
Abstract
Objectives
To estimate the frequency of symptoms of obesity hypoventilation syndrome (OHS) in patients with obstructive sleep apnoea (OSA) and to evaluate comorbidities associated with OHS.
Design
Retrospective study based on patients' medical records and on further sleep tests performed in the study centre during the inclusion visit.
Setting
Respiratory Care Unit and Sleep Disorder Centre of the Zayed Military Hospital United Arab Emirates.
Participants
All patients referred to the study centre for a suspicion of sleep-disordered breathing.
Main outcome measures
Prevalence of OSA and OSA + OHS and comorbidities in patients with OSA and OHS.
Results
A total of 212 adult patients participated in the study. Of these, 107 patients (50.5% [43.8–57.1% CI 95%]) fulfilled diagnostic criteria for OSA, and the majority were men (79.4%). Among patients with OSA, 18 patients (16.8% [10.8–25.1% CI 95%]) fulfilled diagnostic criteria for OHS. In this group, women were more frequently affected than men (31.8% [7/22] vs. 12.9% [11/85], respectively; p = 0.03) and tended to be older than affected men, with a mean age of 55 ± 10.6 years versus 46 ± 13 for men. After adjustment for gender, OHS was significantly associated with hypertension (OR = 3.5; p = 0.03), diabetes mellitus (OR = 4.6; p = 0.02), ischaemic heart disease (OR = 5.1; p = 0.04) and pulmonary hypertension (OR = 16.1; p = 0.001).
Conclusion
OHS is a common condition in obese patients in the UAE and is associated with an increased risk of cardiovascular comorbidities and diabetes.
Keywords
Introduction
Over the last decades, the prevalence of obesity, diabetes and related diseases has increased in the Gulf region as the consequence of the substantial economic growth of this region which has led to sedentarization and major changes in diet and lifestyle. Obesity (body mass index [BMI] ≥ 30 kg/m2) now affects around one-third of the adult population of this region. 1 For example, in the UAE, it has been reported that 32.7% of adults and 12.1% of adolescents (10–19 years) were obese. An even higher prevalence rate was reported in Kuwait (42.1% of adults). 1 With respect to gender, obesity is more frequent in women than in men (39.6% vs. 30.0%). 1
Obesity is associated with many other medical conditions including sleep-disordered breathing. The role of obesity as a risk factor for the development of obstructive sleep apnoea (OSA) is well established. 2 For example, two studies performed in South America reported that over 80% of morbidly obese patients had OSA.2,3 In addition, a recent study performed in primary care in the UK in adults older than 50 years reported that subjects with a BMI of 40 kg/m2or over were 27.39 times (95% CI 24.64–30.46) more likely to have OSA (p < 0.0001). 4 Male gender and increasing age are also considered as risk factors for OSA. 5 OSA is one of the most common sleep disorders which can occur on a similar incidence to that of type II diabetes and twice than that of asthma. 6 In the UAE, the prevalence of OSA in the adult population has been estimated to be around 7%. 6
Another sleep-disordered breathing condition related to obesity is obesity hypoventilation syndrome (OHS) or Pickwickian syndrome. This condition is characterized by the presence of hypoventilation while awake and is defined as the presence of obesity (BMI ≥ 30 kg/m2) associated with daytime hypercapnia (pCO2 > 45 mmHg) in the absence of other causes of hypoventilation. 7 This syndrome is distinguished from classical OSA, in which patients have normal alveolar ventilation when awake, although the two conditions may frequently overlap. It has been reported that patients with OSA have a higher mortality rate than those similarly obese patients without OHS (23% vs. 9%; hazard ratio: 4.0).8,9
The prevalence of OHS in the general population is very poorly documented. A study performed in the USA estimated the prevalence of OHS in the general population to be between 0.15 and 0.30%. 10 Another study in the USA performed in patients with OSA estimated the prevalence of OHS in this population to be between 10 and 20%. 8 To our knowledge, there are no data on the prevalence of OHS in the Middle East either in the general population or in patients with OSA. As obesity is of growing concern in this region,11–13 more information on OHS in the Middle East would clearly be useful. For this reason, we performed a retrospective survey of patients with suspected sleep-related breathing disorders who attended our sleep disorder clinic in the Zayed Military Hospital, an urban tertiary level teaching hospital providing healthcare to the population of UAE. The objective of the study was to estimate the frequency of symptoms of OHS in patients with OSA and to evaluate comorbidities associated with OHS.
Methods
This was a retrospective cross-sectional study performed from March 2008 to June 2009 in the Respiratory Care Unit and Sleep Disorder Centre of the Zayed Military Hospital in UAE. This hospital is one of the largest public hospitals providing tertiary care in the UAE. Its catchment area is the Abu Dhabi region of the UAE and it attracts patients from both urban and rural areas and provides care to both military and civilian patients and to national and foreign residents. The hospital was visited by 651,981 outpatients in 2012.
Study sample
The study population consisted of all patients referred to the centre for the investigation of possible sleep-disordered breathing. These patients were referred from the respiratory clinics, or other specialties such as cardiology, ENT, endocrinology and family medicine or from outside private clinics. Patients aged younger than 18 years were excluded.
Data collection
Data on demographics, clinical symptoms and comorbidities (diabetes mellitus, arterial hypertension, ischaemic heart disease or pulmonary hypertension) were documented from the medical records. Results of spirometry, echocardiography and measurement of arterial blood gases (ABG) 14 were documented from the patient's medical records, as well as the results of evaluations performed during dedicated visits to the internal medicine, cardiology and endocrinology departments.
All patients underwent overnight polysomnography (PSG) using Alice5 (Philips –respironics) with EEG (C3–A2, C4–A1, O1–A2, O2–A1) ROC, LOC, 2 Chin EMG, both legs tibialis anterior EMG for leg movements, continuous ECG and oxygen saturation monitoring. Respiration was monitored by oro-nasal thermister and piezoelectric belts for thoracic and abdominal movements. Transcutaneous CO2 monitoring was performed if the ABG showed hypercapnea.
Polysomnographic data were scored on the basis of standard criteria15,16 by an experienced registered PSG technologist. Sleep-disordered breathing parameters were obtained from the polysomnogram. For each patient, the apnoea-hypopnea index (AHI) was determined as the total number of apnoeas + hypopneas × 60/total sleep time (min). Apnoea was defined as complete cessation of breathing for >10 s. Hypopnoea was defined as a reduction in amplitude of airflow by at least 30% of baseline for duration of at least 10 s accompanied by an oxygen desaturation ≥ 4%. Patients with OSA were defined as those with an AHI > 5/h and those with OHS as having a BMI > 30 kg/m2 and day time hypoventilation with pCO2 > 45 mmHg.
Statistical analysis
For descriptive statistics, data were expressed as mean ± SD, or as percentages for categorical variables. Potential associations between incidence rates for OHS and other categorical variables were evaluated with Fisher's exact test or the Mantel–Haenszel test, as appropriate. The strength of association was expressed in terms of odds ratios (OR).
Results
Study sample
At baseline, a total of 212 patients participated in the study. The mean age was 45.6 ± 13.2 and the majority were men 164 (77.4%). The mean BMI was 33.8 ± 8.9 kg/m2 and over half of the study population (57.1%) was obese (BMI > 30 kg/m2).
Frequency of OSA and OHS
Demographics and patients' characteristics during the admission phase.

Data were collected from the patient's medical records. All data are represented as mean ± SD or number (%). Data on pulmonary function tests (FEV1 and FVC) concerned 60 patients.
BMI: body mass index.
Of the 107 patients with OSA, 18 patients (16.8% [10.8–25.1%; CI 95%]) fulfilled criteria
for OHS according to the definition used. This corresponds to 8.5% [5.4–13.1%; CI 95%] of
the total population involved in the study (Figure 1). The mean BMI in this population was
45.4 ± 13.1 kg/m2 and the mean daytime pCO2 was 57.4 ± 11.69 mmHg.
Prevalence of OSA and OSA + OHS in the population referred to
the sleep centre (n = 212).
Retrospective data of patient with OSA alone and OSA + OHS.

Data on pCO2 were missing for 82 patients.
OHS: obesity hypoventilation syndrome; OSA: obstructive sleep apnoea; BMI: body mass index; AHI: apnoea-hypopnea index.
The occurrence of apnoea or hypopnoea episodes was quite higher in the OSA + OHS group and the median AHI score was >30 events/h reflecting a severe OSA.
Comorbidities
Comorbidities in patients with OSA and OHS.

*The denominator was the total number of men and women with-OHS group, respectively, n = 11 and n = 7.
OHS: obesity hypoventilation syndrome; OSA: obstructive sleep apnoea.
The association between OHS and the presence of comorbibities was analysed using the
Mantel–Haenszel test. The presence of OHS in OSA patients was significantly associated
with all comorbidities documented in the study: hypertension (OR = 3.5; [95% CI: 1.2 –
10.3]; p = 0.03), diabetes mellitus (OR = 4.6; [95% CI: of 1.4 – 15.4];
p = 0.02), ischaemic heart disease (OR = 5.1; [95% CI: 1.2 – 21.3];
p = 0.04) and pulmonary hypertension (OR = 16.1; [95% CI: 3.2 – 82.0];
p = 0.001). The results of this analysis are presented as a Forest plot
in Figure 2. Risk of
selected cardiovascular and diabetes comorbidities in patients with OHS. The
reference group in each case corresponded to patients with OSA who did not fulfill
criteria for OHS. Data are presented in the form of a Forest plot showing odds
ratios with their 95% confidence intervals. Data are adjusted for sex, using the
Mantel–Haenszel test.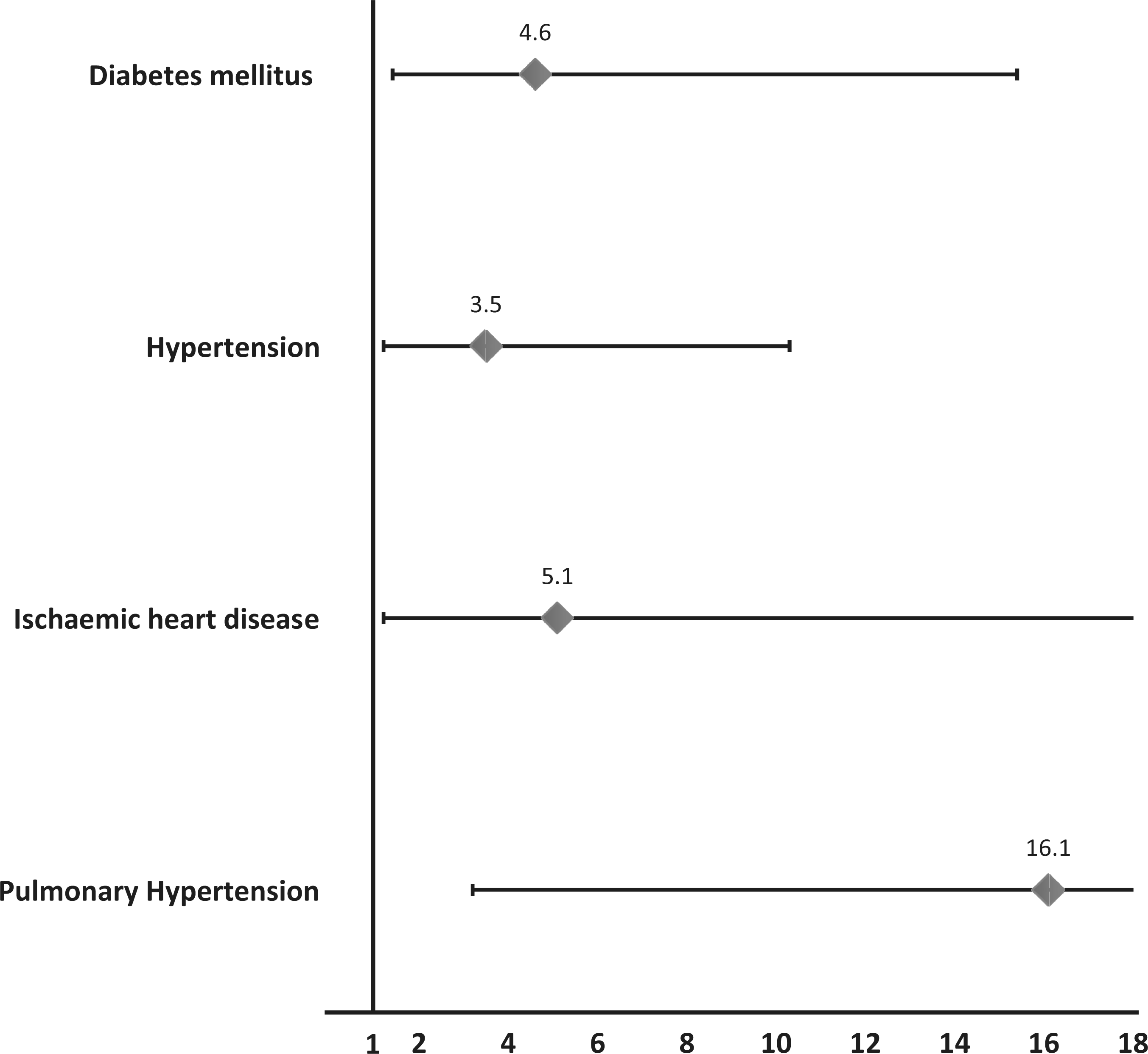
Discussion
This retrospective study was performed in the UAE in adult patients admitted to the Respiratory Care Unit and Sleep Disorder Centre of Zayed Military Hospital for suspicion of sleep-disordered breathing. The primary objective of the study was to estimate the frequency of symptoms of OHS in patients with OSA. In this study, we found that the proportion of patients with OSA referred to the sleep centre who also fulfilled criteria for OHS was 16.8%.
The main limitation of our study is missing data due to the retrospective design of the study, which could have led to incomplete case ascertainment. In addition, the study sample is relatively small and came from a single tertiary care centre in the UAE, albeit a large one. Without a complete description of the hospital's patient base, we are unable to ascertain the representativeness of the sample included, which may not portray accurately the OSA population in the UAE. The results of this study should thus not be generalized to the entire population of the UAE.
The frequency of OHS observed in this study is somewhat lower than those reported from previous prospective and retrospective studies performed in the USA, Western Europe and Japan, which have estimated the prevalence of OHS to be between 10 and 20% of all patients referred to sleep centres and between 20 and 30% of all patients with OSA.15,17 In the Middle East and Gulf region, there are no comparable data and our study is the first to address this issue. Nonetheless, our study may underestimate the true prevalence of OHS in patients with OSA as the study sample represented a pre-selected population referred to the study centre for a suspicion of a sleep-disordered breathing, which may not correspond to those most at risk for OHS. On the other hand, we could overestimate the true prevalence of OHS as we attributed all pCO2 > 45 mmHg measured in obese patients to OHS, whereas in reality some patients may have been hypercapnic due to other conditions such as chronic obstructive pulmonary disease. Prospective studies should be able to avoid this by excluding other comorbidities in patients with hypercapnia by performing thyroid function tests, pulmonary function testing, and chest imaging.
The relationship between OHS and OSA has been investigated in previous studies. For example, in a prospective study performed in France, it was found that in patients with sleep-disordered breathing, there was a strong association between OHS and OSA given that around 90% of patients with OHS have OSA. 18 This result suggests that the association of comorbid OHS and OSA was much more frequent than OHS alone.
Our patients with OSA were predominantly men and obese (BMI > 30 kg/m2), consistent with other studies. 5 In contrast, we did not observe a clear gender difference with respect to OHS which is again consistent with previous studies reporting a similar prevalence of OHS in women and in men. For example, Nowbar et al. 8 showed that around half (48.9%; 23/47 patients) of patients with obesity associated hypoventilation were men. This suggests that risk factors for OHS and possibly OSA may differ between women and men.
The secondary objective of this study was to identify comorbidities associated with OHS. The strong association between OHS, diabetes cardiovascular comorbidities and pulmonary hypertension is consistent with findings from other studies. Nevertheless, the relative weight of these comorbidities is somewhat different to studies performed elsewhere in the world. For example, a prospective study performed in France estimated that 58% of OHS patients have pulmonary hypertension defined as a mean pulmonary artery pressure > 20 mmHg, 18 which is nearly twice that observed in our study (33.3%). However, the limited precision of comorbidity rates due to the small sample size should also be born in mind when interpreting such differences. Incomplete documentation of comorbidities or ethnic differences in vulnerability may also contribute to inconsistencies in reported comorbidity rates between studies.
As in other regions of the world, this study reveals a relatively high proportion of patients with OSA in Abu Dhabi who also present OHS. In light of fast-rising obesity in the Middle East region, the prevalence of OHS is also likely to rise in the near future as obese patients enter the at-risk age bracket. Since this condition is associated with serious life-threatening comorbidities, it is important to build awareness about OHS in healthcare professionals in the UAE and to encourage systematic diagnosis of OHS through systematic measurement of blood gases in subjects who are obese or have OSA. Early diagnosis leading to timely treatment may improve long-term prognosis, especially since access to treatment with positive airway pressure devices is free in the UAE. In addition, patient education programmes to encourage weight loss in obese subjects are clearly important. Further prospectively designed studies would be useful in order to measure the magnitude of the problem at the general population level and to monitor patients' response to therapy.