
Abstract
Introduction
This report demonstrates the importance of making a diagnosis in patients with chest pain, rather than simply excluding myocardial infarction.
Case history
A 70-year-old man with hypertension but no other medical history was admitted with chest pain, described as ‘sharp’ with no radiations, and 10/10 in severity. There was no associated nausea or sweating; the pain came on at rest, although he had been doing an unusual amount of heavy lifting prior to the admission. He had no modifiable cardiac risk factors other than hypertension. He had been given glyceryl trinitrate spray and morphine by paramedics and the pain had resolved within 10 min. Clinical examination was normal, with a heart rate of 64 beats per minute, blood pressure 146/90 mmHg and no murmurs. There was no neurological deficit and there were no abdominal masses.
Initial serum troponin I was 62 ng/L (reference range< 40 ng/L) and repeat after 8 h was 48 ng/L. ECG showed deep anterolateral T wave inversion (Figure 1). The initial working diagnoses were of an acute coronary syndrome or musculoskeletal chest pain, on a background of left ventricular hypertrophy (LVH). Bedside echocardiography showed significant apical hypertrophy (2.7 cm wall thickness) with no other abnormalities and no features of aortic dissection. Chest radiography was normal. The patient was not hypoxic or breathless and therefore a pulmonary embolism was thought unlikely.
ECG.
Initial treatment consisted of continuing this gentleman’s usual lisinopril, and adding in bisoprolol as he remained hypertensive. He was not given antiplatelet therapy. A cardiac magnetic resonance (CMR) scan was performed to confirm the suspected diagnosis of hypertrophic cardiomyopathy (HCM).
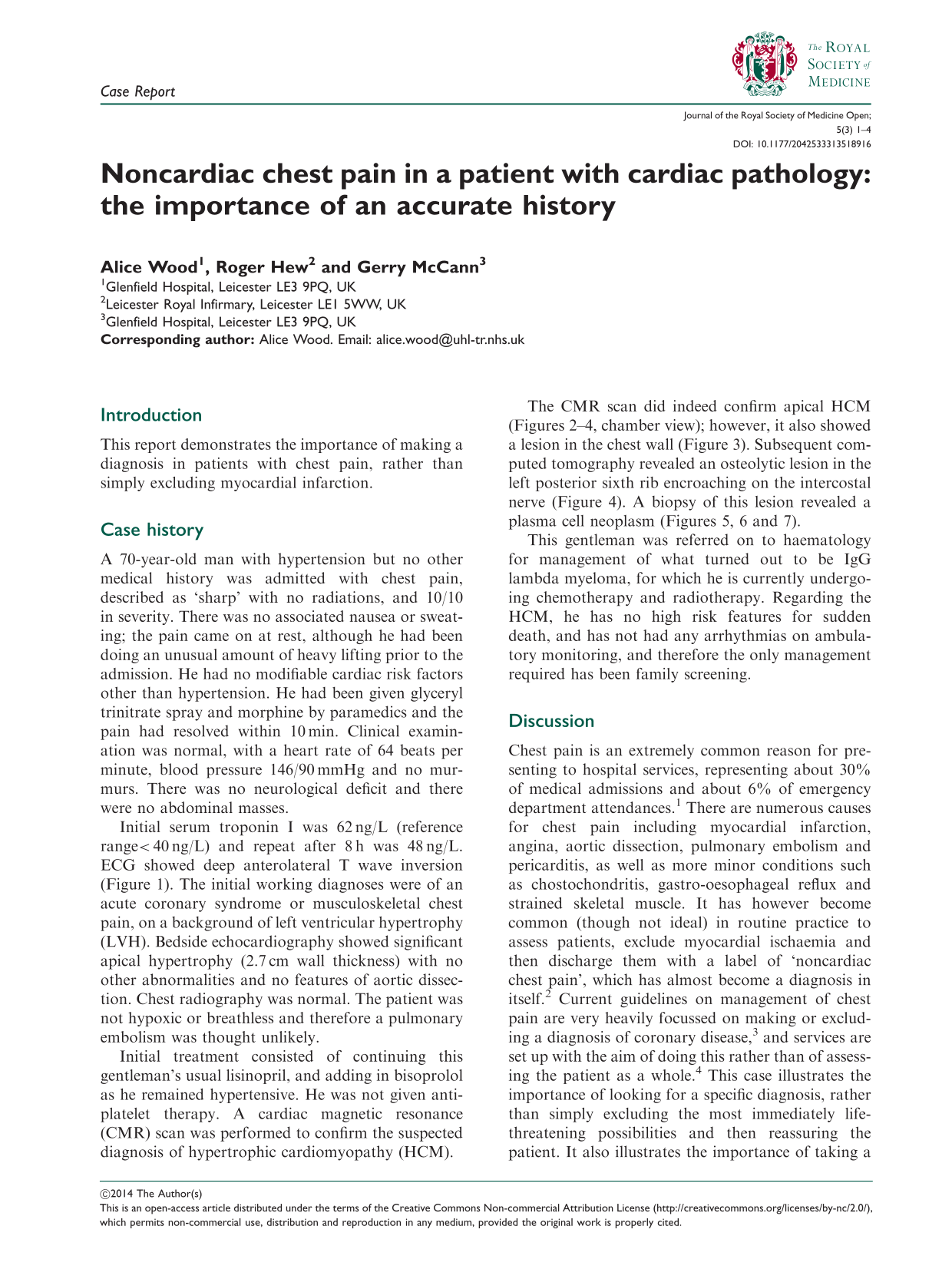
The CMR scan did indeed confirm apical HCM (Figures 2
–4, chamber view); however, it also showed a lesion in the chest wall (Figure 3). Subsequent computed tomography revealed an osteolytic lesion in the left posterior sixth rib encroaching on the intercostal nerve (Figure 4). A biopsy of this lesion revealed a plasma cell neoplasm (Figures 5, 6 and 7).
MRI, four-chamber view – systole and diastole. MRI showing image revealing left posterior chest wall lesion. CT image showing chest wall lesion encroaching on intercostal nerve. Plasma cell infiltration. Haematoxylin and eosin section, ×10 magnification. Plasma cell infiltration including atypical forms. Haematoxylin and eosin section, ×40 magnification. CD138 immunohistochemical marker highlighting the plasma cells, ×40 magnification.





This gentleman was referred on to haematology for management of what turned out to be IgG lambda myeloma, for which he is currently undergoing chemotherapy and radiotherapy. Regarding the HCM, he has no high risk features for sudden death, and has not had any arrhythmias on ambulatory monitoring, and therefore the only management required has been family screening.
Discussion
Chest pain is an extremely common reason for presenting to hospital services, representing about 30% of medical admissions and about 6% of emergency department attendances. 1 There are numerous causes for chest pain including myocardial infarction, angina, aortic dissection, pulmonary embolism and pericarditis, as well as more minor conditions such as chostochondritis, gastro-oesophageal reflux and strained skeletal muscle. It has however become common (though not ideal) in routine practice to assess patients, exclude myocardial ischaemia and then discharge them with a label of ‘noncardiac chest pain’, which has almost become a diagnosis in itself. 2 Current guidelines on management of chest pain are very heavily focussed on making or excluding a diagnosis of coronary disease, 3 and services are set up with the aim of doing this rather than of assessing the patient as a whole. 4 This case illustrates the importance of looking for a specific diagnosis, rather than simply excluding the most immediately life-threatening possibilities and then reassuring the patient. It also illustrates the importance of taking a detailed history and not being misled by the circumstances in which the patient presents – in retrospect this patient’s pain was not anginal in character, but as he presented to a coronary care unit with an abnormal ECG it was felt necessary to exclude an acute coronary syndrome.
HCM can cause chest pain (usually typical angina even in the presence of normal coronary arteries, due to increased demand and sometimes due to high diastolic pressures impeding coronary flow); however, this was not felt to be the case here. HCM is an autosomal dominant condition with a prevalence of 1 in 500. 5 Apical forms, which represent about 7% of HCM cases in western populations, are thought to be more benign. 6
Myeloma is a bone marrow-based, multifocal plasma cell neoplasm associated with a monoclonal immunoglobulin called M-protein (most commonly IgG) in serum and/or urine; in about 5% of cases it occurs as an isolated plasmacytoma, as was initially the case in this patient. Myeloma is more common in men than women (1.4:1) with a median age at diagnosis of 70 years. 7 It is most commonly diagnosed via serum and urine electrophoresis rather than by direct biopsy of a specific lesion. It causes multiple lytic lesions throughout the skeletal system, with the ribs being affected in about 45% of patients. It presents in a variety of nonspecific ways, including pathological fractures, tiredness and other symptoms of hypercalcaemia, recurrent infections and renal impairment. 8 Chest pain as the first presenting symptom of myeloma has been reported 9 but is not a common presentation. Extraosseous plasmacytoma rarely progresses, whereas osseous plasmacytoma is thought to represent early myeloma and generally progresses to the systemic disease. Myeloma can be associated with LVH because of amyloid deposition within the heart; however, this was clearly not the cause of the LVH in this gentleman – his ECG would be very atypical for cardiac amyloid, and his MRI scan demonstrated regional (apical) hypertrophy with normal gadolinium kinetics and nulling. Cardiac amyloid would be expected to show global subendocardial late gadolinium enhancement and high myocardial gadolinium concentrations early after injection. 10
On this occasion the extra cardiac diagnosis was essentially made by luck – if the diagnosis of HCM had been made conclusively on echocardiography, he would have been discharged home without the plasmacytoma being identified. However, it illustrates the importance of taking a detailed history and not being misled by the circumstances in which the patient presents, or by the apparently obvious cardiac diagnosis. In retrospect, this patient’s pain was not anginal in character, and is likely to have been due to the plasmacytoma encroaching on an intercostal nerve, but as the patient presented to a coronary care unit with an abnormal ECG, it was felt necessary to exclude an acute coronary syndrome.