
Abstract
Understandings of disability are situated within social, political and economic circumstances. Internationally, medical conceptualisations of disability prevail, influencing policy and practice, creating a discourse which encourages categorisation, diagnosis and prescribed ways of understanding behaviour. This body of knowledge has a profound influence, providing powerful explanatory models of disability. Such discourse excludes other ways of knowing, with little attention paid to competences and the construction of worlds especially from the perspectives of disabled children themselves. This article draws upon a small number of UK qualitative studies which have examined disabled child abuse and included the experiences of disabled children. These studies have highlighted how medicalised notions of disability have led to both medicalised and psychiatrised responses to abuse, which have ill-served disabled children. It could be argued that medicalisation has led to disabled children being labelled as either ‘too disabled’ to be abused or ‘not disabled enough’ to receive an appropriate response which meets their needs; they are also sometimes regarded as showing signs of mental ill health when such signs are more likely to be an understandable manifestation of the trauma of abuse. Evidence collected indicate that much can be learnt from understanding the construction of disabled childhoods and how our current limited exploration of this affects how society prevents, identifies and responds to disabled child abuse and associated trauma. Drawing upon disabled children’s recommendations to ‘see me, hear me and understand me’, this article will argue that in order to protect disabled children and support them to recover from abuse, we need to move away from a tick-box culture of medicalising, categorising, psychiatrising and ‘othering’ to a greater understanding of disabled children’s worlds, and to a rights-based model of disabled child protection whereby we challenge the increased barriers to support faced by disabled children who have experienced abuse.
Introduction
Disabled children across the world are among the most likely to be subjected to sexual and physical violence, neglect and bullying. Prevalence figures are difficult to obtain, predominantly due to a lack of investment in improving measurement, and by a very narrow and often stigmatising definition of disability (Cappa, 2017). An often cited figure, based on a meta-analysis of 17 studies of violence against disabled children, suggests that disabled children are three to four times more likely to experience abuse than their non-disabled peers (Jones et al., 2012). However, this is considered to be an underestimation, given the lack of attention placed on disabled child abuse, and due to the fact that disabled children are often invisible, marginalised, not listened to or heard (Miller and Brown, 2014; Jones et al., 2017; Franklin and Smeaton, 2017). In the United Kingdom, there is a growing body of evidence suggesting that children with learning disabilities constitute a significant minority of sexually exploited children and are at increased risk of sexual exploitation (Beckett, 2011; Brodie and Pearce, 2012; Smeaton, 2009, 2013; Franklin and Smeaton, 2017), and more recently criminal and gang-related exploitation (Children’s Commissioner, 2019), although both forms of exploitation overlap.
Despite this increased risk and higher prevalence, recent studies on disabled child abuse and child protection provision have indicated that disabled children who have been abused often receive inadequate responses and experience barriers to justice (Taylor et al., 2014; Jones et al., 2017; Franklin and Smeaton, 2017). These include the lack of recognition of abuse of disabled children, not being given information and support to empower them to be able to speak out about abuse, not being listened to or their behaviours associated with trauma being ignored or mis-labelled. Moreover, if/when abuse is identified, services are ill-equipped to support them. We would suggest that this is rooted in a predominantly medicalised conceptualisation of disability which influences societal responses to disabled child abuse and affects policy and practice development to meet the needs of this group. Medical discourse encourages categorisation, diagnosis and prescribed ways of understanding behaviour, which ‘others’ and silences disabled children who have experienced abuse and whose experiences and perspectives need to be heard if we are to challenge the barriers they face to receiving appropriate support.
This article draws upon a small number of qualitative UK studies which have examined disabled child abuse and included the experiences of disabled children and young people via in-depth face-to-face interviews. The studies were undertaken within a framework which respected the rights of disabled children to express their views and worked within the social model of disability to ensure that all barriers to participation were eliminated, as far as possible. Due to the consistent recommendations expressed by disabled young participants to ‘see me, hear me and understand me’, this article will argue that in order to protect disabled children and support them to recover from abuse, we need to move away from a tick-box culture of medicalising, categorising, psychiatrising and ‘othering’ to a greater understanding of disabled children’s worlds. Furthermore to a rights-based model of disabled child protection, whereby we understand and challenge the increased barriers to accessing and receiving support faced by disabled children who have experienced abuse.
Background
Disability is a much contested term, with different meanings and associations. The World Health Organization (WHO) defines disability as The interaction between individuals with a health condition (e.g. Cerebral Palsy, Down Syndrome and depression) and personal and environmental factors (e.g. negative attitudes, inaccessible transportation and public buildings, and limited social supports). (WHO and World Bank, 2011)
This bio-psycho-social definition considers disability to be the interaction between impairment and the social and physical environment. It is considered a hybrid between the medical model of disability, which focuses solely on individual impairments, and the social model of disability which argues that exclusion occurs not because of an individuals’ inability to fit into their environment but because of society’s inability to be inclusive. In the 1970s, disability rights activists highlighted the distinction between impairment (lost or limited functioning experienced by a person) and the exclusion and barriers faced by those with an impairment (Union of the Physically Impaired Against Segregation (UPIAS), 1975).
Understanding disability through a social model of disability and holistic way is key to identifying barriers to the protection of disabled children and young people. Barriers may be attitudinal, structural or policy driven. However, medicalised notions of disability have prevailed and led to both medicalised and psychiatrised approaches and responses to abuse, which have ill-served disabled children. The concept of ‘psychiatrised children’ – the focus of this special issue – is highly relevant as this deliberately politicises the assumptions relating to children who have been diagnosed within mental health services and avoids the (mental) health/illness binary dominant in biomedical psychiatry (LeFrançois and Coppock, 2014). It denotes that something has been done to children and young people. In addition, psychiatrisation describes the process by which non-medical or psychiatric issues become defined as a psychiatric or mental health issue, as opposed to children’s emotional distress being regarded as an appropriate response or reaction, which is important in supporting disabled children to recover from abuse.
Psychiatrisation, beyond the psychiatric clinic and hospital, is created and reproduced in multiple contexts and social spaces, such as schools, the media and the family, becoming part of a ‘common sense’ discourse (Goulart, 2017). The range of human emotion becomes narrowly defined and defined as pathological and deviant from the assumed norm. Children become categorised and essentialised, with certain qualities regarded as intrinsic to ‘the child’, without accessing children’s own perspectives and lived experience (Brady, 2014). Brady et al. (2015), along with others, argue that diversity and variation in children’s lives is often overlooked, they are homogenised and decontextualised from their wider lives in policy, practice and in research. This is particularly the case with disabled children, and in the context of their protection. Within child sexual abuse and exploitation practice responses there is a tendency to frame the experiences of young people as a trauma affecting mental health and, in some cases, as mental illness. As LeFrançois and Coppock (2014) state, [. . .] the incompetence that may be attached to a child based on a negative mental health label and the incompetence that may be attached to a child based on age (as well as based on social relations of gender, race and class) mutually constitute each other, allowing sanism to intersect with adultism and other possible aspects of a child’s disadvantaged and socially constructed identity to reinforce and reproduce notions of incompetence and inferiority. (p. 166)
Why do we need to challenge medicalisation and psychiatrisation?
In framing otherwise human experiences of distress as ‘illness’, disability or a disorder, requiring a diagnosis or categorisation, there are social and political consequences for individuals and for wider society. Narratives can become hidden and silenced as young people are perceived to be lacking capacity, mentally unstable (e.g. having borderline personality disorder) and too disabled and/or traumatised to be included and to be heard. Non-medicalised responses to distress become less considered and young people’s own accounts are not validated or legitimated. Social institutions and processes contribute to prejudice and discrimination associated with disability and mental illness, otherwise known as structural stigma. Through encounters with the systems involved in their protection, disabled young people who have experienced child sexual abuse provide examples of such structural stigma.
It can be argued that social workers, and indeed other practitioners, can be implicated in the medicalisation and pathologisation of children and youth, including their life experiences, as a psychiatric and biomedical paradigm is highly influential in practice (Mitchell, 2003; Morley, 2003). Underlying this pathologisation are socio-cultural productions of the problem, deviant, dysfunctional or ill/disabled child (Liegghio, 2016; Osher and Osher, 2002). Liegghio (2016) argues that social workers may inadvertently participate in cultural reproductions that stigmatise children and youth, their lives and ultimately their distress. Negative encounters with professionals where young people are discriminated against, not by individuals but by structures and processes, are not always recognised as such (Liegghio, 2017). For example, perceptions of child victims vary, the ‘culturally approved victim’ (Lamb, 1999: 117, cited in Woodiwiss, 2018: 5) is seen as sexually innocent, passive, lacking in agency, White and middle class – and we would argue ‘not disabled’. Evidence highlights that there still exists reluctance to believe disabled children and young people are abused and/or an underestimation or minimalising of the experiences they may have (Marchant, 1991; Westcott and Cross, 1996; Franklin et al., 2015). This suggests that disabled children face attitudes which specifically discriminate them from receiving appropriate support.
For the disabled children and young people in our studies there exists a double stigma – of experiencing child abuse and maltreatment, and of being regarded as mentally or physically ‘damaged’, ‘ill’, not ‘normal’ and in need of recovery. However, as will be highlighted below, these children often have to prescribe to a medical label and indeed often require a medical diagnosis of a disability to be able to access appropriate post-abuse services that meet their needs. For disabled children, the presence or absence of a medical or psychiatric diagnosis can have significant consequences for the recognition of their abuse (as highlighted above) and for recovery. We need to look carefully at responses and practices to ensure that groups that are routinely oppressed, such as disabled children, are not more likely to experience or need a medical/psychiatric label to have their rights to protection and support enacted. Looking further into the intersectionality of this group is beyond this article; however, we acknowledge further oppression of groups such as, disabled LGBTQ+ young people, disabled young people from a Black and minority ethnic background and issues concerning socio-economic disadvantage and gender. This remains an under-researched area.
Little is known (or it is not well understood) about the ways in which medicalisation and psychiatrisation of children and young people’s experiences play out in the lives of those who have experienced child abuse and neglect. Theorising about the relationship between circulating discourses, institutional responses and children’s lived experience draws attention to the individualisation and responsibilisation of a social and criminal issue. It highlights that what appears to be a caring response concerned with the welfare of children and young people can be contributing to victim-blaming.
In adopting a childhood studies approach to research, understanding children as a specific social group, attention can be directed at children’s rights and the structures that enable and restrict control over their lives (Alanen and Mayall, 2001). If children are a social group, they exist in relation to other groups, which involves paying attention to relations of power, images of ‘the child’ in policy and the ways that children as a minority group are listened to and taken account of in different social settings, such as health care and at school (Brady et al., 2015). Socially and culturally constructed understandings of childhood, coupled with a dominant biomedical framing of disability, impact on children’s capacity for agency and whether child agency becomes constrained or is facilitated: Central to the psychiatrisation of young people are childhood discourses about competence, innocence, risk and criminality. (Liegghio, 2016: 115)
Importantly, the competence and capacity of psychiatrised children are considered diminished by their mental and emotional distress (LeFrançois, 2008). It has implications for autonomy as having a mental health issue may lead children to be considered incompetent and raises questions about capacity to act. Liegghio (2016) states that ‘in the lives of young people adultist and sanist practices intersect’ (p. 116) to justify the denial of autonomy. We would add that this also applies to disabled children and young people.
In summary, medicalised responses prevent distress from being understood as politically and personally meaningful (Mills, 2014). Psychiatric practices are seen as resolving an issue for a young person but they do not address the social and political circumstances which caused/led/contributed to the distress.
There is a long and continued history of oppressive practices towards disabled children and also children with mental health issues. The inclusion of those who have lived experience of distress following child abuse is fundamental to increasing knowledge and understanding and in moving towards alternative ways of knowing.
Methodology/the studies
We draw on data from three studies which sought the views and experiences of disabled children and young people who had experienced abuse (Table 1). The first study (Study A, Taylor et al., 2015; Jones et al., 2017) was commissioned by NSPCC (National Society for the Prevention of Cruelty to Children) and gathered qualitative data from deaf and disabled young people who had experienced abuse and/or neglect from across the United Kingdom. This was a pan-disability study involving seven Deaf young people, and young people with long-standing mental health conditions, learning disabilities and attention deficit hyperactivity disorder (ADHD). Study B (Franklin et al., 2015; Franklin and Smeaton, 2017) was commissioned by Comic Relief and undertook in-depth interviews with young people with learning disabilities who had experienced child sexual exploitation across the United Kingdom. Finally, Study C (Franklin et al., 2019), funded by The Centre of Expertise in Child Sexual Abuse/Home Office, sought the views of young people with learning disabilities/difficulties who had accessed child sexual abuse services. It is important to note that many of the participants across all three studies had multiple impairments, including often undiagnosed/unidentified learning disabilities, autism, ADHD and mental health needs. Together these studies enabled the views of children and young people with a wide range of impairments to express their views and share experiences of service responses to sexual abuse – a subject which as individuals, and collectively, they are predominantly silenced on.
Summary of Research Studies.
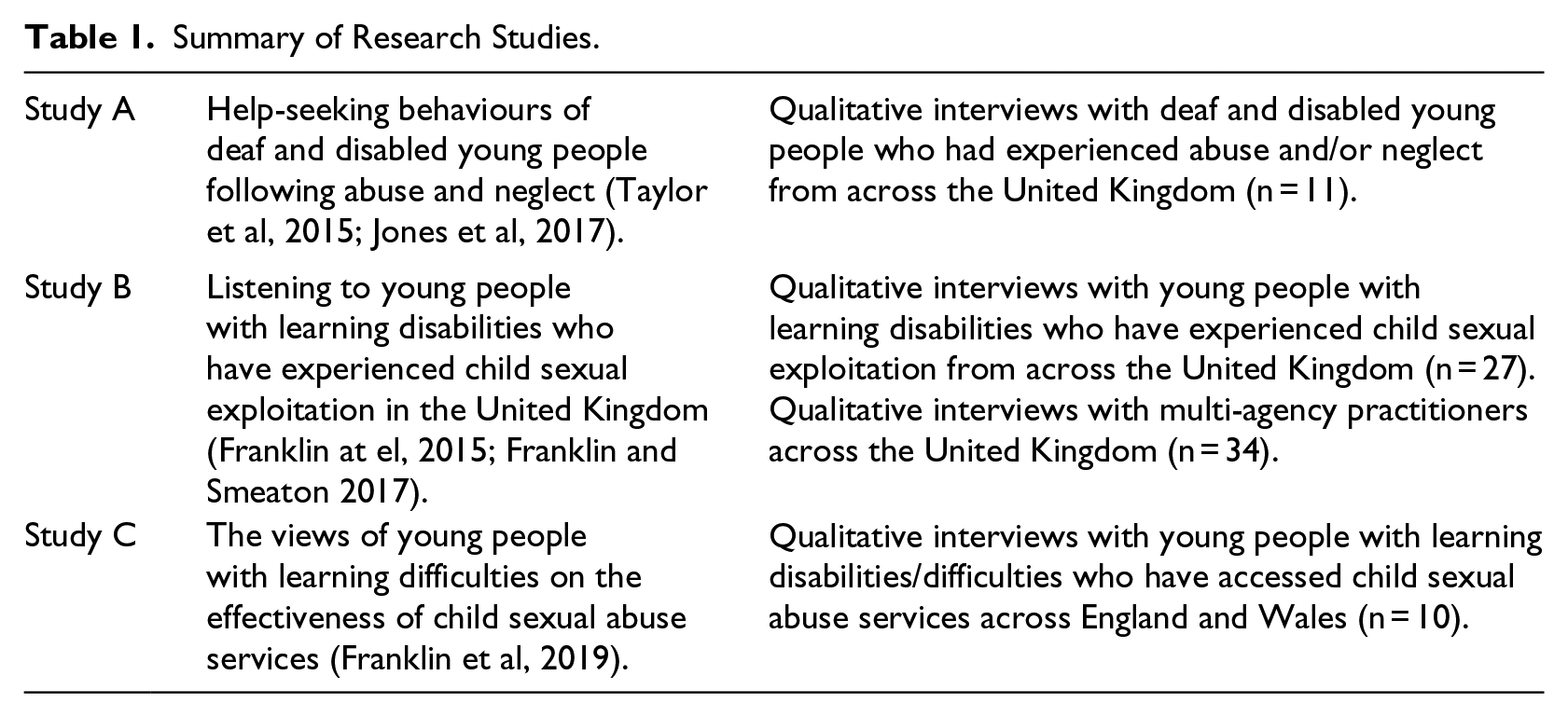
All three studies paid particular attention to ensuring that the young people who were interviewed had support prior, during and post interview – thus they were all recruited via support services. Questions within the face-to-face interviews focused on experiences of service responses. The young people were not asked directly about abuse, however, many chose to talk about their experiences thus it was important that considerable care and attention was given to ensuring an ethical approach was undertaken and the wellbeing of both young people and researcher was safeguarded. Across all studies, data were analysed thematically. The quotes that appear below have been carefully anonymised and contextual data removed which could enable identification. Pseudonyms are used.
A significantly large number of services across the four countries of the United Kingdom were contacted in order to facilitate recruitment of disabled young people to be interviewed across all three studies. Following correspondence with many practitioners across child abuse services, it transpired that vast numbers of services were unable to identify any disabled young people who they had supported and often remarked that they did not have the capacity to work with this group or rarely came into contact with disabled young people – as far as they were aware. Moreover, in identifying young people for the team to interview often there was confusion by practitioners in defining or understanding learning disability, and young people with a diagnosis of autism or Asperger’s were often also included in this category – despite these young people not having a learning disability. This is of interest methodologically and also has implications for the visibility of this group of children for availability of appropriate services to meet their needs, and for accurately recording prevalence rates, issues which we will return to later in the article. It is also of importance to note that when disability services were contacted in studies A and B, many remarked that none of the disabled children they supported had been abused (this was assumed, not necessarily known), and/or that this was not a topic which they would feel able to discuss with disabled children and young people. Thus adding credence to the invisibility of disabled child abuse, despite known increased prevalence.
Initially, the three studies examined the data collected from the young people to address specific practice and policy questions set by the funders of the studies. Findings from these studies have been reported elsewhere, and have been used to inform service responses in the United Kingdom. However, further important methodological and theoretical learning from across these three unique studies was warranted, and thus secondary analysis of the data across the studies was undertaken alongside an examination of field notes, and researcher reflections. The following presents methodological learning and theoretical discussion from across the three studies. The data clearly identify two themes of relevance to our focus on psychiatrisation:
Prevalence of a medical model of disability which underpins how disabled children are defined, and seen, as victims of abuse. This medicalisation appears to affect whether their abuse is identified, if they are believed when disclosing or displaying behaviours which might indicate trauma, and their ability to be able to access post-abuse services which meet their needs. Medicalised notions of being ‘too disabled’ or ‘not disabled enough’ define children’s experiences.
Medicalisation and psychiatrisation of disabled young people’s experiences of abuse leading to inappropriate responses by child abuse services. Responses which can victim-blame children, silence them, inappropriately label them and again not meet their needs for support.
Findings
Medical model of disability: impact on identification of disabled children as victims of abuse and immediate responses when abuse is identified
As discussed above, evidence has highlighted that there still exists a reluctance to believe that disabled children and young people are abused, leading to discriminating responses (Marchant, 1991; Westcott and Cross, 1996; Franklin et al., 2015). From our undertaking of research in this field, evidence suggests that there needs to be a more nuanced understanding of this and the impact that such misunderstandings have on disabled children who are experiencing abuse. From our interactions with child abuse services, through interviews with multi-agency practitioners within Study B, and from the hearing the experiences of disabled children across the studies, we identified that there exists a more nuanced conceptualised spectrum of disability, albeit still medicalised, which determines whether a child’s abuse is recognised and responded to.
‘Too disabled’ to be sexually abused
We encountered assumptions that disabled children are not abused, underpinning this appeared to be the notion that these children were ‘other’, different from their non-disabled peers and thus somehow protected from abuse. Utilising a medicalised model, this group of children were described as those with more ‘severe’ physical, communication or learning needs – those who can be easily and visibly identified as ‘disabled’. Ideas prevailed that possibly because these children’s bodies and/or minds are so ‘broken’, ‘damaged’ or ‘sick’ they would not be targeted by perpetrators of abuse, despite the fact that the very nature of their impairments can create vulnerabilities, which are exploited.
Evidence from other studies has indicated that such children are often not believed, and/or their communications of distress or trauma are assigned to their impairment rather than a manifestation of abuse (Miller and Brown, 2014; Jones et al., 2017; Franklin and Smeaton, 2017). At this end of the spectrum, over-medicalising disability can lead us to not seeing the child, or seeing past an impairment, leading to their abuse remaining hidden.
As previously stated, when approaching services to recruit participants for the studies, it appeared that this idea of disability prevailed, with most services indicating they did not support disabled children. Where possible, further correspondence often identified that they did in fact support disabled children – albeit not disabled children who would fit the above medicalised definition of disability and could easily and visibly be identified as ‘disabled’. The disabled children that they were supporting were not seen as disabled, which had ramifications for the child in accessing a service that did not understand their needs and/or the barriers they might face to getting good support.
Being ‘too disabled’ to be abused is illustrated through the following examples. In Study B, young people told us of their experiences which indicated that professionals had neglected to consider that abuse could, or was occurring because they had not considered it possible for young people with their impairments. Two examples illustrate this, both of which concern young men under 18 years old, one with a learning disability and one who is autistic. With the first young man, due to his learning disability, it had not been considered important to teach him about safe sex and to have conversations with him about his sexuality, consent and/or what healthy relationships should be. He was also not believed when he described numerous men sexually exploiting him in a local park.
The second young man similarly had not had conversations about his sexuality, and through his own exploration of whether you can be both gay and autistic, he had been sexually exploited online. This also became physical and sexual abuse. In both cases, we are not suggesting that giving information to these young people could have prevented the abuse, however, an assumption was made that disabled young people did not need to know about sexual consent, personal safety, sexuality and healthy/unhealthy relationships, an overarching medicalisation of disabled children had prevented professionals from seeing the young people and their right and need for information, and ultimately protection.
No recognition of impairment-related needs impacting responses to abuse
Conversely, at the opposite end of the spectrum, we also identified children and young people who were seen as ‘not disabled enough’, or there was no recognition of impairment-related needs because of a lack of a medical or psychological diagnosis and/or they did not fit the medicalised profile of a ‘disabled child’. This impacted on whether their abuse was identified and responded to appropriately. These children were often seen as ‘bad’, on the edges of criminalisation, excluded from education, sometimes misusing alcohol and substances, and quite possibly being targeted by ‘gangs’. However, their learning disabilities, ADHD, autism or other impairments, and indeed their abuse, remained hidden under the radar as services focused on their ‘badness’ and troubling behaviour. Many disabled young people that we interviewed explained how at school their disability-related needs had not been met, leading to a deterioration in their behaviour and attendance, and ultimately exclusion, isolation and the creation of circumstances where they could be targeted and exploited, including sexually. Their victimisation continued as they described behaviours which were understandably a manifestation of trauma (e.g. challenging of authority, anger, misusing substances, going missing) which were assigned to their ‘badness’. In most cases, these young people were not known to Disability Services as they did not meet the high threshold for support or had not been referred to services.
One participant expressed her frustration that her extremely challenging behaviour was not recognised as a sign of distress and an indication of abuse by her foster parents. This young woman was Deaf and in foster care and therefore, in regular contact with services. She felt, The social workers should have thought why I was always so angry, why I was always behaving badly to the foster parents.
Another participant in Study A, whose abuse began at age 8, attempted suicide at 9 years. She was admitted as a psychiatric in-patient, assessed and treated many times over the course of her young life but at no time felt she was given an opportunity to disclose her abuse – the focus and service response had been placed on diagnosing her mental illness and treating the symptoms of the trauma of abuse. She explained, when I first started showing signs of mental illness I think someone should have sat down and asked me why ‘cause it’s not a normal thing for an 8 year old to do.
From these two examples it seems that even when disabled children display expressions of distress which bring them into close contact with services, this does not necessarily increase the likelihood of detection or prevention of abuse. Participants described a number of behaviours that children used to communicate their abuse and convey their distress. As the first young woman went on to explain, I tried to tell people quite a lot of the times, like when I was nine I was Sectioned because I tried to kind of take my life kind of thing cos I couldn’t handle it anymore and I was Sectioned for like three months and even then nobody asked me why did I do it.
This child’s actions appear to have been interpreted as an expression of distress caused by her chaotic family life and inherited ‘mental illness’, without any additional explanations being considered. Such inappropriate and limited responses are further explored in the next section.
Medicalisation and psychiatrisation of disabled young people’s experiences of abuse, leading to inappropriate responses by child abuse services
Even when overcoming the barriers noted above that exist for disabled children, and having their abuse recognised and responded to, there exist very few specialist services, or generic services which state that they support disabled children who have experienced child sexual abuse (Franklin et al., 2019). (Note: Across all studies, we were unable to access children to interview who had accessed specialist post-abuse Disability Services, there are only a handful of such services across the United Kingdom.) Thus, in the United Kingdom, most disabled children either do not receive any post-abuse support (Taylor et al., 2015) or access a service that may be ill-equipped to meet any impairment-related needs. When abuse of disabled children was recognised, the evidence indicates that medicalisation continues, and furthermore psychiatrisation, with some child abuse services medicalising young people’s experiences.
Predominantly support consisted of a Child and Adolescent Mental Health Service referral, and possibly counselling, or activities focused on prevention of further abuse. Evidence suggests that these responses rarely met the child’s needs at the time, enabled their agency or understood their experiences. In most cases, young people spoke of responses which can be described as further medicalisation or psychiatrisation. Across all three studies, when asked what would have helped, disabled young people spoke at length of relationship-based support where they were listened to and understood – and not medicalised and pathologised.
To illustrate, the evidence indicates that decisions are often made quickly and in isolation from the child, to provide a therapeutic intervention, sometimes within a Child and Adolescent Mental Health Service (CAMHS). Disabled young people reported that they need time to process the experience of being abused and/or sexually exploited before they were ready for psychological/psychiatric intervention, but often services are provided too soon after the event: It was planned badly . . . it was all on top of each other . . . everything just piled in all at once . . . looking back on it now, I could do with it (therapy) now more than anything because I’ve processed it more. (Young person accessing a sexual violence service)
Another young woman said, There was a lot going on at the time and it was very quick . . . (Young person accessing a complex safeguarding service)
Young people expressed how they wished to change how quickly such services came into their lives and for services that offered this avenue of support to be timely, responding to the needs of the individual young person.
Therapy was differently described than other forms of received support. For example, in support provided by specialist child sexual exploitation (CSE) or sexual violence services, ‘we talk about things. If I’m stressed I’ll just talk to her’ or ‘I could rant about my week . . . it’s just talking’. These less formal means of support were found to be helpful, especially in allowing young people to ‘open up’ in their own time, rather than within a prescribed intervention appointment time.
Feeling supported, helped and having someone to talk to about anything were really important to young people. They particularly valued not being ‘forced to talk about things in a way you don’t want to’, ‘it feels like a friend but it’s not a friend, do you know what I mean?’
Yet the support services could also be guilty of stigmatising young people, by taking an approach which was often focused on changing their behaviours and any perceived ‘risk taking’. The approach of some exploitation and sexual violence services could be said to have influenced internalised degrees of blame for the young people’s abuse. They used language which implied that they felt responsibility for their abuse, for example, ‘not putting myself in danger’, ‘being better behaved’, ‘not do stupid stuff’, ‘if it happened again don’t make the same mistakes’, ‘trying to make myself a better person’. This seems to resonate with previous research which unpicks the consequences of a professional focus on individual deficit and deviance from the norm: For psychiatrised children and youth, their competence and capacity is considered diminished both by their mental and emotional distress and by notions that a young person does not have the wisdom to predict the consequences of their decisions. (Liegghio, 2016: 122, citing Brannen and O’Brien, 1995; Dalrymple, 2005; Ekmann-Ladd, 1996; Kellet et al., 2004; LeFrançois, 2008)
In the cases of our three studies, there were many examples where not only mental distress but an impairment was assigned to lacking capacity, and thus particular attention in services was focused on ‘training’ disabled young people to understand the consequences of ‘risky behaviour’ and/or behaviour which was seen as ‘challenging’.
The evidence also indicated that there was an interesting tension between being perceived as having mental ill health, often as a result of the abuse, and in having low self-esteem or vulnerability which almost ‘invited’ abuse. Both are individualising in their focus and exacerbate the belief that there is something wrong with the sexually abused young person, without acknowledging their lack of power or choice in the abusive situation. The response to both was to provide strategies and coping mechanisms to deal with emotional responses (including self-harm) and to prevent future abuse. Other researchers have drawn attention to victim-blaming language in sexual abuse practice and interventions (Brown et al., 2016; Franklin et al., 2019; Eaton and Holmes, 2017). There has long been a concern with the balance between care and control relating to children, a further manifestation of this is in balancing ideas of risk with those of responsibility and accountability for behaviour.
When services are not meeting either the impairment-related needs or understanding the manifestations of trauma responses to abuse, young people reported exerting their agency and developing strategies in order to resist their influence. One young woman describes her experience of children’s mental health services: I didn’t like them (CAMHS) . . . it was so patronising. They were basically telling me, instead of physically hurting myself, hold an ice cube so you can hurt yourself without leaving any marks. So it wasn’t really helpful, so in the end I just pretended to be better so that I could leave. (Young person accessing a sexual violence service)
A Deaf young woman who uses British Sign Language also explained that she had been offered counselling immediately following the abuse investigation by the police but that it was so unhelpful that she withdrew after only one session and no further follow-up was offered: I did have counselling but with a woman who couldn’t sign. She would use a laptop to communicate with me. She typed, ‘How are you?’. I thought it was strange. I typed back ‘I am ok’. She said, ‘Do you want to talk about anything?’ . . . It wasn’t possible because we couldn’t communicate with each other.
On other occasions, educational support was not provided if a young person was not perceived to be impaired enough, with an assumption that the impact of sexual abuse was short term: (The support worker) would maybe email my school and say ‘she’s struggling’ or ‘feeling upset’ or whatever, I think they (school) thought ‘It’s over, she’s fine now, she can get back to all her work’ . . . I’m on my final warning because I’m behind on my work and I’ve missed lessons. (Young person accessing Child Sexual Exploitation service)
Another young woman who had a diagnosis of autism felt that she was treated ‘like glass or like a brick’ within her school – autism was sometimes acknowledged and she was treated as ‘special or different’, perhaps because of a fear of the unknown (glass); alternatively, at other times because there was no understanding of autism it was not acknowledged and no accommodations or adjustments were made (brick). This was coupled with the school having little understanding of potential affects of abuse: They just blow you off like, ‘ugh, go away peasant, I don’t have time for you’. Some of them just completely ignore the fact that I have autism at all. (Young person accessing post-abuse therapy)
Concluding reflections
The development of social science understanding is critical in order to challenge narrow conceptualisations of childhood disability. No more so than when examining societal responses to child sexual abuse, and upon hearing the experiences of disabled children and young people who have experienced sexual abuse. These studies have shown that disabled children and young people are ill-served by the systems, structures and professionals charged with protecting and supporting them. Medical discourse relating to disabled children encourages categorisation, diagnosis and prescribed ways of understanding which does not enable reflection upon the ways that disability, childhood and victim status are constructed and interplay.
A common tactic used to establish a dominant position in a contentious field is to present a position that appears to be common sense and rational. Of course we should be responding with interventions for young people who have experienced child abuse. However, upon hearing from the experiences of disabled children it is clear that current practice is not meeting their needs. Crucially, due to this dominant discourse of ‘too disabled’ to be abused or ‘not disabled enough’ to be abused, little attention has been paid to the need to develop appropriate preventive approaches, support those around the child to identify signs of abuse or develop accessible, adequate responses and therapeutic recovery services.
Psychiatrised/psychologised/therapeutised interventions are often regarded as the solution to children and young people’s distress following abuse – abuse expressed verbally, emotionally or through externalised behaviour. Yet such distress has been caused by social and politically violent acts and is both a rational and understandable stress response to the experience of abuse or exploitation, rather than evidence of mental ill health. An alternative framework for distress of disabled children and young people arising from child abuse is urgently needed, in particular, a framework that recognises abuse in the lives of children that do not conform to the image of an ‘ideal’ or ‘culturally appropriate’ victim.
By increasing a social, cultural and political understanding of childhood disability, mental health and illness, responses from practice are likely to be more informed and more appropriate. Across the three research studies, our research found that what disabled children and young people want is an increased understanding of how to make information and support accessible and to communicate clearly, in a way that suits the young person; allowing extra time to process information; proceeding at their own pace and embracing what they need to be able to relax and reduce anxiety (Franklin et al., 2019). There is also need for other ways of encouraging children and young people to speak out or communicate about abuse. Most importantly there needs to be a move away from medicalised notions of disability to an approach that keeps the child at the centre and recognises the increased risks of abuse for this invisible group, so that those children who cannot speak out are seen and heard. Practice which serves to medicalise and psychiatrise disabled children, not only within health services but also across other support services who are working within a medical rather than social model approach, must be resisted.
Current discourse pays little attention to meaning making, competences and the construction of worlds from the perspectives of disabled children and young people themselves. We need to move away from a tick-box culture of medicalising, categorising, psychiatrising and ‘othering’ to a greater understanding of disabled children’s worlds, and to a social relational, rights-based model of disabled child protection whereby we understand and challenge the increased barriers to support faced by disabled children who have experienced abuse. The young people in these studies have shown that we need to question current practice of child abuse services, as it appears that they are potentially not helping them to make sense of the experience in the context of their lives or they provide a very particular understanding of the experience (often focused on the young person’s behaviour and/or impairment). This prevents disabled children from being seen, heard, listened to and understood, and to receiving a child centred, children’s rights approach to protection and provision.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: (Study A) NSPCC (National Society for the Prevention of Cruelty to Children, (Study B) Comic Relief and the Centre of Expertise on Child Sexual Abuse (Study C).