
Abstract
Invasive candidiasis (IC) is associated with high mortality in intensive care unit (ICU) patients. Timely diagnosis of this potentially fatal condition remains a challenge; on the other hand, the criteria for initiating empirical antifungal therapy in critically ill patients are not well defined in different patient population and ICU settings. Alongside the international guidelines, reaching regional and local consensus on diagnosis and management of IC in ICU setting is essential. This report summarizes our present status of IC management in ICU, considered by a group of Iranian experts in the fields of intensive care and infectious diseases. A round table of 17 experts was held to review the available data and discuss the optimal treatment strategies for IC in critical care setting. Comparative published data on the management of IC were analytically reviewed and the commonly asked questions about the management of IC in ICU were isolated. These questions were interactively discussed by the panel and audience responses were taken to consolidate point-to-point agreement with the panel arriving at consensus in many instances. The responses indicated that patients’ risk stratification, clinical discretion, fungal diagnostic techniques and the empirical therapy for IC are likely to save more patients. Treatment options were recommended to be based on the disease severity, prior azole exposure, and the presence of suspected azole-resistant Candida species. This report was reviewed, edited and discussed by all participants to include further evidence-based insights. The panel expects such endorsed recommendations to be soon formulated for implementation across the country.
Introduction
Antifungal therapy in high-risk patients with severe sepsis is often started in the absence of proven disease and mainly based on the high clinical suspicion for invasive fungal infections (IFIs). 1 The local epidemiology for fungal infections and the prevalence for each of the species at a given care facility may provide physicians with useful clues for the empirical treatment of such infections. In the intensive care unit (ICU) setting, a timely treatment approach for fungal infections is often mandated due to the high mortality attributed to invasive candidiasis (IC) and the lack of precise and reliable diagnostic tools for this condition. 2 –4 It is often not possible to wait for the culture results and the empirical approach becomes warranted. This treatment strategy is shown to result in reduced IFI-related mortality in ICU. 1,3,5
Taken into consideration the international guidelines, arriving at a consensus by Iranian intensive care and infectious diseases experts was deemed necessary in order to improve our current situation in the diagnosis and management of IC in critical care settings. Accordingly, experts from the two disciplines of critical care medicine and infectious diseases attended a round table discussion on 28 July 2013. This report provides a brief review of the literature published by both international and local field authorities on the role which IFI plays in mortality and morbidity of ICU patients. The applicable predictive and diagnostic tools and their place in the clinical management approaches, based on the current international guidelines, were addressed. The consensus from the experts’ panel which is outlined in the present report revolved around three pivotal issues: (1) when to suspect and how to diagnose IFI in ICU setting? (2) when to start prophylactic, preemptive and empirical treatment? and (3) what treatment options to take?
IFIs in ICU: how big is the problem?
IFIs have dramatically increased over the past 20 years. Some contributors to this rise are thought to be the aging population with life sustaining therapies such as widespread use of broad spectrum antimicrobial therapy and the emergence of resistant microorganisms, hemodialysis, widely used invasive medical devices, bone marrow transplantation, solid organ transplantation, chemotherapy regimens and HIV. 6
The major risk factors for developing IFI include prior antibiotic use, central venous catheterization, total parenteral nutrition (TPN), a recent major surgery, use of steroids, dialysis and immunosuppression. 7 ICU length of stay is considered to be an important risk factor with the rate of infections notably rising after seven to 10 days. 8
IC is the fourth leading cause of bloodstream infections and the most common IFI accounting for 70–90% of all invasive mycoses 9 with increased cost, morbidity and mortality, especially in ICUs. 10 Studies have indicated IC occurring seven to 15 times more frequently than aspergillosis. 11 It has been estimated that up to 10% of nosocomial disease is attributed to candida infections 12 and almost half of all candida infections occur in ICU. 13 In other words, the incidence of IC in ICU appears to be almost 10 times bigger than the medical or surgical wards. 10,13,14
Epidemiological insights and the treatment rationale
Candida albicans and Aspergillus fumigatus are the main pathogens responsible for IFIs. In ICU patients however, candida infection accounts for the most prevalent cause of IFIs. 1,10 Together with the growing incidence of IC in critically ill patients, the spectrum of pathogenic Candida species has also been changing. Although Candida albicans (accounting for 40–60% of IC) is still the most common pathogen, there has been a significant recent shift towards non-albicans strains, i.e. Candida glabrata, Candida tropicalis and Candida Krusei causing infection in 20–30% of cases. 15,16 This change in the epidemiological patterns may at least be partly due to the widespread prophylactic and therapeutic use of fluconazole. 17 In ICU patients, infection with C. glabrata is shown to be associated with relatively higher mortality than other Candida spp. 15 Studies on the rate of attributable mortality of invasive candidemia in different subtypes have shown that C. glabrata and Candida Krusei are the main subtypes resulting in a mortality rates of more than 50%. 18
With an overall estimated mortality rate of 50–75% and 40% for invasive aspergillosis and IC, respectively, IFI imposes a significant healthcare cost burden. 19 Particularly in ICU patients, the high incidence rate of IC (9.8 per 1000 admissions) carrying high morbidity (increased length of stay up to 22 days) and mortality rate (almost 30–40%) consumes a significant share of limited resource. 20 –22 A recent study substantiated that patients with and without candidemia had an ICU crude mortality rate of 52.6% versus 20.6%, respectively (p < 0.001). 23
A local report on nosocomial fungal infections in ICU and transplant wards revealed that most prevalent fungal infections appear to result from Candida albicans, Penicillium spp., Aspergillus niger, and Cladosporium spp. where environmental fungal contamination was shown to be more prominent in ICU. Moreover, the length of hospital stay was shown to play a major role in colonization of fungi in critical care settings. 24
In other local studies on fungal infections in children with advanced kidney disease undergoing peritoneal dialysis 25 and adults with kidney transplantation, 26 the role of Candida spp. was shown to be dominant. Furthermore, a multi-centre analysis on the prevalence of IFIs as deep-seated mycosis through direct and culture examinations in immunocompromised hosts (in Tehran, Iran) revealed that Candida spp. tend to be isolated in 70.4% (39.4% C. albicans and 30.9% non-albincans) and Aspergillus spp. in 14.1% of the examined cases. 27 Our so far available epidemiological data in Iran appear to be more or less in line with those international rates. 28,29
Given the above insights on the prevalence of IFI in critical care setting, the key issue helping to reduce the heavy burden imposed by IC is known to be timely and appropriate interventions. Different studies 30,31 have indicated that IFIs’ wide range of mortality rates (22–97%) mainly depends on the time of intervention.
Prompt clinical suspicion and timely diagnosis of IC still remains a challenge as fungal cultures and sensitivity may not be readily available globally, fungal cultures and non-culture-based diagnostic tools lack necessary sensitivities and in many instances awaiting cultures or other paraclinical reports could potentially delay definitive management. Therefore, clinical predictive rules and scoring systems could act as a bridge to prevent detrimental delays in instituting management with its antecedent increase in morbidity and mortality.
With regard to antifungal therapy timing, the empirical approach guided by practical experience, observation and non-specific evidence in a given high-risk patient, is clinically supported by different authors. 3,21,22,31 Therefore, the risk factors for IC in critically ill ICU patients should be well defined and the population at highest risk should be targeted promptly for empiric therapy regardless of the availability of the paraclinical reports or definitive diagnosis. 32,33 The empirical approach which mostly depends on clinical suspicion is shown to result in better outcome in high-risk patients admitted to ICU. 1,3,10
The recent increase in fluconazole-resistant Candida species has encouraged the use of other antifungals such as echinicandins. 17,34 The high activity, broad spectrum and low toxicity profile of these agents, of which caspofungin is currently available in Iran, make them ideal agents for empirical use against IC. 35,36 The most recent IDSA (Infectious Disease Society of America) 35 and ESCMID (European Society for Clinical Microbiology and Infectious Diseases) 34 guidelines have recommended the empirical antifungal therapy in critically ill patients with risk factors for IC without any other known cause for fever.
Given the high mortality, other than the empirical approach, prophylactic and preemptive therapy might become indicated in distinct high-risk populations for candida infection. 4 With regard to the targeted therapy, upon documentation of candidemia, the infecting strains should be identified for appropriate therapy as Candida species are variably susceptible to different antifungals. 37
The above insights reemphasize the clinical burden and the significance of appropriate clinical decision making on therapeutic approaches in IFI within ICU. As substantiated in an earlier consensus report from a group of infectious disease experts in Iran, early initiation of antifungal therapy may reduce the IFI burden in ICU; however, the widespread use of the available therapeutic options should be balanced against their cost and benefits as well as the potential emergence of resistance. After all, the empirical antifungal therapy approach was considered a strongly recommended approach in this report. 38
IC in ICU-admitted patients, the implications of available scoring systems
According to a recent survey, 50–80% of the critically ill patients who were admitted to ICU had already been exposed to risk factors for IC, 5–15% had candida colonization on admission and 5–30% actually had IC. 29 In the presence of such a clinical prevalence and impact, the diagnosis of IC in critically ill patients remains difficult. Both culture and non-culture-based diagnostic measures are subject to noticeable pitfalls.
Cultures from non-sterile sites are mainly colonization and blood cultures for candidemia become positive in only half of the cases.
28
Despite this lack of sensitivity, fungal blood culture remains the gold standard for IC diagnosis. Culture-based diagnosis and species identification is time-consuming and dependence on the culture results only delays therapy.
28,39
Nevertheless, newly introduced non-culture-based techniques such as 1,3 -β-
The 1,3-BG test is shown to have false-positive results among ICU patients with a generally low (<70%) specificity in hospitalized patients. Some of the main attributable factors for the false-positive results of this test are hemodialysis, gauze contamination during surgery, intravenous immunoglobulin (IVIG) administration, bacterial infections, and the use of antimicrobial drugs such as colistin, ertapenem, cefazolin, cefotaxime and ampicillin-sulbactam. 39,40
Given the above and based on the earlier insights on the incidence of IC among high-risk ICU patients, some risk prediction models have been developed. 5,10,43,44
The most popular prediction rule and scoring system for IC in non-neutropenic adult patients are Ostrosky-Zeichner model 45 and Candida Score. 44 According to Ostrosky-Zeichner prediction rule with the sensitivity, specificity, positive predictive value and negative predictive value of 34%, 90%, 10% and 97%, respectively, patients with indwelling central venous catheters who have received systemic antibiotics and have at least two of the following: TPN, any dialysis, any major surgery, pancreatitis, any steroid therapy or immunosuppression, are considered potentially high risk to develop IC. 10,45 Candida Score is based on the presence or absence of conditions (with the coefficient β or individual risk scores in brackets) such as TPN (0.908), surgery on ICU admission (0.997), multi-focal Candida spp. colonization (1.112) and severe sepsis (2.038). Patients with a score of >2.5 are at high risk for development of IC. 44 With the sensitivity of 81% and specificity of 74%, one may only need the presence of sepsis and any one of the three other remaining risk factors or the presence of all of them together except sepsis in order to consider starting antifungal treatment for a particular patient. 32,44
The clinical suspicion for IC based on these scoring systems can provide physicians with an easy tool for timely administration of an appropriate antifungal agent. 44,45
Therapeutic approaches in IC, the position of international guidelines
Therapeutic approaches for IC are mainly formulated based on risk factors identification, early diagnostic testing or the definitive diagnosis. As such, patients might receive antifungal agents as prophylaxis, preemptive, empirical or targeted therapy. Figure 1 illustrates a simple scheme for these approaches.
31,46,47
Management strategies for invasive candidiasis. In critically ill and high-risk patients, early initiation of antifungal therapy is shown to reduce mortality. Courtesy of Zaragoza R and Peman J, 2008, subject to creative commons license.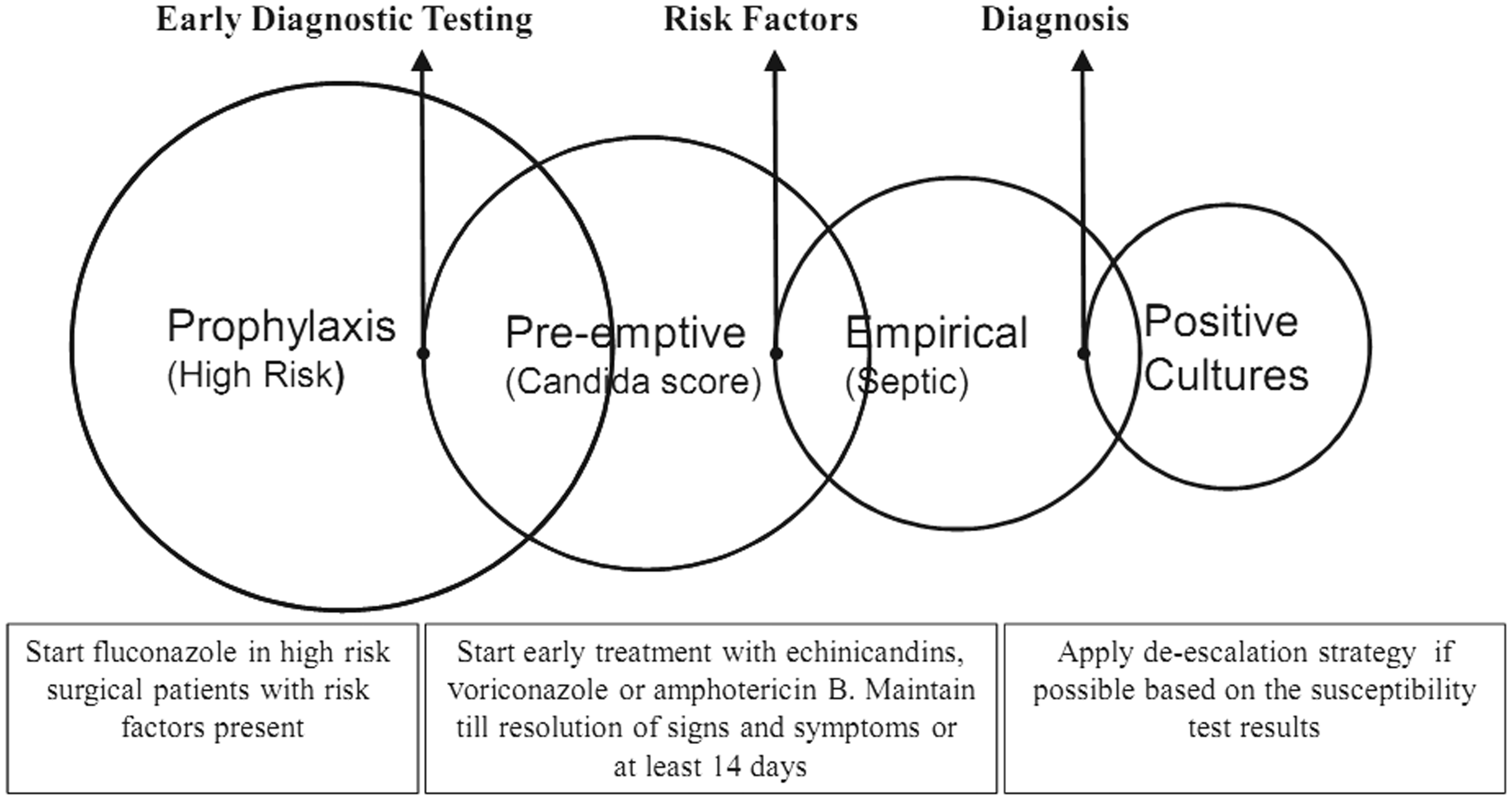
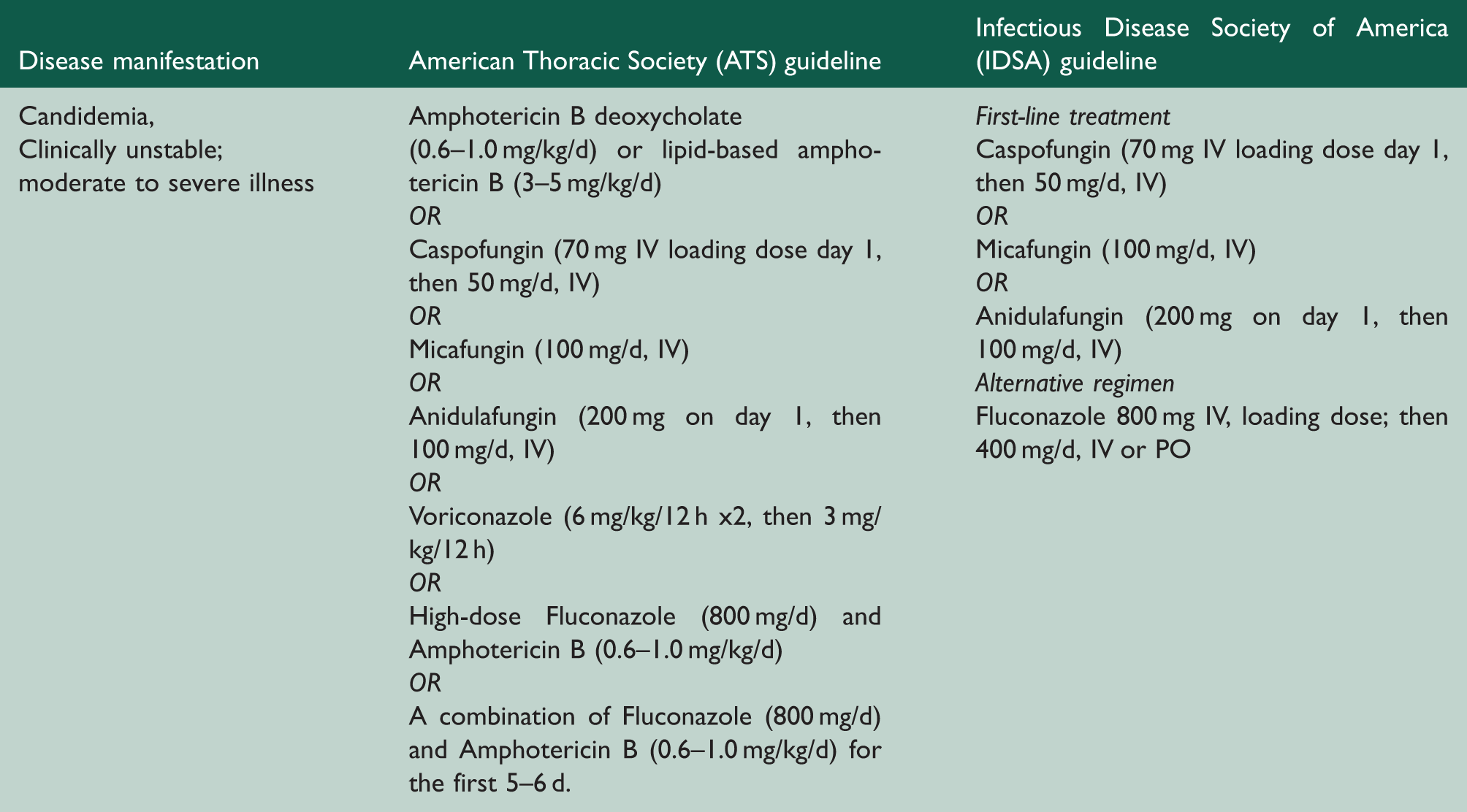
Summary of the ATS and IDSA guidelines for treating invasive candidiasis in critically ill patients.
Recent outcome prediction studies have indicated adverse outcome predictors such as ICU length of stay, renal insufficiency, thrombocytopenia, hematological malignancies, need for mechanical ventilation, needs for inotropic support, APACHE II (Acute Physiology and Chronic Health Evaluation II) score of >20 at the time of candidemia, inadequate empiric antibiotic treatment and delay in starting antifungal therapy. 3,31,49
Taken together, since delayed treatment leads to an unacceptably high mortality with a significant human and economic burden, 31 prompt diagnosis and management should be sought. Application of the validated scoring systems such as Candida Score 44 and Ostrosky-Zeichner model 5,10,45 in ICU will help clinicians to identify the high-risk patients who substantially benefit from prompt treatment against IC. Meanwhile, utilizing the evolving diagnostic strategies and modalities as well as the expanding antifungal armamentarium can be justified through continuous research in the field.
Literature review, participants and the consensus method
To gather evidence, we started from a literature review on the management strategies for IFIs in critical care setting. To do so, databases including MEDLINE (PubMed), Scopus and Google Scholar were searched and relevant papers together with the most recent international practice guidelines on the management of IC in ICU were retrieved and circulated amongst invited panelists. All contributors had reviewed the resources before attending this experts’ input forum.
The panel comprised 17 experts (intensive care and infectious diseases specialists) from different medical care centres and universities in Tehran, Iran. Each was invited based on his/her expertise in the management of IC and other fungal infections in critical care setting. Following plenary talks, interactive discussion and review of literature, three pivotal and commonly asked questions were dealt with. Audience responses and supporting evidence were put together to consolidate point-to-point agreement. For most instances, the expert panel could draw an agreed-upon pathway. One of the authors consolidated the experts’ comments and later, circulated the decision checklist amongst the panelists for endorsement. The clinical algorithmic approach which was agreed by the panel to be followed for the management of IC in the critical care setting (as detailed in the result section of the current report) is summarized in Figure 2.
The algorithmic approach for the management of invasive candidiasis in critical care setting, agreed upon by the Iranian ICU panel of experts. For referencing and further justifications please see the results section. IC: invasive candidiasis; AmB: Amphotericin B; LAmB: Liposomal Amphotericin B; PCR: polymerase chain reaction; 1,3-BG: 1,3-beta-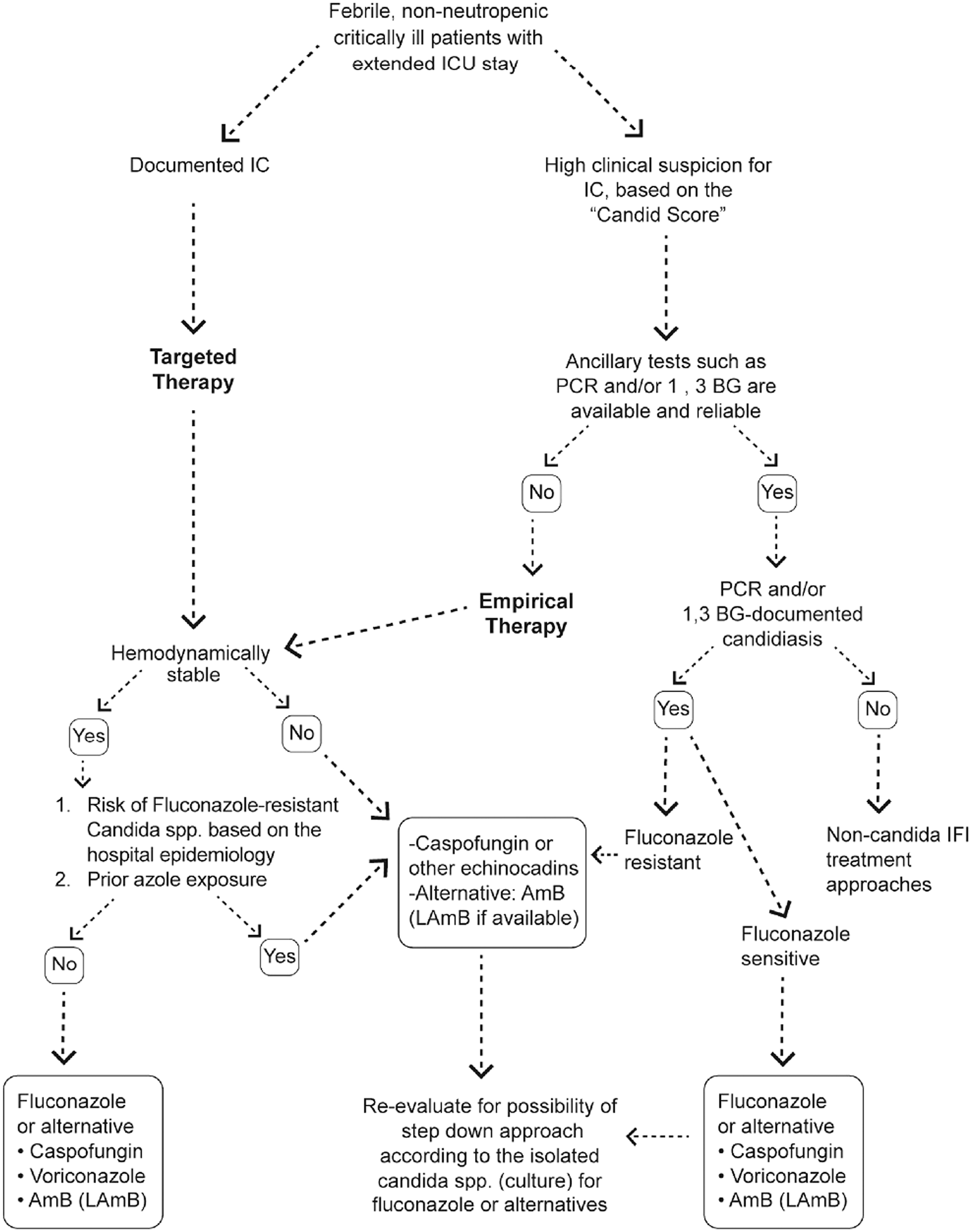
The manuscript generated from this experts’ meeting was distributed, reviewed and edited by all participants. The current expert opinion report as well as future local recommendation documents on the management of IC in critically ill patients (on the basis of the present consensus) will be formulated as a local recommendation and is expected to be implemented across the country following necessary endorsements from national health authorities and the allied scientific societies.
Results
How to diagnose IC?
Discussion
Since the local epidemiological data on fungal infections in ICU are still lacking, our perspective of the incidence and the impact of IFIs in our ICUs should be further clarified in future investigations. The IC scoring systems and predictive models are not used commonly in our setting and many clinicians seem not to be conversant with these tools. Some believe that due to the relatively low sensitivity of such scoring systems and risk prediction models and the high number needed to treat, ancillary testing such as 1,3-BG and PCR should be utilized instead. On the other hand, many others rely more on the significance of clinical suspicion and the value of Candida Score as one of the most applicable tools for high-risk patient selection.
As such, when ancillary tests are neither available nor reliable, the use of risk prediction models and scoring tools such as ‘Candida Score’ would distinguish patients who are at markedly increased risk for IC. The appropriate treatment can then be empirically administered.
Responses
Majority (13/17) of the panel agreed that due to the lack of availability and reliability (lab-to-lab variation) of such tests, although they are good to have, clinicians should depend on their clinical suspicion and proceed to empirical antifungal therapy against IC. This applies to critically ill patients or those characterized as high risk for IC, based on the available validated scoring systems namely the Candida Score. At the same time, more precise and guideline-oriented clinical evaluations should be implemented to curb the overuse of antifungal agents in the critical care setting.
Introducing these clinical scoring systems to less experienced physicians in the field and increasing their awareness about the use and misuse of antifungals based on the current evidence will be crucial. The ancillary investigations such as PCR and 1,3-BG can also be considered based on their availability, reliability (reference labs) and cost-utility justification (Figure 2).
When to start therapy? The prophylactic, preemptive and empirical approaches
Discussion
The concept of preemptive and empirical therapy could overlap in many situations. When we intend to empirically treat IC in non-neutropenic and non-transplanted patients, some key issues such as how early is early and how long to continue treatment should be made as clear as possible. In an ICU-admitted patient who continues to exhibit signs of systemic inflammatory response following 4–7 days of ICU stay with appropriate and adequate antibiotic therapy, institution of empirical antifungals for IC is warranted. It also holds true for patients just admitted to ICU or transferred from another facility with his/her clinical state over the past 4–7 days prior to ICU transfer consistent with ongoing infection. This discretion however depends on the clinical judgment of the treating physician. 4,35
Other than the empirical approach, some non-neutropenic patients are appropriate candidates for prophylactic antifungal therapy. A patient with major abdominal surgery admitted to ICU is a typical example. 4
Time to start antifungal therapy for high-risk patients is the crucial point with a significant value in patients’ outcome. 31 In a high-risk and critically ill patient, empirical therapy for IC is not only an essential component of the immediate management but also is part of care continuity. When culture results become available and a distinct strain is recovered, the treatment regimen can be adjusted. 20
The duration of empirical antifungal therapy should be at least 14 days (14 days since the beginning of therapy or 14 days following a negative culture result). 34,35
Responses
All the experts (17/17) agreed that timely treatment against IC in potentially high-risk patients is crucial. When a patient acquires the score of more than 2.5 in Candida Score and stays for over 4–7 days in ICU, empirical therapy should be strongly encouraged. Treatment should continue for at least 14 days (Figure 2).
What treatment options to use? The question of susceptibility, availability and cost versus utility
Discussion
Considering the availability of the treatment options, we should be able to follow the algorithmic approach laid down by the international guidelines. The decisions should however be adjusted and individualized based on specific limitations such as the availability of the treatment options, cost-utility rationale and tolerability of the given regimen in distinct patients. When high-risk patients for IC are stable and the disease is not severe, patients should be treated with fluconazole if not recently exposed to azoles. In case of prior azole exposure or presumed infection with C. glabrata or C. krusei, echinicandins (caspofungin which is the only echinicandin currently available in Iran) will be the antifungal of choice. 35
In case the patient who is at risk for IC is critically ill and hemodynamically unstable, caspofungin is the first-line therapy. Although ESCMID guideline 34 has recommended not to use AmB for any indication in these population due to its potential side effects, it should still be an alternative modality against IC when other therapies are not available or poorly tolerated. Local studies are needed to evaluate the cost versus utility of the above therapeutic options against IC in ICU.
Responses
A majority of the panelists (15/17) agreed that empirical therapy is indicated in some subset of ICU patients including those with unexplained sepsis. The decision depends on the candida colonization (at multiple sites) and some other risk factors in the absence of any explained cause for fever. Given the correlation between delay in initiation of anti-fungal therapy and mortality in IC patients, everyone agreed that the most effective antifungal agent (as defined by the guidelines) should be employed empirically. Caspofungin, L-AmB and Fluconazole are in turn the mostly recommended antifungals for the empirical therapy against IC in ICU 38 (Figure 2).
Conclusive remarks
All panelists participating in the experts’ meeting for the management of IC in critical care setting were in consensus on the need to promptly identify and manage high-risk patients for IC in ICU. Risk stratification, clinical discretion and the use of validated scoring systems such as the Candida Score are the key to choosing the right patients for empirical antifungal therapy against IC.
International guideline clauses seem to be partly applicable to our local practice. Although there were swings away from AmB in such guidelines, it still should remain in the armamentarium of IC management in our ICU practice. Treatment strategies can be modified on a case by case basis depending on recent azole exposure, severity of the underlying illness and the extent of infection.