
Abstract
Objectives
The prevalence of diabetes mellitus is increasing. Previous work has shown that suboptimal glycaemic control is associated with poor perioperative outcomes with increased rates of postoperative morbidity and mortality in several surgical specialities. Recently published UK guidelines have laid out the standards of perioperative care for patients with diabetes. Because an increasing number of patients with diabetes undergo surgery, it is important that these nationally agreed standards of care are adhered to.
Design
A retrospective review of the standard of care of patients against existing audit standards laid down in national guidelines, and a comparison of outcomes with people without diabetes.
Setting
A single major orthopaedic department.
Participants
Fifty consecutive patients undergoing knee arthroplasty between July 2010 and June 2011.
Main outcome measures
Postoperative complications; pre, peri and postoperative glucose control; hospital length of stay.
Results
Although there were no serious postoperative complications, the pre, peri and postoperative management was found to be suboptimal, particularly with reference to optimization of blood glucose control, both in terms of HbA1c preoperatively and blood glucose monitoring perioperatively. The average length of hospital stay was not different between groups; however, 36 patients with diabetes had at least one documented hyperglycaemic episode and four at least one hypoglycaemic episode.
Conclusions
Perioperative care of diabetes in patients undergoing knee arthroplasty could be improved. Several changes have been made since this audit was carried out, in particular adoption of the comprehensive Joint British Diabetes Societies Guideline on the perioperative management of adult patients with diabetes.
Introduction
According to the Association of Public Health Observatories, 3.8 million adults in England and Wales – 8.5% of the population – will have diabetes mellitus by 2020. 1 Their report found the incidence was a 25% increase on previous estimates, and attributed this increase to the advancing age, rising body mass index and changing ethnicity of the population.
The 2013 National Joint Registry Report for England and Wales stated that 84,883 total knee replacements (TKRs) were performed in 2012. 2 It is likely, therefore, that a significant proportion of these patients would have the dual pathology of diabetes and osteoarthritis.
In 2011, NHS Diabetes produced a set of clinical standards for the perioperative period which outlined best practice at an institutional and individual level. 3
The purpose of this study was to assess the performance of a university hospital’s orthopaedic department against these standards.
Methods and materials
A comparison of our findings, compared to the audit standard goals.
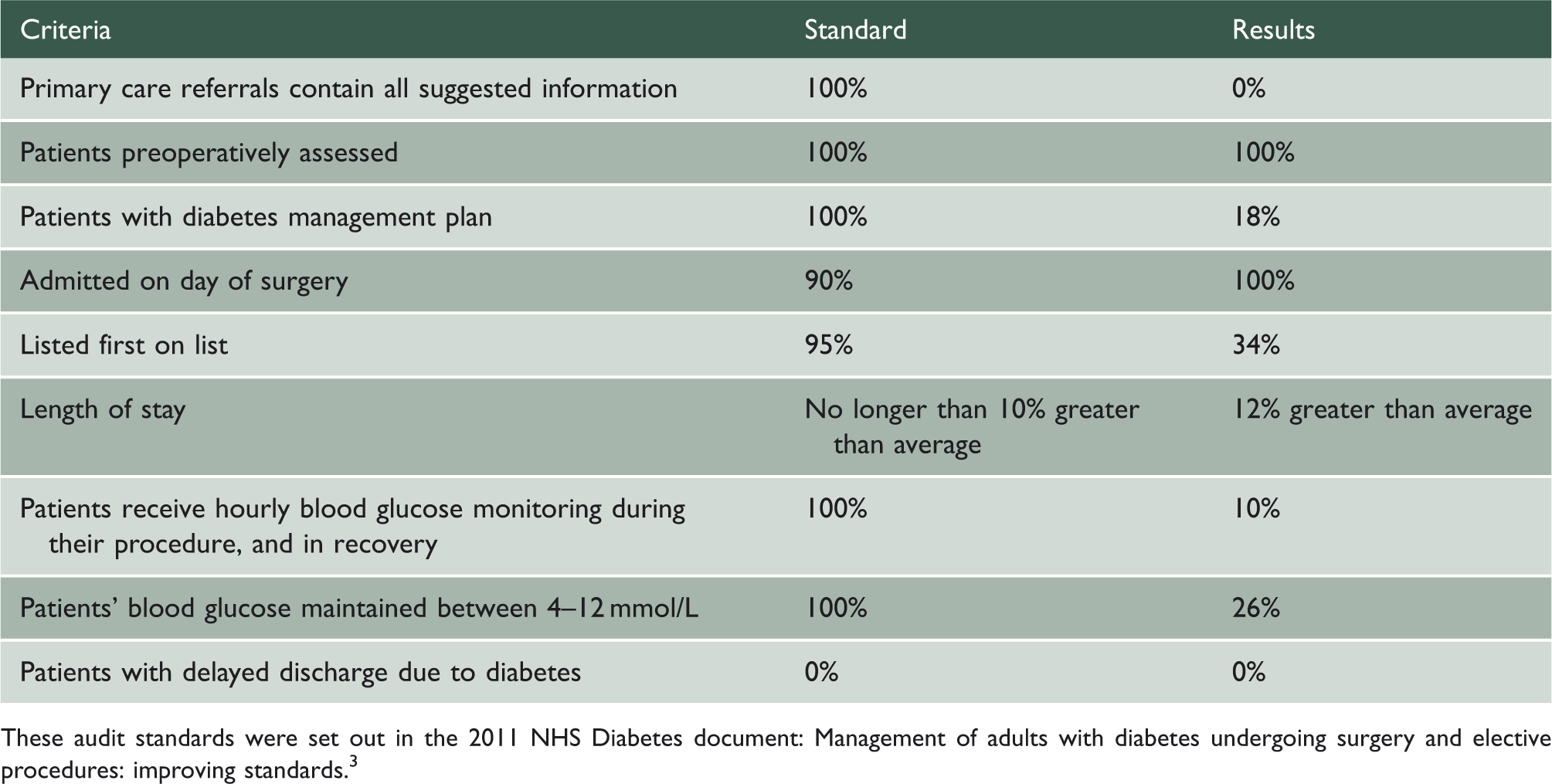
These audit standards were set out in the 2011 NHS Diabetes document: Management of adults with diabetes undergoing surgery and elective procedures: improving standards. 3
The minimum amount of information that Ref. 3 suggests should be included in a standardized GP referral letter to a surgical outpatient for a person with diabetes.

In England and Wales, all of these data (except the most up to date HbA1c within three months of referral) should be collected either as good clinical practice or part of their Quality and Outcomes Framework (QoF).
The length of stay for all patients having a total knee arthroplasty was recorded, and differences between those with and without diabetes measured. Blood glucose measurements during the inpatient stay were reviewed and any postoperative complications were recorded.
Ethical approval was not deemed necessary for this study that was classed as a service improvement exercise.
Comparisons were made between those patients with and without diabetes. Statistical analysis was done using Stata Statistical Software: Release 12 (StataCorp LP, College Station, TX).
Results
Four hundred and eighty-five patients underwent knee arthroplasty between June 2010 and July 2011; of these, 50 were identified as patients with diabetes. Of the patients with diabetes, two patients underwent staged bilateral surgery and only the first side was considered for analysis. There were 33 males, and the mean age of the entire cohort was 72 years (range 50–87). Forty-two patients had a TKR (Genesis 2, PFC Sigma, AGC); four patients a unicompartmental knee replacement (Oxford partial knee replacement); one patient bilateral simultaneous unicompartmental knee replacements; one patient a patello-femoral replacement (Avon). Two patients had revision knee replacements, one of these was a unicompartmental to TKR and the other a cruciate retaining to posterior stabilized TKR.
Forty-nine patients had type 2 diabetes, and a single patient had type 1. Of those with type 2 diabetes, 12 were treated with insulin; 29 were on oral hypoglycaemics only, and eight were diet controlled. Thirty-nine patients had their diabetes managed at their GP; nine patients were under secondary care follow-up, and for two patients it was indeterminate.
The median length of stay was five days for both groups. The interquartile range was 4–7 days for patients without diabetes and 5–7 days for patients with diabetes. These data are shown in Figure 1. The mean length of stay for the unicompartmental knee replacement patients with diabetes was 2.75 days (range 2–5).
Box plot showing length of stay in patients with and without diabetes. There is no significant difference between the two groups. Data are shown as median and interquartile range, with the error bars representing the 25th (lower error bar) and 75th (upper error bar) quartiles.
Six patients had wound-related complications postoperatively although there were no episodes of deep joint infection. As has been previously documented, it can take several years for postoperative complications to become apparent. 4 Three patients had minor cardiac problems postoperatively. Table 1 shows the results as compared to national standards.
No referral letters included a recent HbA1c result. The patients’ blood pressure was stated in 16%; medical history 84%; medications 84%; body mass index 20%; estimated glomerular filtration rate 4%; and the duration of diabetes in 48% of letters.
A recent HbA1c taken in either primary or secondary care was available in 72% of patients. There was no evidence that the three patients with documented levels above 69 mmol/L (8.5%) were referred for further management or had their surgery delayed. In the postoperative period, 36 patients had at least one documented hyperglycaemic episode and four patients had one documented hypoglycaemic event requiring intervention from the nursing staff. The blood glucose levels documented amongst the 36 patients with postoperative hyperglycaemia ranged between 12.9 and 22.2 mmol/L.
Discussion
There is an increasing awareness of the importance of perioperative glycaemic control to prevent postoperative morbidity and mortality. Yet despite this work done to assess the management of patients with diabetes referred for elective surgery, the management remains poor. 5 In this UK study, only 57% of patients with diabetes had their HbA1c checked, and of those only 66% had a level below 64 mmol/mol (8.0%). 5 The key question however is whether diabetes, and in particular, poor glycaemic control leads to a worse outcome post TKR, and if so, does improving glycaemic control change anything. Furthermore, orthopaedic outcome can be assessed in a number of ways: in terms of objective functional outcome or in terms of patient satisfaction. Postoperative complications, particularly the infection rate, range of motion and especially long-term survival of the implant are also of critical importance.
Elevated blood glucose levels pre and postoperatively have been shown to be associated with poor outcomes in surgical patients. 6 The outcomes are worst in those people with hyperglycaemia, but not known to have a previous diagnosis of diabetes. 6,7 In an unselected cohort from a single institution, 30-day mortality was increased by up to two-fold in those people who were known to have diabetes prior to surgery compared with those who had normal glucose values on hospital admission. This compared to an increased 30-day mortality of more than 12-fold for those found to have high glucose prior to surgery who were not known to have diabetes and a greater than 40-fold rise in mortality for those with the highest postoperative glucose levels (>16 mmol/L) without a prior diagnosis of diabetes. 6 Whilst these data were not statistically significant due to the small numbers at these high levels, in agreement with several other studies, the trend strongly suggested an association between mortality and in hospital hyperglycaemia.
With respect to glucose control in the orthopaedic population, the incidence of infection and other poor outcomes in joint arthroplasty has long been thought to be increased in patients with diabetes. 8,9 England et al. 8 found an infection rate of 7% in TKR patients at a mean follow-up of 4.3 years, despite the administration of routine perioperative antibiotics. These authors also quoted a revision rate of 10% in 59 TKRs. The analysis of this paper is difficult when discussing infection rates in people without diabetes. The authors worked out the infection rate from a retrospective cohort of patients with diabetes and then, in their discussion, compared it with the infection rate in the contemporary literature of the time. In addition, they also compared it against a survival analysis paper 10 from their own unit published previously and found a statistically significant difference that way. Neither paper makes any reference to the prevalence of diabetes amongst the comparison groups. Another group found a deep infection rate of 5.3% in a series of 109 TKRs at a minimum follow-up of three years, which they compared with a general TKR population level of 0.5%–2%. 4 In a database study of almost a million arthroplasty patients, diabetes, hypertension and obesity were all found to be independent risk factors for complications and what the authors describe as ‘a non-homebound’ discharge. 11
The functional outcome of TKR patients with type 2 diabetes was assessed by Robertson et al. 12 In a preoperatively functionally matched cohort of 367 patients with diabetes, they had significantly lower maximal flexion, overall range of motion and Knee Society Scores at one- and 10-year follow-up. 12 However, this study had some limitations because the duration of the patients’ diabetes and their overall glycaemic control were not reported.
Previous work has shown that in patients who are post arthroplasty, the Hospital for Special Surgeries knee score is significantly worse for patients with diabetes, as is the Knee Society Score. 13 However, on assessing the long-term outcome and survival of TKRs, this study found a mean rate of aseptic loosening of 7.4% at eight years, which was not significantly higher than the matched group without diabetes. Although the study showed a significantly increased incidence of complications, there was no significant difference in overall implant survival. 13 This finding was contradicted by a later study with a series of 291 patients with diabetes, where they found a significantly higher rate of aseptic loosening at seven years, although again there was no difference in implant survival rates. 14 In this study, pre and postoperative Knee Society Scores were also statistically worse in patients with diabetes.
It is still unclear whether improved control of blood glucose levels will improve outcome. In a database study, perioperative outcome was assessed comparing uncontrolled blood glucose levels, controlled levels and patients without diabetes over a seven-year period. 15 In line with data from other work, 6 this study reported that uncontrolled diabetes was associated with significantly increased rates of stroke, urinary tract infection, ileus, haemorrhage, transfusion, infection and death and, that regardless of the type of diabetes, patients with uncontrolled glucose levels had a higher rate of complications. Another similar database study reported similar findings by assessing perioperative outcomes after total hip and knee arthroplasty. 16 They found patients with diabetes were at increased risk, but also an increased risk of pneumonia but not of joint infection – the lack of a detected increased risk of joint infection was explained by the study focusing on the inpatient perioperative stay, whereas many deep joint infections only become apparent after discharge. 16
HbA1c has been used in other studies to see whether it is a marker for predicting infection risk. 17 One study evaluated 4241 joint replacement patients, 46 infections were identified, 28 of which were serious deep joint infections and 18 superficial infections. Three hundred and fifty of 4241 patients overall had diabetes. Of these 350, 12 developed an infection – a rate of 3.4% in the population with diabetes, compared with 34 infections in the 3891 patients without diabetes (0.87%). It was concluded that patients with diabetes were at significantly higher risk of infection. The mean HbA1c of the infected patients was 55 mmol/mol (7.2%) compared with a mean of 52 mmol/mol (6.9%) in the non-infected patients, leading to the conclusion that HbA1c was not related to infection risk, although the group of infected patients with diabetes was small at only 12 patients. 17 Our study, which reviewed 50 patients with diabetes and focused on their perioperative management, identified that it was suboptimal. It will also provide a basis for a future study assessing long-term outcome.
Conclusion
Our study has shown, in agreement with previous data, that the perioperative care of patients with diabetes is still suboptimal. Poor long-term glycaemic control is likely to be associated with worse clinical outcomes and, in line with the NHS Diabetes national guideline for the perioperative management of patients with diabetes undergoing surgery, it may be prudent to delay surgery until the preoperative HbA1c is under 69 mmol/mol (8.5%).