
Abstract
Objective
To evaluate surgical treatment delay disparities by race/ethnic group in a group of breast cancer patients treated in the New York region.
Design
Cohort study.
Setting
Two affiliated hospitals in the New York region.
Participants
Patients admitted at two affiliated hospitals in the New York region for breast cancer treatment during 2007–2011.
Main outcome measure
Time to receiving first surgery for breast cancer, defined as the time in days between initial diagnosis (biopsy) and definitive surgical treatment (lumpectomy or mastectomy). Predicted time to first surgery by race group was also analysed using a multivariate linear regression model with adjustments made for several demographic and clinical factors.
Results
Totally, 3071 patients who were first treated with surgery were identified. Racial background was classified as White, African American or Asian/other. Overall median time to surgery was 28 days: 28 days in whites, and 34 and 29 days in African Americans and Asian/others, respectively (p = 0.032). Multivariate analyses showed that only African Americans, not Asian/others, had significantly increased surgical delay compared to whites (p = 0.019).
Conclusions
This study demonstrates significant racial differences in surgical delay in a group of breast cancer patients treated in the New York region. These differences may reflect tacit attitudes of medical providers or processes insensitive to patient educational needs. Additional studies may improve our understanding of this delay.
Introduction
Breast cancer is the second most common and second highest mortality cancer in women, and it creates an enormous financial and emotional burden on society. While the United States may have the highest five-year survival rate in comparison to other top developed nations (90% survival rate for breast, cervical and colorectal cancers; 2002–2007), African American women have not equally shared in this benefit, and their mortality rate is 37% higher than their white counterparts.1–4
There have been many reported studies on potential correlation of a range of hypothesised contributing factors to differential mortality, such as race, socioeconomic status, environmental factors, treatment quality and timeliness and disease characteristics.5,6 However, two recent studies and several recent meta-analyses have isolated race as a stronger predictor variable.7–11
In the first stage of the breast cancer care continuum (Figure 1), a significant differential delay in time from symptom recognition (mammogram or self-examination) to initial visit (diagnostic delay) was identified and linked to mortality since different racial/ethnic groups seek medical care from different medical atmospheres.
12
Breast cancer care continuum.
In an examination of the breast cancer care continuum shown in Figure 1, there are treatment disparities. A few reports have studied disparities in surgical intervention timing.6,13 It has been demonstrated that although most women received surgery within three months, 22% of African American women compared to 14% of white women experienced delays greater than three months. These differences remained even after adjusting for access to care and poverty index. 14 Similarly, it was reported that African American women were less likely to have begun treatment less than 30 days from diagnosis. 6 It was also observed that African American women were four to five times more likely to have a treatment delay of more than 30 days. 15 Compared to other racial groups, African American women are more likely to suffer post-operative complications. 16 In addition, there are disparities in treatment quality. Data on 861 patients from the National Cancer Institute Black-White Cancer Survival Study identified 21% of African American women compared to 15% of white women who did not receive basic minimum treatment as recommended by National Institutes of Health (NIH). Furthermore, 36% of patients with late stage disease compared to 4% with early stage disease failed to receive minimum recommended treatment. 17 This treatment disparity further compounds the race disparities because African American women are disproportionately represented in late stage diagnosis. African American women were overrepresented among patients who missed appointments and presented with advanced stage, and the effect of race on survival was still present after adjusting for those factors. 18
Clearly, there seem to be multiple factors that cause racial disparities in breast cancer mortality. Data reported on treatment delays reveal that timeliness of care is a critical factor in improving outcomes. This study augments the existing statistical data on race-based disparities in surgical/treatment delay for African American women with breast cancer. It is the first study to move beyond measures of surgical/treatment delays and to further analyse contributing factors through multivariate analysis including race, age at diagnosis, year of diagnosis, stage of cancer as classified by the American Joint Committee on Cancer (AJCC), surgery type, insurance status and co-morbidities. While study of access to care is confounded by cultural, environmental, or regional variation, this research aims to identify the comprehensive nature of and potential remedy for surgical treatment delay.
Methods
All patients undergoing initial surgical breast cancer treatment from 2007 to 2011 were evaluated. All the treatments were performed at two large affiliated teaching hospitals in the metropolitan New York region that provide comprehensive cancer services and have shared guidelines. Patients who received neoadjuvant chemotherapy or radiation therapy were excluded. After obtaining institutional review board approval, data from the two hospitals’ tumour registries were obtained and information on several demographic and clinical factors, including cancer and non-cancer related data were gathered. These data included age at diagnosis, year of diagnosis (2007–2011), AJCC stage, type of surgery, hospital, number of co-morbidities and insurance status. Data on race were gathered and racial background was classified as White, African American or Asian/other. Time to receiving first surgery or surgical delay was defined as the time in days between diagnosis (biopsy) and definitive surgical treatment (lumpectomy or mastectomy).
Statistical analysis
Initial analyses were based on unadjusted comparisons between racial/ethnic groups in terms of demographic and clinical factors using the chi-square test for categorical variables and one-way analysis of variance for continuous variables. Median time to receiving first surgery or surgical delay was compared in the three racial/ethnic groups using the non-parametric Kruskal–Wallis test. A multivariate linear regression model was employed to predict the time to receiving first surgery for each group.
Adjustments were made for several patient demographic and clinical factors, including age (per 10-year period), diagnosis year, AJCC stage (with stage 0 or 1 vs. stage 2 or stage 3+), type of surgery (mastectomy vs. lumpectomy), hospital, number of co-morbidities (1+ vs. 0), insurance status and year of diagnosis. Each of these variables and implicit hypotheses related to each were distilled from the literature. Recognition of a valuable opportunity to measure surgical delay precisely from a regional registry of cases provided a unique opportunity for analysis. Through regression analysis, this set of variables was analysed in order to further understand the nature and source of surgical delay and its relationship to race and other demographic and clinical characteristics of women with breast carcinoma. Statistical significance was considered at p < 0.05. All statistical analyses were performed using MINITAB 14.0 (MINITAB® Release 14.1. Minitab Inc).
Results
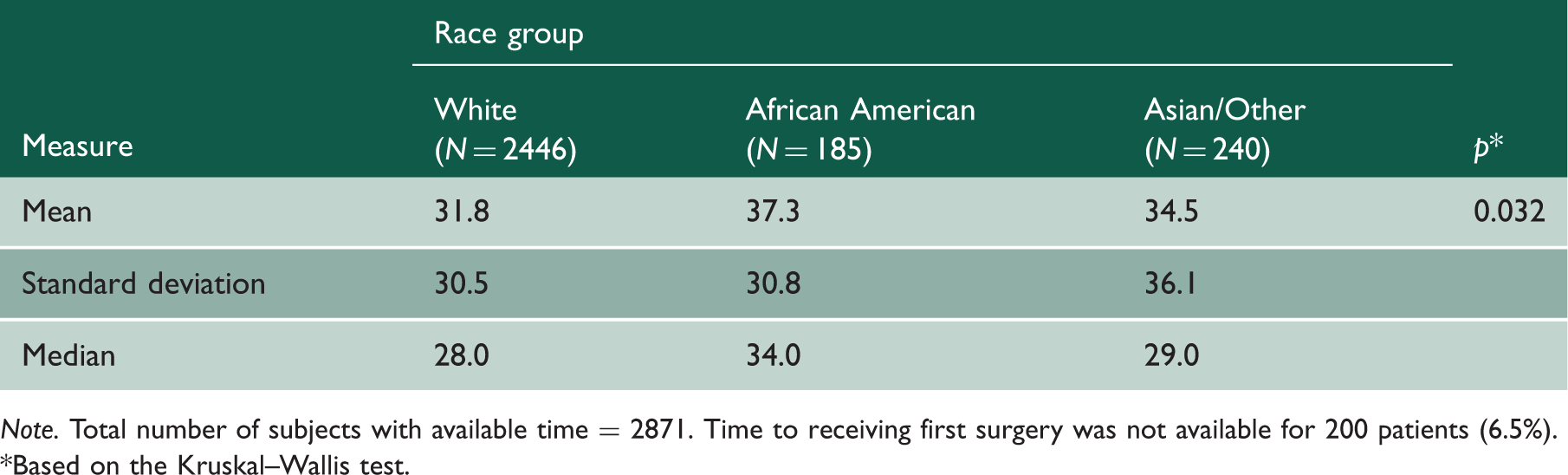
A total of 3237 patients undergoing initial surgical breast cancer treatment from 2007 to 2011 were evaluated. Among the sample patients, 166 patients (5%) received neoadjuvant chemotherapy or radiation therapy and were thus excluded. The final study population consisted of 3071 patients. Average age at diagnosis in the study population was 59.2 years (SD = 13.0). Results from comparing the three race groups in terms of demographic and clinical characteristics are shown in Table 1. The three race groups were significantly different in terms of age at diagnosis, insurance status, diagnosis year and surgical type (p < 0.05). Indication for having at least one co-morbid condition was marginally different in the three race groups (p = 0.055). Table 2 shows descriptive statistics and comparison of time to receiving first surgical treatment for breast cancer in the three race groups. Time to receiving first surgery was not available for 200 patients (6.5%). Median time to first surgery or surgical delay was significantly different in the three groups: 28 days in whites vs. 34 and 29 days in African Americans and Asian/others, respectively (p = 0.032, by the Kruskal–Wallis test). The distribution of surgical delay by race group is shown in the Box-and-Whisker plots in Figure 2. The boxes show the 25th, 50th (median) and 75th percentiles, and whiskers show the minimum and maximum times that are not outliers or extreme values. The figure clearly demonstrates longer surgical delay for African Americans compared to whites, while the difference was clearly less pronounced for Asian/others compared to whites. Multivariate linear regression analysis was conducted on the range of variables that were hypothesised to demonstrate a relation to surgical delay. Results from fitting the multivariate model for time to receiving first surgical treatment are shown in Table 3. The results show that the Asian/other group did not differ significantly from white women (p = 0.54) while African American women had significantly longer surgical delay compared to white women (p = 0.019). Surgical delay also significantly increased with higher AJCC stage (shorter predicted time to surgery for stage 0 or stage 1 patients compared to stage 2 or stage 3+ patients; p = 0.016). Patients undergoing mastectomy (37%) vs. lumpectomy also had significantly increased delay (p = 0.004). In addition, there was a significantly increased surgical delay with more recent year of diagnosis (shorter predicted time to surgery in 2007 and 2008 vs. 2011; p < 0.001 and p = 0.002, respectively). There was a trend toward longer surgical delay with older age at diagnosis (p = 0.082) and lack of insurance (insured patients had shorter predicted time to surgery; p = 0.075). While 51% of patients had at least one co-morbidity, no significant impact was observed for the number of co-morbidities on surgical delay (p = 0.11).
Box-and-Whisker plots for time to receiving first surgery by race group. Total number of subjects with available time = 2871. Comparison between race groups in terms of demographic and clinical factors. Note. 73 patients (2%) had missing information on AJCC stage, 167 patients (5%) had missing information on surgery type. AJCC: American Joint Committee on Cancer. *Based on the chi-square test or one-way analysis of variance. Descriptive statistics for time to receiving first surgery by race group. Note. Total number of subjects with available time = 2871. Time to receiving first surgery was not available for 200 patients (6.5%). *Based on the Kruskal–Wallis test. Multivariate linear regression model for time to receiving first surgery. Note. Total number of subjects with available time = 2871. Time to receiving first surgery was not available for 200 patients (6.5%). A natural logarithmic transformation was applied to the response variable (time) in order to approximate a Gaussian distribution. Model also adjusted for a missingness indicator for AJCC stage (2% missing). AJCC: American Joint Committee on Cancer.


Discussion
This study demonstrates that African American women had significantly increased delay in receiving surgical treatment for breast cancer compared to white women. Multiple studies have reported a significant difference in mortality and other outcomes (process or clinical) for African American women with breast cancer versus white women.2–4 The unadjusted difference in treatment delay demonstrated in this study underscores and echoes previous studies of race-based disparity in diagnostic, treatment or adjuvant therapy delay in breast cancer care.6,19 This may be partially explained and remedied by improved understanding of delays in specific segments of the continuum of care. It is important to explore the ‘empirical’ factors that may contribute to surgical delay for African American women with breast carcinoma and seek out clues to understand the nature of this specific delay. Previous epidemiological studies have demonstrated linkages between race and mortality and between surgical delay and mortality but have suffered from variable definitions of race, socioeconomic status, access to care and tumour biologics, constraining efforts to identify specific factors related to increased mortality for African American women with breast cancer or causes of disparate treatment delay. Additionally, other reports state that breast cancer mortality race disparity is due to difference in breast cancer disease characteristics.20,21 It has been shown that at any stage, African American women have higher pathologic grade and Estrogen Receptor (ER)/Progesterone Receptor (PR) negative disease compared to white women, indicating worse prognostic markers early on.19,22 Data on women with breast cancer in the Greater San Francisco Bay Area between 1988 and 1992 showed that 10-year unadjusted survival rates were 81% for white women, 69% for African American women, 75% for Hispanics and 79% for Asian women. The disease stage-adjusted relative risk for Hispanic and Asian women did not differ significantly from white women, whereas for African American women, it was still significantly higher. 23 Worse disease characteristics most presumably in the race’s genetics seem to be another factor in race mortality disparities.
The trend for longer surgical treatment delay with older age reported in this study is not surprising. This age-related differential in treatment delay may be due to life-long attitudes or economic and cultural barriers to care, and to other extrinsic factors that could contribute to the observed delay at each stage of the breast cancer care continuum.
In a parallel result, higher AJCC stage at diagnosis was related to treatment delay. Increased severity as indicated by tumour stage might be expected to reduce delayed treatment in order to improve prognosis. However, that was not the case in this analysis, again pointing to extrinsic variables and their impact on timely access.
The significant difference in surgery type (mastectomy versus lumpectomy) in relation to surgical delay may be explained by a number of factors, including patient reluctance to choose mastectomy for aesthetic or other reasons or factors related to the differences in process complexity or treatment scheduling. The fact that insurance status was not significantly related to treatment delay may reflect the quality of care or shared guidelines in the two affiliated facilities and/or generally low barriers to care in the regional population.
The significant increase in surgical delay for more recent years of diagnosis may be due to administration of additional tests, e.g. magnetic resonance imaging (MRI), bone density and other tests that are more commonly done before surgical treatment in more recent years.
The strength of this study is its methodological contribution and reinforcement of the previously demonstrated relationship between race and time to receiving first surgical treatment for breast cancer as it further analyses a set of hypothesised factors related to that delay. Other variables of note that might have been studied include educational status, missed appointments and other factors from the literature that may be linked specifically to surgical delay.
A significant limitation of this study is the unevenly dispersed study population in terms of race: 85% white, 7% African American and about 8% Asian, Hispanic and Other. We sought to examine the length of surgical delays mainly between African Americans and white patients. It is known that the sociological composition of the area surrounding the two hospitals is a fairly affluent suburban neighbourhood that is predominately white. The proportion of Asians, Hispanics, Latinos, Alaskan Indian, etc. who underwent treatment was relatively small. Preliminary analysis showed that surgical delay was not statistically different for Hispanics, Latinos, Asians and other non-African American minority groups (median = 29 days for all of those groups; p = 0.93) and thus were grouped together into one single category, Asian/other. Also, it is possible that Asians, Hispanics, and others are more likely to seek alternative remedies for treatment rather than in the US medical system possibly due to cultural issues, language barriers and affordability. 24
Conclusions
This study demonstrates significant racial differences in surgical delay for a regional population of women with breast carcinoma receiving surgery from 2007 to 2011. In the context of previous studies of disparate morbidity and mortality for African American women with breast cancer, this study provides an example of a differential contributing factor or related variable that may help to disaggregate the many hypothesised factors contributing to disparate outcomes by focusing specifically on treatment delay and its potential remedy as a measurable focus of process improvement. In trying to understand these findings, a speculative picture emerges of delay across the continuum and of surgical delay specifically. For many patients, a breast cancer diagnosis may be their first encounter with serious illness and the complex delivery system. Surgical delay may specifically be affected by historical perceptions of cancer, where surgery is considered as the beginning of an inevitable decline ending in death. Asians and Hispanics as with some African Americans have been found to have less faith in their medical care providers and thus may be more reluctant in undergoing surgical treatment than whites. These differences may reflect tacit attitudes of medical providers or processes insensitive to patient educational needs. Further qualitative studies may enhance our understanding of this delay.
While other studies have focused on variations in mortality and morbidity by racial groups, this study takes important steps toward a better understanding of the factors related to delay in receiving surgical treatment for breast cancer. Further studies may include examining the trends of breast cancer mortality and surgical delays among newer minority groups (including immigrants) and identifying the trends of which groups are more likely to seek treatment taking into account socioeconomic status.