
Abstract
Objectives
Provision of person-centred generalist care is a core component of quality primary care systems. The World Health Organisation believes that a lack of generalist primary care is contributing to inefficiency, ineffectiveness and inequity in healthcare. In UK primary care, General Practitioners (GPs) are the largest group of practising generalists. Yet GPs fulfil multiple roles and the pressures of delivering these roles along with wider contextual changes create real challenges to generalist practice. Our study aimed to explore GP perceptions of enablers and constraints for expert generalist care, in order to identify what is needed to ensure health systems are designed to support the generalist role.
Design
Qualitative study in General Practice.
Setting
UK primary care.
Main outcome measures
A qualitative study – interviews, surveys and focus groups with GPs and GP trainees. Data collection and analysis was informed by Normalisation Process Theory.
Design and setting
Qualitative study in General Practice. We conducted interviews, surveys and focus groups with GPs and GP trainees based mainly, but not exclusively, in the UK. Data collection and analysis were informed by Normalization Process Theory.
Participants
UK based GPs (interview and surveys); European GP trainees (focus groups).
Results
Our findings highlight key gaps in current training and service design which may limit development and implementation of expert generalist practice (EGP). These include the lack of a consistent and universal understanding of the distinct expertise of EGP, competing priorities inhibiting the delivery of EGP, lack of the consistent development of skills in interpretive practice and a lack of resources for monitoring EGP.
Conclusions
We describe four areas for change: Translating EGP, Priority setting for EGP, Trusting EGP and Identifying the impact of EGP. We outline proposals for work needed in each area to help enhance the expert generalist role.
Introduction
Provision of person-centred generalist care is a recognized core component of quality primary care systems.1,2 The World Health Organisation (WHO) believes that a lack of generalist primary care is contributing to inefficiency, ineffectiveness and inequity in healthcare. 3
Generalism is a professional philosophy of healthcare practice 4 ; described as ‘expertise in whole person medicine’. 5 The ‘expertise’ of generalism relates to an approach to care which is person not disease oriented; taking a continuous rather than an episodic view; integrating biomedical and biographical understanding of illness; to support decisions which recognize health as a resource for living and not an end in itself. 6 In primary care, General Practitioners (GPs) are the largest group of practising generalists. Holistic, or whole person, care lies at the heart of definitions of being a GP 7 and is a core component in the GP curriculum. 8
In the UK, GPs fulfil multiple roles: including delivering community-based care for chronic disease, health promotion, and now commissioning, as well as the person-centred role of the expert generalist. The pressures of delivering multiple roles (an ‘all-rounder view’ of the generalist role) along with wider contextual changes create real challenges 9 to generalist practice, contributing to the concerns raised by the WHO. 3
Particular concern relates to the care of people living with chronic conditions and with multimorbidity.10,11 May et al. 10 argue that a lack of person-centred, rather than condition focused, care is contributing to an excessive burden on patients. Yet much of this care is being delivered in the primary care context – raising questions about whether we lack capacity to deliver person-centred expert generalist primary care for this group of people.
Our study therefore focuses on the delivery of expert generalist care in the primary care context. We set out to answer the question, what factors enable or constrain expert generalist practice (EGP)?
Methods
Theoretical framework: assessing provision of EGP
Generalism is a professional philosophy of practice: 4 described in the seminal texts of authors such as McWhinney and Freeman 12 and accounts of the biopsychosocial approach to consultation. 13 As such, it is deeply engrained 14 in the philosophy and ideals of practice. However, in order to study provision of care, we need to translate rich descriptions of a philosophy of generalism into a framework we can use to study practice.
Accounts of generalism recognize multiple and variable components 5 which both contribute to and arise from person-centred care in different contexts 5 (p.7) (for example, continuity and coordination of care, communication skills and relational care). However, our focus is on the distinct expertise of the generalist: that which is unique to and distinguishes generalist care from other approaches to practice; namely a person, rather than condition, focused approach to making decisions about care needs. 6 It is this that we recognize as EGP. EGP refers to the distinct form through which the philosophy of generalism is operationalized.
From this description, we thus recognize EGP as a complex intervention as described within the Medical Research Council Complex Interventions framework. 15 It has several interacting and variable components (patient, practitioner and context), and a range of possible outcomes. 15 At its core are two distinct or ‘constant components’ (understood as fixed for all practitioners, all patients and every treatment). 16 These are firstly the principle of person-centred decision making which recognizes health as a resource for living and not an end in itself.6,17 Secondly, the practice of interpretive medicine: integrating multiple sources of knowledge (including biomedical, biographical and professional) in a dynamic exploration and interpretation of individual illness experience. 17 Practice leads to decisions about what is wrong, and what is needed to intervene, which support an outcome of health as a resource for living. 18
The NPT-EGP framework – the Normalization Process Theory 19 toolkit adapted to examine the complex intervention that is EGP.

*NPT predicts the need for activity in 16 domains of work, grouped into four categories: Sense making, Engagement, Action and Monitoring.
**Analysis of activity shown as GREEN if necessary work
identified  ; RED if no
activity identified
; RED if no
activity identified  ;
CROSSHATCHING if mixed picture
;
CROSSHATCHING if mixed picture  .
.
Box 1. Describing the three datasets
1. Interviews with practising GPs in
Merseyside (Autumn 2011: JR, FM, CFD, SM, CM,
JG, VP, GF) All GPs on a local peer support group email list
(n=160) were invited to take part in an
interview exploring experiences of delivering generalist
care to people with multimorbidity. Ten GPs replied, one
practice manager also took part. All GPs had completed
specialist training; seven women, three men; three early
career, seven experienced GPs. An interview schedule based
on the modified NPT Toolkit (Table 1) was used
(available from the authors) to explore enablers and
constraints for EGP. JR conducted all
interviews. 2. Survey of attendees at an RCGP Conference
workshop on Generalism (October 2012, JR, GF,
AH) Workshop attendees (approximately 250 people) were all
invited to complete an online survey developed from the
modified NPT toolkit (revised in light of findings from
dataset 1). The Survey monkey link was also circulated in an
RCGP newsletter and participants invited to pass the link on
to interested parties (https://www.surveymonkey.com/s/QCL6R3K).
Ninety-six replies were received, 94 from practising
GPs. 3. Focus groups with International GPs in
training attending RCGP Conference (October
2012, GI, JW, AS, JR) Organized by the Junior International Committee of the
Royal College of General Practitioners, two focus groups
were held with conference delegates to explore international
GP Trainee and First five GPs’ perspectives on expert
generalist practice. Sixteen people attended one of two
groups run by GI, AS and JW. Participants came from
Portugal, Spain, Austria, Poland, Italy, Romania, Denmark
and Israel. The interview schedule was developed from the
survey tool and is available from the
authors.
Sampling and data collection
We collected three datasets (see Box 1).
Analysis
A Framework Analysis approach 24 was used to categorize the data. Transcripts and survey responses were read to identify examples of work related to EGP which fell into the 16 domains identified within the modified NPT framework (Table 1). We categorized activities as ‘enablers’ where they offered examples of the work necessary for integration of EGP in usual care. Where we identified an absence of work, or a contradiction to EGP, we categorized these activities as constraints. JR analysed the full dataset; GI conducted a parallel analysis of the focus groups, VP coded five of the GP interviews. We used a Red/Amber/Green approach to summarize the findings in each of the 16 domains: green if we identified examples of the necessary work (enablers) with no constraints; red if we failed to identify any examples of the necessary work; amber if we saw a mixed picture.
Results
A summary of results across the 16 NPT domains is shown in Table 1, highlighting constraints across all four categories of work: Sense making, Engagement, Action and Monitoring. Detailed datasets are available from the authors. Here we present examples from the dataset to illustrate our key findings.
Sense making
We explored participants' perceptions of individual and collective understanding of what EGP is, how it is different from other forms of care, and why it matters. Responses revealed widespread acknowledgement that offering person-centred care mattered, but with problems in the other three domains of Sense making (Table 1).
All participants described a belief in a person-centred approach to care as an
essential component for General Practice and primary healthcare. Some
articulated this specifically as an iterative interpretive
practice supporting personalized decision making
framed by a view of the whole person. [I work in] in a speciality of generalism in general practice … My role
is to look after patients and their illnesses, which is very much a
counterpoint to what happens in secondary care, where the systems are
set up to look after people's diseases. (Interview group, experienced
GP)
However, others found it hard to articulate the distinct expertise of the
generalist role. Some described instead the type of problems they were able to ‘manage’. [The generalist] is someone who knows a bit about everything and knows
when to ask for help … We manage simple things, and we ask for help for
more complicated things. (Interview group, middle career
GP)
Others spoke of the importance of continuity and relationships, the ‘variables’
in EGP (Figure 1), but
also reflected that these were not unique to generalist practice. For some, they
recognized a distinct expertise of professional practice but which they
described as ‘intuition’ or a ‘sixth sense’. They reveal practice which relies
on instinctive feeling rather than conscious reasoning – a tacit process of
professional practice.
25
The tacit nature of this process may contribute to the
reported perceptions that whilst patients and primary care practitioners value
EGP, the wider community lack an understanding of the role. Expert Generalist Practice – a complex
intervention.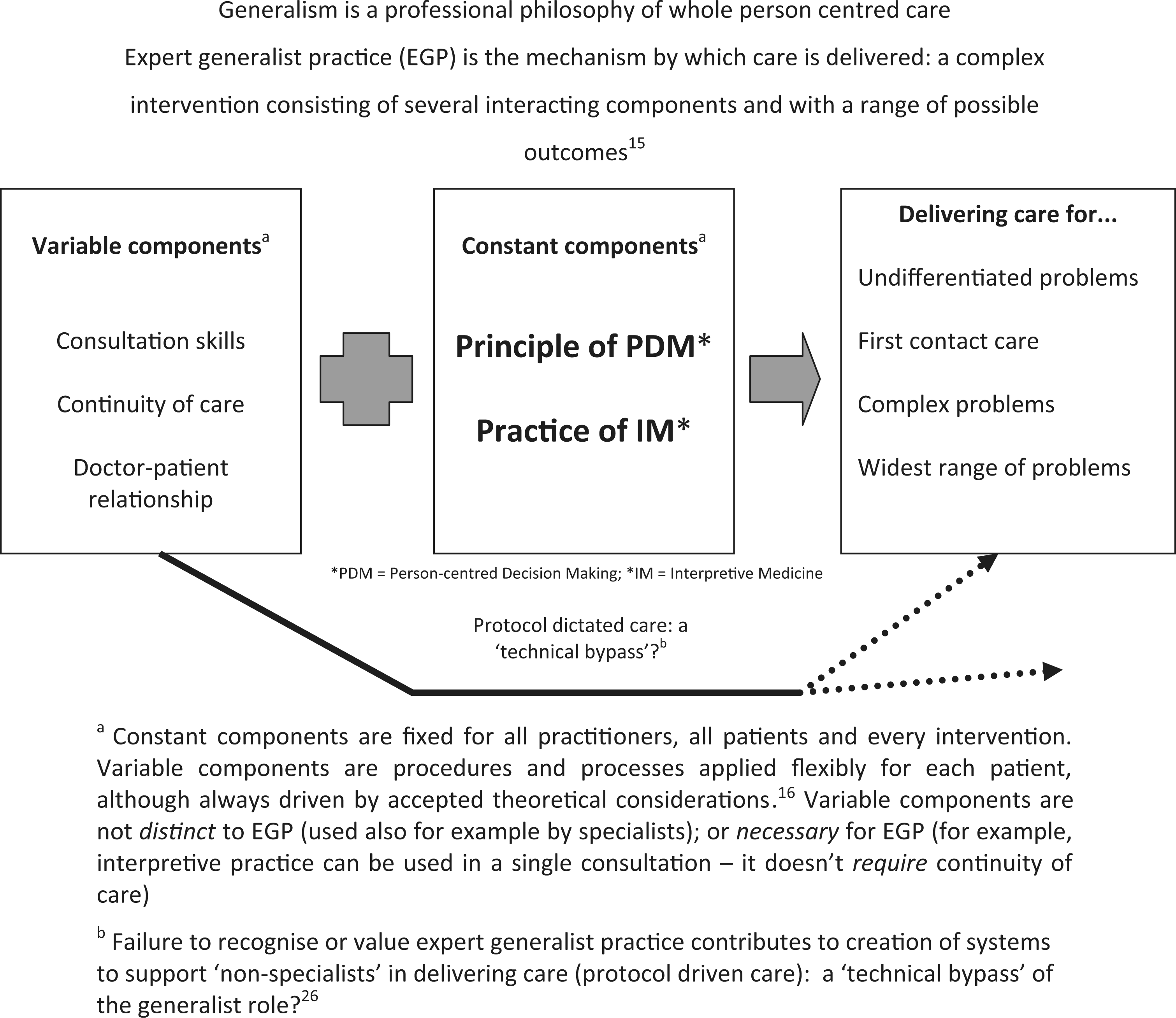
Engagement
There was evidence of personal commitment from GPs to engage with EGP. For example, some GPs spoke of the importance of continuous investment – of working in the same practice over an extended period in order to gain the historical contextual knowledge they felt they needed to work as an expert generalist. Other strategies included work to support continuity of care and relationship building (Figure 1).
In order to investigate how the ‘ideal’ of EGP translates into daily practice,
participants were also asked about the organization of care for complex patients
with multimorbidity. Responses revealed that these patients were often more
likely to be receiving care organized around protocol-driven care. As a locum, I note this is structured very differently between practices.
It is common for the practice nurse to manage chronic health conditions
using the guideline/silo approach. (Survey respondent, locum
GP)
This was perceived to stem from a lack of a system wide engagement with the
personalized approach of EGP. External priorities were perceived to be
unsupportive of EGP, with competing priorities, a lack of time and a general
increasing workload placing a significant constraint on EGP. Daily task is dealing with acute problems when the complex patients can
be silo'd or overlooked. Actually time well spent going through complex
patients but no time for this in busy day. (Survey respondent, qualified
GP)
None of our participants spoke of champions for EGP acting as beacons for
colleagues, although our interview/survey schedules did not explicitly probe for
this. Whilst we saw repeated examples of people continuing to commit to the
ideal of General Practice despite the pressures, there was a suggestion that
external constraints threatened to limit, rather than enhance, engagement with EGP. Unfortunately the tick box protocol driven model we currently run under
is promoting a lack of generalist skills and indeed an inability to
think outside the boxes. (Survey respondent, qualified
GP)
Action
Here we sought evidence of capacity for delivery of the ‘constant components’ of EGP. Again, analysis revealed a mixed picture.
Some participants clearly described being comfortable with interpretive practice
and having the skills for the task. For example, GPs described case histories of
personalized decision making and interpretive practice; delivering ‘beyond
protocol care’ which focused on the person rather than the medicine. Some
described having had formal training in the skills needed; one survey
participant spoke of gaining skills through research science training. For the
majority, expertise came through experiential learning (64% in the survey).
However these skills were not perceived to be universal. sadly, some experienced GPs and consultants either do not have these
skills or do not feel able to use them. (Survey group, qualified
GP)
The distinction between ‘knowing’ and ‘doing’ generalist practice was a common
theme. Some respondents described the impact of external constraints on their
capacity to implement the skills and expertise of generalist practice. You've always got the targets coming out at you from the computer … I
think the problem is time … you've got your 10 minutes to try and have
that consultation. It's sometimes easier just to say ‘the evidence shows
that this is the best for your blood pressure to be’, and you know,
press on. And so sometimes I suppose you do do that. (Interview group,
experienced GP)
For others, the constraint lay in the lack of ‘development of a sense of personal
and collective trust in EGP through practice’ (Table 1). For example, those who spoke
of practice as being ‘intuitive’ also described a fear of how others might judge
this type of practice. I think we do have more kind of guidelines, protocols and things. Which
are, as if ‘this is what you should do in this’. You sort of almost feel
like you don't follow the protocols, that you're doing the wrong thing.
(Interview group, qualified GP) Personally I am afraid to do something against guidelines … If I only use
my intuition, I cannot defend [myself]. That's why I am afraid of it.
(Focus group, GP trainee)
Clinical governance systems were not perceived to support a sense of ‘building
accountability through EGP’ (Table 1). As highlighted above, GPs
spoke of being fearful of ‘being wrong’. Yet they also recognized that turning
away from EGP towards ‘following a protocol’ brought potential adverse consequences. In an increasingly litigious medical society … with growing patient
expectations it is difficult to know when to stop following EBM
guidelines which inevitably causes the over-medicalising of many
ailments. (Survey group, practising GP)
These uncertainties about the implementation of EGP are perhaps captured in a
comment from one survey respondent. In theory we can do this but in practice don't always. (Survey group,
qualified GP)
Monitoring and feedback
Our final category explored the impact of feedback and monitoring in supporting
the integration of EGP into usual practice. GPs reported that they were able to
monitor the impact of care through following up their patients. Several also
highlighted the importance of shared peer reflection on experiential knowledge
and practice. Both contributed to an individual and collective sense (at least
amongst GPs) that EGP was worthwhile: 83% of GPs responding to the survey said
that EGP was worth the effort. However in one focus group, GPs reflected that
feedback was only of value if a person was receptive to it. A: I think that the only way to learn this to be an expert in
generalisation is to meet every day, many, many patients and to learn
from them, I think that they are the best teacher to us. B: Yes but you
have to be open to it. Some colleagues of ours aren't. (Focus group
participants; two trainee GPs)
There was a perception of a mismatch between the monitoring required by external
systems and that to support EGP. With a sense that those outside of General
Practice failed to understand or value the EGP approach (only 19% of survey
participants thought that their Primary Care Trust thought EGP was worthwhile).
We noted a lack of ‘formal monitoring of impact which supports a collective
sense that EGP is worthwhile’ (Table 1). nowadays when standard care is the norm, you could be criticised for
offering exceptional or special care. (Survey respondent, qualified
GP)
Discussion
Principle findings
Summary and implications – what needs to change to enhance expert generalist practice?

Strengths and limitations of our study
We recognize a number of limitations to our study methods. Our data are derived from convenience samples, predominantly from the UK. It may not be representative of the wider (and international) General Practice community. The majority of the data comes from GPs, and so we lack the insights of other primary care stakeholders including patients. We were not able to compare what GPs report of their work with what they do in practice; to explore differences between the ‘rhetoric’ and ‘reality’ of practice. Finally, enablers and constraints to practice will be context specific and so we cannot assume that the issues identified in this study would apply – for example – to hospital generalists. However, the strengths of our work lie in providing a novel and practical framework which could be applied in multiple contexts to systematically identify barriers to practice, and in turn to evaluate the impact of change.
Implications for practice
EGP makes sense to practising GPs but we note that some practitioners struggled to articulate the distinct expertise of EGP. Our data not only support the view that generalism is ‘deeply known’ 14 to (at least some) practitioners, but also suggest that the practice of EGP has become ‘lost in translation’. Some practitioners know what it is, but have no language to describe (and defend) it; referring instead to ‘intuitive practice’. Others appear to define the generalist role primarily as an all-rounder role, describing their key function as filtering out complex problems to refer on. It is perhaps unsurprising therefore that those outside of the profession fail to understand EGP.
We therefore propose the need for a body of work on Translating EGP: raising the understanding and profile of this distinct role both within the profession and beyond. The recent Royal College of General Practitioners (RCGP) report 5 has started a conversation. We offer our account of EGP as a complex intervention (Figure 1) as a further step in opening up a tacit professional model to all. We emphasize that this is not just ‘doing good general practice’. Rather this is to highlight and celebrate the two central components of EGP – a distinct expertise that is in the toolbag of some, but not all, GPs. 26 Further work is needed to translate these ideas into frameworks that make sense to wider stakeholder groups, including patients as well as policy makers; for example making use of multimedia to support communication (see for example www.youtube.com/watch?v=PZ7vfumUuHk).
We not only saw evidence of GPs and practice teams seeking to engage with EGP, but also a perception of barriers created by external, competing priorities for resources including GP time. This lack of external engagement with EGP may be altered by work to improve understanding of EGP. However, our findings resonate with a wider literature concerned by an overemphasis on community delivery of disease focused care3: defining need for care on the basis of condition focused guidelines 27 and population need rather than a personal assessment of need. We propose a new body of work on Priority setting for EGP. To explore how to assign need for care based on an understanding of personal experiences of health as a resource for living. Our longitudinal study of the experience of living with chronic illness suggests we need to design needs assessment for personalized care on the capacity to manage the work of daily living. 28 We need new priority setting and risk stratification approaches supporting a generalist approach.
Not all GPs reported that they had the skills for EGP. Even GPs who reported having skills in EGP expressed concerns about their capacity to defend the use of these skills, especially if making ‘beyond protocol’ decisions. These findings suggest a shortage of confidence or skills in the interpretive medicine elements of EGP and particularly in a key element of that role – the ability to judge the trustworthiness of the interpretation. We highlight Trusting EGP as a third constraint to practice.
The GP curriculum describes that a GP should have specific problem-solving skills including the capacity to ‘selectively gather and interpret information … and apply it in an appropriate management plan’. 8 Elsewhere, that GPs should take a holistic approach using the ‘biopsychosocial’ approach to understand the whole patient. 8 The biopsychosocial model is recognized to have ‘broaden[ed] the scope of the clinician's gaze’. 29 But gathering more information is not enough unless we also have a framework by which to use it. The biopsychosocial model has been criticized for not ‘guid[ing] us on how to prioritise’. 30 Our findings suggest that we perhaps need to revisit and extend these elements in order to support interpretive practice, particularly in a modern context where a particular view of evidence-based practice is dominant. 6
We suggest the need to review the RCGP GP curriculum and continuing professional training to include greater emphasis on the critical interpretive skills of practice. Gabbay and le May's 25 ethnographic study of how contextually adroit GPs engage in interpretive practice to generate knowledge-in-practice-in-context, or mindlines, offers one source of study. Our own Exploratory Decision Map, 6 translating thinking on demonstrating the trustworthiness of interpretive practice from the qualitative research field into clinical practice, offers another approach. Both identify skills of scholarship (discovery, integration, application and inspiration – see www.sapc.ac.uk/index-php/academic-primary-care) at the heart of professional primary care practice: both clinical and academic. This indicates that generalist primary care would be strengthened by closer working between the clinical and academic arms of the discipline.
Finally, we saw evidence that GPs already monitor the impact of personalized decision making through their continued relationship with patients. However, they felt that external quality monitoring processes did not recognize or support this learning. Current monitoring fails to support the development of trust in, and understanding of, the merits and limitations of EGP. We therefore propose the need for a fourth body of work on Identifying the impact of EGP. Supporting practitioners in evaluating their individual practice has the potential to enhance skills and confidence in interpretive practice (Trusting EGP). If we can also capture that learning, we may also support development of an evidence base from practice on how and when expert generalist care offers something different to, and better than, specialist care. We have recently described a framework by which to generate this evidence from practice – the Generalism in Action framework. 31
Future research
Our goal was to understand how we might enhance the practice of generalist expertise in the primary care setting. Our study has identified four key constraints to EGP and proposed solutions to system wide approach supporting a primary healthcare vision of Health For All. 3 The next step will then be to identify if changes to enhance EGP make a difference to patient outcomes. This will be a focus of the next stages in our research.