
Abstract
Objectives
To record the current use of tranexamic acid during traumatic haemorrhage and elective arthroplasty of the hip and knee.
Design
A questionnaire-based postal survey.
Setting
The questionnaire was sent to the ‘anaesthetic lead’ at all acute trusts in England, excluding centres for children, women’s health, cancer and cardiac care.
Participants
Ninety-nine (66%) centres replied to the questionnaire.
Main outcome measures
Is tranexamic acid used as part of routine standardized treatment for traumatic haemorrhage and for elective hip and knee arthroplasty, and if so what dosage regime was administered?
Results
Few trusts (31%) use tranexamic acid during traumatic haemorrhage, with various dosages used. Its use in hip and knee arthroplasty was also low (38%) with a diverse range of doses prescribed.
Conclusions
Despite many trials showing its efficacy and low risk of side effect, it is clear that its use is not part of standard practice in most centres. Further studies could clarify these concerns and provide a definitive dosing schedule improving patient care and saving lives.
Introduction
Tranexamic acid has been used for many decades to reduce bleeding. It is an inexpensive, easily used, and relatively safe drug. In 1970, the British Medical Journal published results of a trial 1 showing that the use of tranexamic acid significantly decreased menstrual blood loss in women with menorrhagia. Since then its use has spread throughout the surgical specialties including orthopaedic surgery. In traumatic haemorrhage, its use was investigated by the CRASH-2 trial, 2 which concluded that it could reduce blood loss and may prevent thousands of premature trauma deaths each year. In recent years, several systematic reviews and meta-analyses 3 –6 have evaluated the effect of tranexamic acid upon blood loss and transfusion rates in primary total knee and hip replacements. They demonstrated a statistically significant reduction in total blood loss and blood transfusion requirements. A literature review of tranexamic acid in orthopaedic arthroplasty of the hip and knee found many small trials investigating its use. 7 –11 In these limited studies, there was a wide range of different dosing regimens used, involving patient groups of not more than 100. An online search revealed several enhanced recovery programmes running in orthopaedic departments around the country, advocating the use of tranexamic acid in primary orthopaedic arthroplasty of the hip and knee. 12 –14 Again, these all used different dosage regimens.
The aim of this study was to record the use of tranexamic acid in England during traumatic haemorrhage and elective hip and knee arthroplasty.
Methods
A postal questionnaire was sent to the anaesthetic lead of all acute English trusts, excluding centres for children, women’s health, cancer and cardiac care. The questionnaire asked whether tranexamic acid was used as part of their routine standardized treatment for traumatic haemorrhage and for elective hip and knee arthroplasty, and if so what dosage regime was administered.
Results
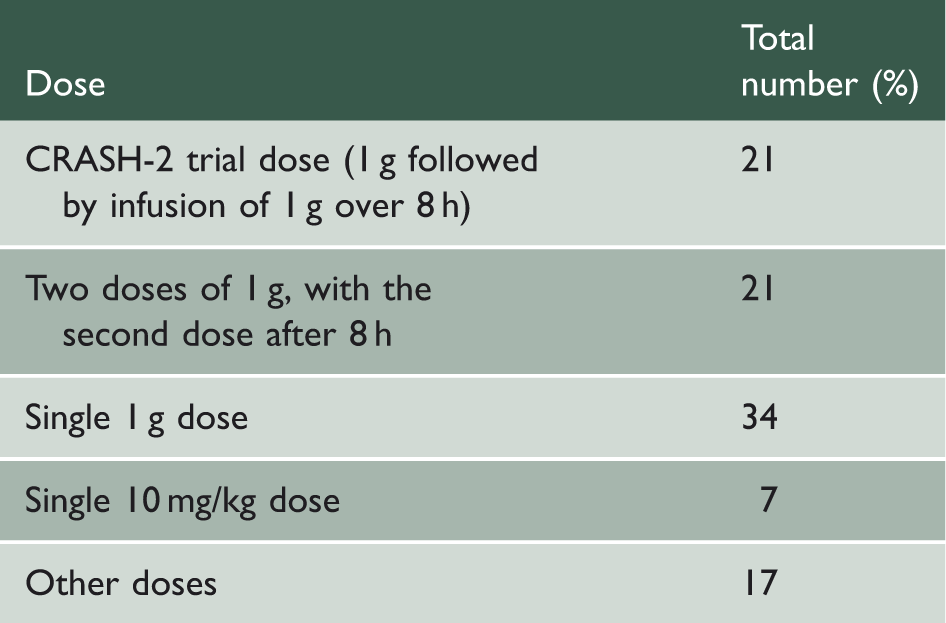
The differing doses prescribed by acute trusts that routinely used tranexamic acid as part of traumatic haemorrhage management.
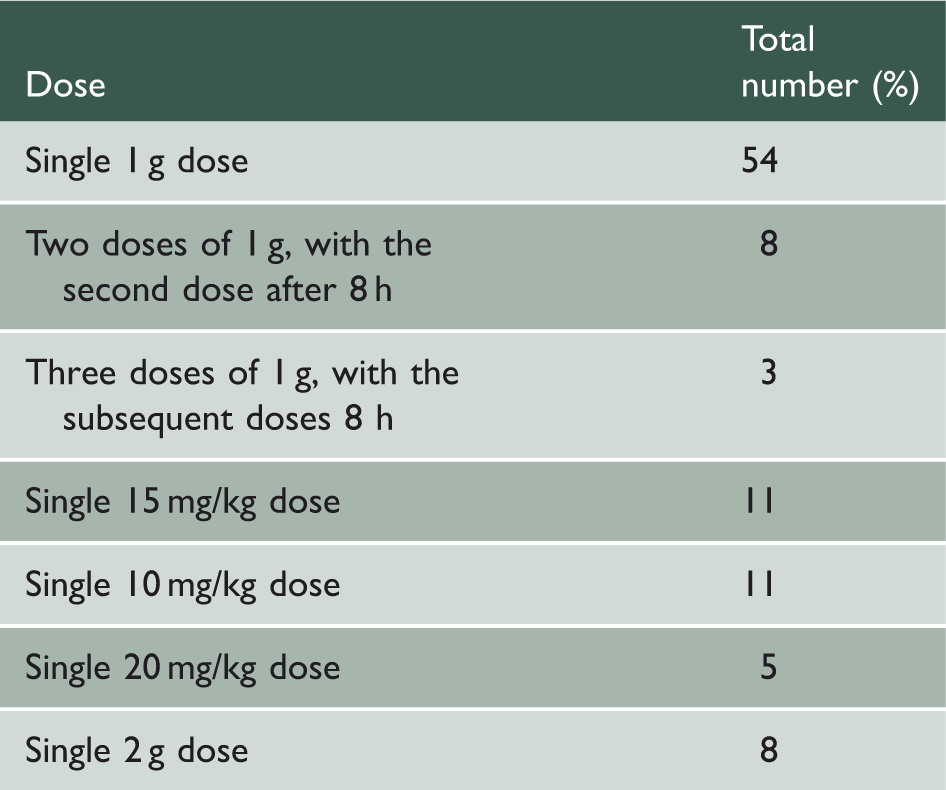
The differing doses prescribed by acute trusts that routinely used tranexamic acid during elective hip and knee arthroplasty.
Discussion
It can be seen from this survey that 69% of trusts that responded do not routinely use tranexamic acid during cases of traumatic haemorrhage. Our results for elective hip and knee arthroplasty show 62% of trusts that responded do not routinely use tranexamic acid. Our survey shows the most common dose given is one dose of 1 g without any postoperative doses, however, a variety of different dosage regimens was observed.
Although the questionnaire was addressed to the ‘anaesthetic lead’ of each acute trust's anaesthetic department, the results may be an underestimate due to its selective use by certain surgeons and anaesthetists. Also, given selectivity bias of a questionnaire, the results may not accurately reflect the precise usage. Nonetheless, it is clear that tranexamic acid is not part of standard practice in most centres.
The CRASH-2 trial established tranexamic acid as an effective hospital-based treatment for traumatic haemorrhage. However, since its publication many questions have been raised; in particular the timing of tranexamic acid, its possible harm if administered late, and its use in a society such as ours where massive transfusion protocols incorporate treatment such as fresh-frozen plasma. Despite this, analysis of the CRASH-2 trial has concluded that tranexamic acid does have a beneficial role if administered within 3 h of injury. 15 This survey also highlighted just how varied the dosage regimens are, even after the large multicentre multinational CRASH-2 trial. Multiple small trials have shown benefit in reducing blood loss for elective hip and knee arthroplasty. 7 –11 Various dosage regimes were used and the optimum dose is unclear. The need for postoperative doses is also unclear.
The low compliance observed with the use of tranexamic acid is likely multifactorial. As well as the uncertainty of the optimum dose and its timing, the low compliance may be due to concerns regarding complications, especially thromboembolism. Numerous studies have analysed the thromboembolic risk and concluded that it is negligible or low. 8,9,11,16,17
Despite many trials showing its efficacy and low risk of side effect, it is clear that its use is not part of standard practice in most centres. A further large randomized multicentre trial could clarify these concerns and provide a definitive dosing schedule and potentially confirm tranexamic acid’s place in protocolized management of arthroplasty and bleeding trauma patients, improving patient care and saving lives.