicted that ruminators would show higher levels of depression relative to worriers, and that worriers would show higher levels of anxiety relative to ruminators.
To achieve these aims, we examined the latent profile structure of repetitive thinking styles in two large data sets. The first data set (Study 1) was constructed from survey data collected by the authors as part of other studies that included the variables of interest. The second data set (Study 2) was collected to provide an independent replication of the observed latent profile structure and its association with depression and anxiety symptoms in a separate sample and to provide additional measures of depression and anxiety more closely linked to clinical outcomes.
Study 1
The purpose of Study 1 was to examine the latent profile structure of repetitive thinking and the association of the latent profiles with depression and anxiety symptoms.
Method
Participants and procedure
Participants (N = 635) were recruited from psychology research pools at two large universities (n = 447, 70.4%), from flyers posted on a university campus (n = 77, 12.1%), and using Amazon’s Mechanical Turk (mTurk; n = 111, 17.5%). Other analyses of the mTurk data set, not related to the aims of the current project, have been published elsewhere (Aldao & Nolen-Hoeksema, 2012, 2013). Amazon’s mTurk is an Internet-based platform that allows researchers to post Human Intelligence Tasks, such as survey completion, in exchange for monetary compensation. Prior work has shown that mTurk can be used to obtain high-quality data that are at least as reliable as those data obtained via traditional methods (Buhrmester, Kwang, & Gosling, 2011). Further, mTurk participants perform similarly on cognitive tasks to participants who are recruited off-line (Paolacci, Chandler, & Ipeirotis, 2010). For the purposes of this survey, we limited the mTurk participant pool to those individuals aged 18 or older located in the U.S. Participants completed these questionnaires either as part of a 1-hr laboratory-based study focused on emotion and motivation (n = 258) or online as part of larger batteries of measures not relevant to the current study (n = 377) and were compensated with course credit or US $7 for their participation. An additional 34 participants consented to participate and completed the surveys but were excluded from this data set because they either failed to complete any of the items assessing the use of rumination or worry (n = 26) or completed the mTurk survey but made a high proportion of mistakes or reported not understanding the instructions (n = 8).
All participants in the final sample provided informed consent and completed the primary study measures assessing rumination, worry, depression symptoms, and anxiety. The final sample (N = 635) included 402 (63.3%) female and 232 (36.5%) male participants (1 participant selected “other”). Participants self-identified their race/ethnicity as 437 (68.8%) Caucasian, 117 (18.4%) African American, 61 (9.6%) Asian American, 35 (5.5%) Hispanic or Latino, 17 (2.7%) Native American, 1 (0.2%) Native Hawaiian or Pacific Islander, and 23 (3.6%) “Other.” 1 Participants’ ages ranged from 18 to 66, with a mean age of 22.49 (SD = 8.80). Participants recruited from Amazon MTurk and university campuses were similar in terms of gender. Participants recruited from university campuses were significantly younger (M = 19.6, SD = 2.9) and more racially diverse (61% White) than participants recruited from Amazon MTurk (mean age = 36.1, SD = 13.3, 73% White), age: t(629) = 25.7, p < .001 (age data were missing for four participants), race/ethnicity: χ2(6, N = 634) = 16.23, p = .01.
Measures
Penn State Worry Questionnaire-3
The Penn State Worry Questionnaire-3 (PSWQ-3) is a 3-item measure of worry that was developed from the original, 16-item PSWQ (Meyer et al., 1990). This shorter measure was developed to avoid problems with reverse-scored items on the longer PSWQ and to enhance clinical utility with an ultra-brief format (Berle et al., 2011). The PSWQ-3 consists of 3 items identified as representative of the fundamental features of worry (“Once I start worrying, I cannot stop,” “I worry all the time,” and “Many situations make me worry.”). The PSWQ-3 has been shown to have similar psychometric properties to the standard PSWQ (Berle et al., 2011; Kertz, Lee, & Björgvinsson, 2014). Items are summed to give the total score, which has a possible range of 3 to 15, with higher scores indicating more worry. In this study, observed PSWQ-3 scores ranged from 3 to 15, with a mean of 7.81 and standard deviation of 3.52, and internal consistency was excellent, α = .89.
Ruminative Responses Scale-Brooding
The Ruminative Responses Scale-Brooding (RRS-B) is a measure of rumination that contains the 5-item brooding subscale of the RRS, a commonly used measure of depressive rumination (Treynor, Gonzalez, & Nolen-Hoeksema, 2003). The RRS-B was developed to reduce the high content overlap between items on the full RRS and self-report measures of depression symptoms, while still measuring the core components of rumination (sample item from RRS-B: “What am I doing to deserve this?”). Consistent with the conceptualization of rumination as a response to depressed mood, the RRS and RRS-B instruct participants to report on their thinking when they feel “down, sad, or depressed.” Items are summed and divided by five (the total number of items) to give the total score, with a possible range of 1 to 4; higher scores indicate more brooding. The RRS-B has shown good psychometric properties in prior research (Treynor et al., 2003), and internal consistency in this study was excellent, α = .81. In this study, scores ranged from 1 to 4, with a mean of 2.26 and standard deviation of 0.69.
Mood and Anxiety Symptom Questionnaire
The Mood and Anxiety Symptom Questionnaire (MASQ) includes 62 items assessing anxiety and depression symptoms (Watson et al., 1995a, 1995b). This study included the 17-item anxious arousal and 22-item anhedonic depression MASQ subscales, which assess nonoverlapping symptoms of anxiety and depression. After reverse-scoring of negatively worded items, items are summed to give total scores, with possible scores of 17 to 85 for the anxious arousal scale and 22 to 110 for the anhedonic depression scale; higher scores indicate more severe symptoms on both scales. Unlike more general measures of depression and anxiety, which frequently share similar items assessing symptoms such as concentration difficulties, irritability, and sleep disturbance, the anxious arousal and anhedonic depression scales are ideal for research questions which seek to eliminate conceptual and measurement overlap between anxiety and depression (Watson et al., 1995a, 1995b). The anxious arousal subscale measures somatic symptoms of anxiety (sample item: “Startled easily”) whereas the anhedonic depression subscale measures low positive affect and lack of interest (sample item: “Felt like nothing was enjoyable”). The MASQ has been shown to have excellent psychometric properties (Watson et al., 1995a, 1995b). Consistent with prior research (Aldao, Nolen-Hoeksema, & Schweizer, 2010), the anxious arousal and anhedonic depression scales demonstrated excellent internal consistencies (αs >.89) and were only moderately correlated with each other in this study, r = .27, p < .001. Total scores ranged from 17 to 72 (M = 28.09, SD = 9.70) for the anxious arousal scale and 23 to 103 (M = 53.82, SD = 14.58) for the anhedonic depression scale.
Data analysis plan
All data were analyzed with MPlus Version 7.11 (Muthén & Muthén, 1998–2012). We utilized the three-step analysis approach to latent variable modeling (Asparouhov & Muthén, 2013). This approach allows investigators to use the indicator variables to create latent classes and then use the constructed profiles to predict distal outcomes (Asparouhov & Muthén, 2013; Bolck, Croon, & Hagenaars, 2004; Feingold, Tiberio, & Capaldi, 2014; Vermunt, 2010). In the first step, the LPA is conducted and the optimal number of profiles is identified. We planned an LPA of the eight repetitive thinking questions (three PSWQ-3 and five RRS-B items, all standardized prior to analysis for ease of interpretation). To examine how many latent profiles provided the best fit to the data, we used standard fit indices (Bayesian and Sample-Size Adjusted Bayesian Information Criteria [BIC and ABIC] and Lo–Mendell–Rubin adjusted likelihood ratio test [LRT]). These fit indices are used to compare models with different numbers of profiles; lower BIC and ABIC values indicate better fit, and significant LRT tests (p < .05) indicate that n profiles provide a better fit than n − 1 profiles. In the second step, the most likely profile memberships are obtained along with the classification uncertainty. In other words, individuals are assigned to the profile that best fits their responses, yet the uncertainty with which that individual fits the assigned profile is also modeled. In the third step, the most likely profile membership variables are analyzed as predictors of the distal outcome variables, taking into account the classification uncertainty. Chi-square tests are provided which test whether profiles differ significantly from each other on each distal outcome of interest. We planned two separate models for distal outcome variables: one predicting anhedonic depression symptoms and one predicting anxious arousal symptoms.
Results
Latent profile analysis
Table 1 shows fit indices for two-, three-, four-, and five-profile solutions. The Lo–Mendell–Rubin adjusted LRT indicated that a four-profile solution provided a significantly better fit than a three-profile solution; five profiles did not significantly improve fit over four profiles (see Table 1). In contrast, the BIC and ABIC indices indicated that the five-profile solution provided a better fit than the four-profile solution (see Table 1). 2 However, examination of the five-profile solution revealed that it did not provide good class discrimination because it included a low-frequency (7.8%) profile that differed from another profile only in severity, not in type. Therefore, we retained the four-profile solution, which provided good entropy (0.84) and good classification probabilities for most likely latent class membership (ranging from 0.85 to 0.96).
LPA of worry and rumination items in Study 1: Fit indices for 2- to 5-profile solutions.

Note. For BIC and ABIC indices, lower numbers indicate better fit. Significant values (p < .05) on the LRT test indicate that n profiles provide a better fit than n − 1 profiles. LPA = latent profile analysis; BIC = Bayesian Information Criteria; ABIC = Sample-Size Adjusted Bayesian Information Criteria.
Figure 1 provides the sample item means for the four-profile solution. Participants were classified into one of the following: (1) low levels of both rumination and worry (low repetitive thinkers, n = 223, 35.12%), (2) high levels of rumination but low levels of worry (ruminators, n = 166, 26.14%), (3) high levels of worry but low levels of rumination (worriers, n = 135, 21.26%), or (4) high levels of both worry and rumination (high repetitive thinkers, n = 111, 17.48%). Classification probabilities were high across the four profiles, with probabilities of .95 in the low repetitive thinkers, .85 in the ruminators, .89 in the worriers, and .96 in the high repetitive thinkers.

Sample item means for the four latent profiles in Study 1. PSWQ = Penn State Worry Questionnaire; RRSB = Ruminative Response Scale, Brooding subscale.
Associations with depression and anxiety symptoms
We then examined possible differences between the four profiles on anhedonic depression and anxious arousal symptoms, using the three-step analysis approach described above (see Figure 2). When predicting anhedonic depression symptoms, the high repetitive thinkers showed higher symptom levels than any of the other three groups, χ2s > 52, ps < .001. Worriers and ruminators both showed higher anhedonic depression symptoms than low repetitive thinkers, χ2s > 29, ps < .001, but did not differ from each other on anhedonic depression symptoms, χ2(1, N = 635) = 0.37, p = .54. When predicting anxious arousal, a slightly different pattern emerged. High repetitive thinkers and worriers both reported higher anxious arousal than ruminators or low repetitive thinkers, χ2s > 18, ps < .001, but did not differ from each other, χ2(1, N = 635) = 1.11, p = .29. Ruminators showed higher anxious arousal than low repetitive thinkers, χ2(1, N = 635) = 16.92, p < .001.
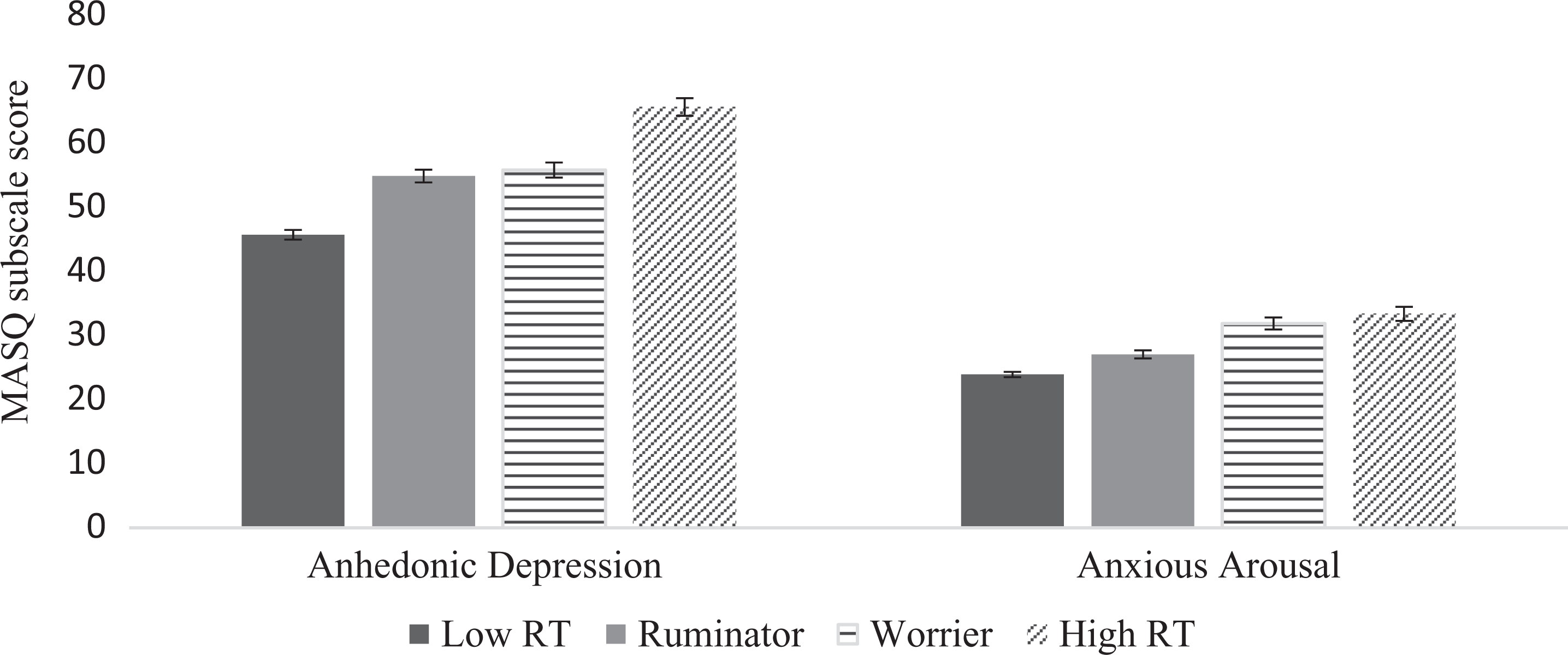
Study 1 latent repetitive thinking profiles as predictors of anhedonic depression and anxious arousal symptoms. MASQ = Mood and Anxiety Symptom Questionnaire; RT = repetitive thinker. Error bars reflect standard errors.
Discussion
In this study, we found evidence supporting the existence of four profiles of repetitive thinking: low repetitive thinkers (i.e., those reporting low rumination and worry), ruminators (i.e., those reporting elevated rumination and low worry), worriers (i.e., those endorsing elevated worry and low rumination), and high repetitive thinkers (i.e., those endorsing elevated rumination and worry). In fact, participants were more likely to be classified into a profile that is characterized by the habitual use of either rumination (26.14%) or worry (21.26%) than a profile characterized by habitual use of both forms of repetitive thinking (17.48%). Thus, rumination and worry might not always be “two sides of the same coin” as some research suggests (Brosschot, Gerin, & Thayer, 2006; McEvoy et al., 2013; Segerstrom et al., 2000; Siegle et al., 2004). Instead, rumination and worry might reflect two distinct processes that different people tend to use to varying degrees. However, our findings also indicate that a subset of participants habitually ruminate and worry.
In order to investigate functional outcomes of each of the four repetitive thinking profiles, we examined associations with symptoms of anhedonic depression and somatic symptoms of anxiety. High repetitive thinkers reported the highest levels of depression symptoms, followed by ruminators and worriers, who endorsed greater levels than the low repetitive thinkers. Contrary to our hypothesis, ruminators and worriers did not differ significantly from each other in self-reported levels of depression. As such, depression symptoms do not appear to be uniquely linked to either rumination or worry. This finding runs counter to our expectation that rumination, with its focus on past losses, would be more strongly associated with depression symptoms than worry, with its future orientation and focus on threats (Nolen-Hoeksema et al., 2008). However, this result is consistent with prior research suggesting that worry is best conceptualized as a transdiagnostic risk factor for both depression and anxiety disorders (e.g., McEvoy et al., 2013). Moreover, engaging in both repetitive thinking styles seemed to have an additive effect, such that the high repetitive thinkers demonstrated higher levels of depression symptoms than either the ruminators or worriers, who did not differ from each other.
High repetitive thinkers and worriers endorsed the highest levels of anxious arousal, followed by the ruminators, who endorsed greater levels than the low repetitive thinkers. Importantly, the worriers endorsed significantly higher levels of anxious arousal than the ruminators. In other words, for those people who tend to use just one type of repetitive thinking, they were more likely to experience anxious arousal if they tended to worry than if they tended to ruminate. Moreover, the high repetitive thinkers and worriers did not significantly differ in levels of anxious arousal. These findings provide insight when delineating the maladaptive effects of rumination and worry. Among individuals who worry much of the time, rumination does not further increase symptoms of anxious arousal. This stands in contrast to anhedonic depression, in which rumination and worry showed an additive effect.
In this study, we found evidence for four types of repetitive thinking profiles, including some individuals who engage primarily in one type of repetitive thought (rumination or worry) but not the other. Individuals who habitually engage in both rumination and worry evidenced the worst outcomes, with higher levels of both anxious arousal and anhedonic depression than any of the other profiles. Consistent with our predictions, worriers reported more anxious arousal than ruminators, but, contrary to our expectations, ruminators did not report more anhedonic depression than worriers. Although these findings are informative, it is important to replicate both the profile structure and the associations with depression and anxiety in an independent sample to establish the replicability and generalizability of these results. Additionally, the results of Study 1 are somewhat limited by our choice of the MASQ scales to measure depression and anxiety. We chose these scales because they better distinguish between the independent features of anxiety and depression by removing symptoms that may artificially inflate associations due to conceptual overlap. However, a limitation of these scales is that they do not have established cutoffs that correspond to clinically significant levels of distress, constraining the potential clinical relevance of our findings. In our second study, we addressed these limitations by collecting data in an independent sample to provide a replication of these findings and added measures of depression and anxiety with established cutoffs.
Study 2
The purpose of Study 2 was to replicate the latent profile structure of repetitive thinking in an independent sample and to examine differences between the profiles in depression and anxiety symptoms. In addition to the MASQ anhedonic depression and anxious arousal scales, we included two complementary measures of depression and anxiety: the Beck Depression Inventory-II (BDI-II) and the GAD-7. Compared to the MASQ-anhedonic depression scale, which specifically measures anhedonia (lack of interest or pleasure), the BDI-II is a more general measure of depression symptoms that covers a wider range of symptoms (e.g., cognitive and physical symptoms of depression). Whereas the MASQ-anxious arousal scale measures somatic symptoms of anxiety, the GAD-7 provides a more specific measure corresponding to the diagnostic criteria for GAD (American Psychiatric Association, 2013). Both the BDI-II and GAD-7 are widely used in clinical settings and have well-established cutoffs that correspond to clinically significant levels of distress, offering benchmarks for interpretation of our results with enhanced clinical utility.
Method
Participants and procedure
Participants in Study 2 (n = 755) were recruited from a psychology research pool at a large university. Participants were required to be 18 years old or older and able to read and write in English. Participants provided informed consent and completed a battery of self-report questionnaires as part of an online survey. An additional 48 participants completed the online survey but were excluded from the final sample used for analyses (n = 755) because they either did not verify that they were age 18 or older or had a significant amount of missing data. The final sample (N = 755) included 561 (74.3%) female and 192 (25.4%) male participants (2 participants did not report their sex). Participants self-identified their race/ethnicity as 352 (46.6%) Caucasian, 228 (30.2%) African American, 56 (7.4%) Asian American/Pacific Islander, 53 (7.0%) Hispanic or Latino, 7 (0.9%) American Indian/Alaskan Native, 35 (4.6%) Biracial, and 23 (3.0%) “Other.” 1 Participants’ ages ranged from 18 to 43, with a mean age of 19.02 (SD = 2.39).
Measures
Similar to Study 1, the PSWQ-3 and RRS-B were again used as the measures of worry and rumination, respectively. The MASQ anhedonic depression and anxious arousal scales were again used to assess nonoverlapping features of depression and anxiety. All of these self-report scales showed excellent internal consistencies in Study 2 (αs ranged from .86 to .93; please see Study 1 methods for descriptions of the psychometric properties of these measures). In Study 2, worry scores ranged from 3 to 15 (M = 8.34, SD = 3.59), brooding scores ranged from 1 to 4 (M = 2.14, SD = 0.77), MASQ anxious arousal scores ranged from 17 to 72 (M = 30.22, SD = 10.36), and MASQ anhedonic depression scores ranged from 22 to 107 (M = 55.35, SD = 14.45).
Beck Depression Inventory-II
The BDI-II is a commonly used 21-item self-report measure of depression symptoms with well-established reliability and validity (Beck, Steer, & Brown, 1996). The items are summed to provide an overall index of depression symptom severity, such that scores of 0–13 indicate minimal, 14–19 mild, 20–28 moderate, and 29 and above severe depression (Beck et al., 1996), with scores of 20 or higher typically used to indicate clinical significance. The BDI-II assesses a range of symptoms including anhedonia, sad mood, and other cognitive (e.g., pessimism) and somatic (e.g., sleep disturbance) depression symptoms (Storch, Roberti, & Roth, 2004). In this study, the BDI-II showed excellent internal consistency (α = .93) and total scores ranged from 0 to 62, with a mean of 11.23 and standard deviation of 10.45.
Generalized anxiety disorder-7
The GAD-7 is a 7-item self-report measure of symptoms of GAD (Spitzer, Kroenke, Williams, & Löwe, 2006). The GAD-7 has demonstrated good reliability and strong convergent validity with clinical interview measures of GAD in prior validation studies (Beard & Björgvinsson, 2014; Spitzer et al., 2006). Items are summed to give total severity scores, and cut-scores of 5, 10, and 15 reflect mild, moderate, and severe anxiety, respectively, with scores greater than or equal to 10 indicating clinical significance. In this study, the GAD-7 demonstrated excellent internal consistency (α = .93) and total scores ranged from 0 to 21, with a mean of 6.22 and standard deviation of 5.34.
Data analysis plan
We first examined the bivariate correlations between the different measures of anxiety and depression symptoms, to assess whether the MASQ-anxious arousal and anhedonic depression scales had less overlap than the BDI-II and GAD-7, as predicted. We then utilized the same three-step analysis approach to latent variable modeling (Asparouhov & Muthén, 2013) used in Study 1, again using MPlus Version 7.11 (Muthén & Muthén, 1998–2012). For the first step, we planned an LPA of the eight repetitive thinking questions (three PSWQ-3 and five RRS-B items, all standardized prior to analysis). To examine how many latent profiles provided the best fit to the data, we again used the BIC and ABIC and Lo–Mendell–Rubin adjusted LRT test. In the second step, we again planned to obtain the most likely profile memberships along with the classification uncertainty. In the third step, we planned to analyze the most likely profile membership variables as predictors of the distal outcome variables taking into account classification uncertainty. We again used χ2 tests to examine whether profiles differed significantly from each other on distal outcomes of interest. We planned separate models for each distal outcome variable (anhedonic depression, general depression, anxious arousal, and generalized anxiety symptoms).
Results
Associations between different measures of anxiety and depression
We first examined the bivariate correlations between the anhedonic depression, anxious arousal, general depression, and generalized anxiety symptom measures, to assess whether the MASQ scales were successful in capturing more distinct aspects of depression and anxiety, relative to the BDI-II and GAD-7. Consistent with prior research (Watson et al., 1995a, 1995b), the correlation between the MASQ anhedonic depression and anxious arousal scales, r = .38, p < .001, was significantly smaller than the correlation between the BDI-II and the GAD-7, r = .68, p < .001, Z = 8.3, p < .001.
Latent profile analysis
Fit indices for two-, three-, four-, five-, and six-profile solutions are provided in Table 2. The Lo–Mendell–Rubin adjusted LRT indicated that a five-profile solution demonstrated a significantly better fit than a four-profile solution, and six profiles did not significantly improve fit over five profiles (see Table 2). In contrast, the BIC and ABIC indices indicated that the six-profile solution provided a better fit than the five-profile solution. We ran additional analyses until the BIC and ABIC values reached a minimum value, which occurred at 9 profiles for BIC and at 13 profiles for the ABIC. In neither case was the LRT significant (9 profiles, LRT = 90, p = .17; 13 profiles, LRT = 45, p =.75), and both solutions provided poorer class discrimination and lower classification probabilities than the five-profile solution. Thus, we retained a five-profile solution.
LPA of worry and rumination indices in Study 2: Fit indices for 2- to 6-profile solutions.

Note. For BIC and ABIC indices, lower numbers indicate better fit. Significant values (p < .05) on the LRT test indicate that n profiles provide a better fit than n − 1 profiles. LPA = latent profile analysis; BIC = Bayesian Information Criteria; ABIC = Sample-Size Adjusted Bayesian Information Criteria.
Sample item means for the five-profile solution are provided in Figure 3. Participants were classified into one of the following: (1) low levels of both rumination and worry (low repetitive thinkers, n = 194, 25.70%), (2) average levels of rumination and worry (average repetitive thinkers, n = 199, 26.36%), (3) high levels of worry but low levels of rumination (worriers, n = 126, 16.69%), (4) high levels of rumination but low levels of worry (ruminators, n = 138, 18.28%), or (5) high levels of both worry and rumination (high repetitive thinkers, n = 98, 12.98%). Classification probabilities were high across the five profiles, with probabilities of .91 in the low repetitive thinkers, .88 in the average repetitive thinkers, .91 in the worriers, .89 in the ruminators, and .92 in the high repetitive thinkers.

Sample item means for the five latent profiles in Study 2. PSWQ = Penn State Worry Questionnaire; RRSB = Ruminative Response Scale, Brooding subscale.
Associations with depression and anxiety symptoms
We then examined possible differences between the five profiles on anhedonic depression, anxious arousal, general depression, and generalized anxiety symptoms, using the three-step analysis approach described above (see Figure 4). When predicting anhedonic depression symptoms, the high repetitive thinkers showed higher symptom levels than any of the other four groups, χ2s > 14, ps < .001. Worriers and ruminators showed the next highest levels of anhedonic depression symptoms. Worriers and ruminators did not differ from each other, χ2(1, N = 755) = 0.90, p = .34, but both reported significantly more anhedonic depression than average repetitive thinkers or low repetitive thinkers, χ2s > 15, ps < .001. Finally, average repetitive thinkers reported more anhedonic depression symptoms than low repetitive thinkers, χ2 = 21.825, p < .001.

Study 2 latent repetitive thinking profiles as predictors of anhedonic depression, general depression, anxious arousal, and GAD symptoms. Anhedonic depression and anxious arousal refer to scores on the respective subscale of the MASQ. General depression reflects total BDI-II score; generalized anxiety reflects total GAD-7 score. Error bars present standard errors. GAD = generalized anxiety disorder; MASQ = Mood and Anxiety Symptom Questionnaire; BDI-II = Beck Depression Inventory-II.
When predicting general depression symptoms (measured by the BDI-II), the same pattern emerged. The high repetitive thinkers again showed significantly higher symptom levels than any of the other four groups, χ2s > 59, ps < .001. Worriers and ruminators again did not differ from one another, χ2(1, N = 755) = 0.661, p = .42, but both showed higher symptom levels than the average repetitive thinkers and the low repetitive thinkers, χ2s > 31, ps < .001. Furthermore, the average repetitive thinkers reported significantly more depressive symptoms than the low repetitive thinkers, χ2(1, N = 755) = 60.89, p < .001. When compared to standard cutoff scores for the BDI-II (Beck et al., 1996), the mean score for the high repetitive thinkers (M = 24.9, SE = 1.2) was above the cutoff for clinical significance and in the “moderate” symptom range; the scores for the other groups were in the “minimal” symptom range (scores <14) (worriers, M = 13.9, SE = 0.8; ruminators, M = 13.1, SE = 0.8; average repetitive thinkers, M = 8.1, SE = 0.5; low repetitive thinkers, M = 3.8, SE = 0.3).
When predicting anxious arousal symptoms, the high repetitive thinkers again showed higher symptom levels than any of the other four groups, χ2s > 20, ps < .001. Worriers and ruminators did not differ from each other on anxious arousal, χ2(1, N = 755) = 2.63, p = .105. Worriers again showed higher anxious arousal symptoms than average repetitive thinkers, χ2(1, N = 755) = 7.09, p = .008, but ruminators did not differ from the average repetitive thinkers, χ2(1, N = 755) = 0.95, p = .33. Worriers, ruminators, and average repetitive thinkers all showed higher anxious arousal symptoms than low repetitive thinkers, χ2s > 60, ps < .001.
When predicting generalized anxiety symptoms (measured by the GAD-7), a slightly different pattern emerged such that all of the profiles significantly differed from each other. Again, the high repetitive thinkers showed significantly higher symptom levels than any of the other four groups, χ2s > 38, ps < .001. The worriers showed higher symptom levels than the other three groups (ruminators, average repetitive thinkers, and low repetitive thinkers), χ2s > 31, ps < .001; the ruminators showed higher symptom levels than the other two groups (average repetitive thinkers and low repetitive thinkers), χ2s > 7, ps < .001; and the average repetitive thinkers showed higher symptoms levels than the low repetitive thinkers, χ2(1, N = 755) = 109.88, p < .001. 3 Using the standard cut-scores of 5, 10, and 15 to reflect mild, moderate, and severe anxiety, respectively (Spitzer et al., 2006), only the high repetitive thinkers reported generalized anxiety symptoms in the moderate range, above the cutoff for clinical significance (M = 13.3, SE = 0.48). The worriers (M = 9.3, SE = 0.4), ruminators (M = 6.2, SE = 0.4), and average repetitive thinkers (M = 5.0, SE = 0.3) all reported generalized anxiety symptoms in the mild range. The low repetitive thinkers’ scores placed them below the cutoff for mild generalized anxiety symptoms (M = 1.8, SE = 0.1).
Discussion
In Study 2, we used LPA to identify profiles of repetitive thinking styles. Five profiles emerged: high repetitive thinkers (i.e., those endorsing high levels of rumination and worry), ruminators (i.e., those endorsing high levels of rumination but low worry), worriers (i.e., those endorsing high levels of worry but low rumination), average repetitive thinkers (i.e., those endorsing average levels of rumination and worry), and low repetitive thinkers (i.e., those endorsing low levels of rumination and worry). Similar to Study 1, we found evidence for a subgroup of individuals who tend to both ruminate and worry (high repetitive thinkers), but also separate groups of individuals who tend primarily to ruminate (ruminators) or primarily to worry (worriers). Rather than finding just one subgroup of low repetitive thinkers, as we found in Study 1, in Study 2 we found that this last group was split into two subgroups (average versus low repetitive thinkers). Overall, these results suggest that rumination and worry may be best conceptualized as distinct repetitive thinking styles rather than one overarching construct, given the identification of people who predominately engaged in one type of repetitive thinking but not the other (e.g., Hong, 2007; Muris et al., 2004).
Importantly, these profiles of repetitive thinking styles were differentially associated with symptoms of depression and anxiety. For both anhedonic depression and general depression, the high repetitive thinkers endorsed the highest levels compared to all other profiles of repetitive thinking styles. These results suggest that habitually engaging in both rumination and worry was linked to the highest levels of depression symptoms, higher than engaging in either form of repetitive negative thinking without the other. Moreover, this group was the only one to report general depression symptoms in the moderate symptom range, above the cutoff used to indicate clinical significance, highlighting the potential clinical relevance of these findings (although we should note that individuals who score above this cutoff do not necessarily meet full diagnostic criteria for major depressive disorder). As previously mentioned, this finding suggests that ruminating and worrying frequently has an additive effect on one’s experience of anhedonia and depression.
We also found that the ruminators and worriers did not significantly differ from each other in their levels of anhedonic depression or general depression, contrary to our prediction that depression would be higher among ruminators than worriers. One interpretation of this finding may be that rumination and worry do share common features, or perhaps even a common mechanism, which contributes to the experience of anhedonia and depression. Overall, this is consistent with extant literature demonstrating that both rumination and worry have similar associations to depressive symptoms, which may highlight the transdiagnostic nature of repetitive negative thinking (e.g., Fresco, Frankel, Mennin, Turk, & Heimberg, 2002; Roelofs, Huibers, Peeters, Arntz, & van Os, 2008; Segerstrom et al., 2000).
When examining associations with anxious arousal, the high repetitive thinkers endorsed significantly higher levels than the worriers, ruminators, average repetitive thinkers, or low repetitive thinkers. The worriers had the second highest levels of anxious arousal, but did not significantly differ from the ruminators, in contrast to our findings from Study 1. Worriers also had significantly higher levels of anxious arousal than the average or low repetitive thinkers, and ruminators had significantly more anxious arousal than the low repetitive thinkers. Taken together, these results suggest that engaging in high levels of both rumination and worry is associated with the greatest physiological arousal and somatic symptoms of anxiety (e.g., racing heart, shortness of breath, trembling or shaking). Overall, this provides further support for the synergistic effect of engaging in both of these repetitive thinking styles frequently and the detrimental outcomes associated with doing so.
When examining associations with symptoms of generalized anxiety using the GAD-7, the high repetitive thinkers endorsed the greatest levels, followed by the worriers, then the ruminators, then the average repetitive thinkers, and finally the low repetitive thinkers. Similar to the findings discussed above, engaging in high levels of both rumination and worry was associated with the greatest symptoms of generalized anxiety (e.g., difficulties controlling worries, feeling restless and on edge). Following the high repetitive thinkers, the worriers demonstrated the second highest symptom levels of generalized anxiety, which was significantly greater than all other profiles of repetitive thinking. Unlike the other measures of depression and anxiety, worriers reported significantly higher levels of generalized anxiety symptoms than ruminators, and this result could not be explained by shared item content across the GAD-7 and PSWQ-3. 3 This finding suggests that generalized anxiety symptoms, specifically, are more closely linked to worry than to rumination, consistent with the inclusion of worry as a key symptom in the diagnostic criteria for GAD (American Psychiatric Association, 2013). In terms of clinical significance, the high repetitive thinkers were the only group who reported generalized anxiety symptoms in the clinical range (a score ≥ 10), although we should note that these scores indicate high levels of anxiety symptoms, not a GAD diagnosis. In contrast, worriers, ruminators, and average repetitive thinkers all reporting generalized anxiety symptoms at different points within the mild range.
Overall discussion
In latent profile analyses of repetitive thinking styles in two independent samples, we obtained similar, but not identical, profile structures. Both studies found profiles of individuals who frequently ruminate and worry (high repetitive thinkers), individuals who primarily worry (worriers), individuals who primarily ruminate (ruminators), and individuals who rarely ruminate or worry (low repetitive thinkers). In Study 2, a fifth profile of “average repetitive thinkers” also emerged; this group reported slightly higher levels of rumination and worry than the low repetitive thinkers. Consistent with predictions, both studies identified subgroups of individuals who engage in both rumination and worry (high repetitive thinkers), as well as individuals who primarily use just one type of repetitive thinking or the other, but not both (ruminators and worriers). These profile structures support the study of ruminators and worriers as separate groups of people in future research, as some individuals habitually engage in just one type of repetitive thought without using the other.
Despite partial replication of our findings across two independent samples, it is important to note that some differences emerged between the two studies. The two studies differed in the total number of profiles identified (four versus five); four of the profiles were remarkably similar across the two samples, but in Study 2 a fifth profile of average repetitive thinkers emerged. The average repetitive thinkers reported levels of worry and rumination between 0 and 0.5 SDs below the mean on all items, compared to the low repetitive thinkers, who reported levels of worry and rumination from 0.5 to 1 SDs below the mean. The average repetitive thinkers appear to differ from the low repetitive thinkers primarily in degree, rather than kind. But future research using larger representative samples would be needed to determine whether four or five profiles of repetitive negative thinking best represent patterns of thinking styles in the population.
We found only partial support for our hypothesis that worriers would be uniquely characterized by anxiety symptoms, and no support for our hypothesis that ruminators would be uniquely characterized by depression symptoms. In Study 1, we found that worriers reported higher levels of anxious arousal than ruminators, but this result was not replicated in Study 2. In Study 2, we did find evidence that worriers reported higher levels of generalized anxiety symptoms than ruminators, and this result held even after removing potential measurement artifact (by removing two “worry” items on the GAD-7). Although the worriers reported statistically significantly higher generalized anxiety symptoms than the ruminators, both groups reported symptom levels in the “mild” range, calling into question the clinical significance of this difference between the two groups. In terms of depression, we found no evidence that ruminators reported significantly more depression than worriers, with no significant differences between the groups on depression symptoms in either study. Taken together, these findings suggest that there are separable groups of ruminators and worriers, indicating that rumination and worry are not identical constructs. However, we found little evidence for a unique role of rumination versus worry in the expression of depression and anxiety symptoms, respectively. Rather, our results were more consistent with recent evidence that both rumination and worry are transdiagnostic risk factors for both depression and anxiety (e.g., McEvoy et al., 2013; McLaughlin & Nolen-Hoeksema, 2011; Nolen-Hoeksema et al., 2008; Nolen-Hoeksema & Watkins, 2011; Olatunji et al., 2013).
We also found very consistent evidence that high repetitive thinkers, who both ruminate and worry, had the highest symptom levels. With one exception, 4 the high repetitive thinkers showed higher levels of depression and anxiety compared to all other profiles in both samples, for both measures of depression and anxiety. Moreover, the high repetitive thinkers were the only group to report symptom levels in the clinically significant range in Study 2, with clinically significant symptoms of both depression and generalized anxiety. These results support the idea that individuals who habitually ruminate and worry tend to have the most maladaptive correlates (i.e., more symptoms of depression and anxiety) that are common targets of many forms of psychotherapy, such as cognitive behavioral therapy. This finding is conceptually similar to prior research indicating that patients with comorbid depression and anxiety have higher symptom severity and worse functional outcomes than individuals with either disorder alone (e.g., Lamers et al., 2011). Individuals who both ruminate and worry may be a particularly important group to target for mental health prevention and intervention.
A few limitations of these studies should be noted. First, we utilized a nonclinical sample, which likely restricted the range of symptoms of observed; an important next step would be to extend this work to individuals diagnosed with major depressive disorder, GAD, or other disorders that are commonly characterized by heightened rumination and worry. For example, individuals with social anxiety disorder might worry about future social encounters and may engage in post-event processing, a specific form of rumination in which an individual broods about his or her performance in a past social situation (Brozovich & Heimberg, 2008). Additionally, rumination has also been associated with escapist behaviors, such as substance abuse and eating disorders (e.g., Aldao et al., 2010; Nolen-Hoeksema, Stice, Wade, & Bohon, 2007). The extent to which rumination versus worry play unique roles in the development and maintenance of other maladaptive behaviors and mental health issues is an important topic for future research. Second, despite utilizing large samples in the present studies, most participants were young undergraduates, limiting generalizability to other demographic groups. Third, we utilized only self-report measures, which are subject to shared method variance. Additionally, the BDI-II and GAD-7 are self-report measures of symptom severity; clinical interviews are required to verify Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5) criteria and make diagnoses of major depressive disorder or GAD. It will be crucial for future research to include other types of assessments (e.g., psychophysiological measures, behavioral observation, ecological momentary assessment) to develop a more nuanced understanding of rumination and worry across diverse contexts for different types of individuals. Fourth, the rumination measure that we used, the RRS-B, instructs participants to report on their responses to depressed mood, whereas the PSWQ-3 includes no such instruction. It is possible that this difference in instructions may have partially contributed to the identification of distinct profiles of ruminators and worriers. However, we view this difference between the two measures as reflective of true differences in the constructs of rumination and worry, rather than a mere methodological artifact. Rumination is defined as a response to depressed mood; worry is not (Nolen-Hoeksema et al., 2008). Additionally, brief measures of both the RRS and PSWQ were used; different results might be obtained with measures that include more items assessing rumination and/or worry. Finally, we only examined two types of repetitive thinking: rumination and worry. We focused on rumination and worry because they are the two forms of repetitive negative thinking with the largest evidence base as risk factors for depression and anxiety (e.g., Mor & Winquist, 2002; Newman, Llera, Erickson, Przeworski, & Castonguay, 2013). In future studies, it will be important to examine profiles of a wider range of repetitive thinking, including stress-reactive rumination (Robinson & Alloy, 2003), positive rumination (Feldman, Joormann, & Johnson, 2008), post-event processing of anxiety-provoking social situations (Brozovich & Heimberg, 2008; Rachman, Grüter-Andrew, & Shafran, 2000), trauma-focused rumination (Ehring, Frank, & Ehlers, 2008), and obsessions (Rachman, 1997). Transdiagnostic measures of repetitive thinking have also been developed, such as the Repetitive Thinking Questionnaire, which are not disorder-specific (Mahoney, McEvoy, & Moulds, 2012). Such transdiagnostic measures offer the advantage of reducing conceptual and measurement overlap with symptom measures but only assess the general tendency to engage in repetitive negative thinking and cannot be used to compare different types of repetitive thinking (e.g., rumination versus worry).
In summary, we identified distinct profiles of repetitive thinking, namely, high repetitive thinkers, ruminators, worriers, low repetitive thinkers, and, in Study 2, average repetitive thinkers. Moreover, we examined associations with symptoms of depression and anxiety to examine where rumination and worry correspond or differ. This study provided a person-centered approach to assess negative repetitive thinking and highlighted areas of future research that hold promise for crystalizing our understanding of rumination and worry. We found support for the existence of separable groups of ruminators and worriers, but our results also supported the conceptualization of these thinking styles as transdiagnostic risk factors that cut across depression and anxiety. We hope that future work in this area continues to use a person-centered approach to better delineate functional similarities and differences among various types of perseverative cognition.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.