
Abstract

Retropharyngeal abscesses (RPAs) are extremely uncommon in very early infancy and have specific management challenges.
Case report
A six-week-old thriving, full term male presented to a peripheral emergency department (ED) with a left anterolateral neck swelling. This was associated with overlying erythema and he was febrile at 38.1°. The parents of the child did not wait for the child to be seen but returned the following day for review. The erythema and swelling had increased and a palpable mass in the left neck with associated cervical lymphadenopathy was present. On initial blood investigations, he had a white cell count (WCC) of 16.6 and a C-reactive protein (CRP) of 69.2. He was admitted and commenced on IV flucloxacillin and cefotaxime. Ultrasound of the neck demonstrated a 3 × 2.7 × 2.1 cm lobulated lesion consistent with an abscess. His antibiotics were subsequently changed from flucloxacillin to vancomycin and arrangements were made to transfer the patient to a tertiary paediatric centre.
On arrival, the child had mild stertor but no increased work of breathing. He was saturating at 100% on room air. On examination, a large palpable suprahyoid left neck swelling anterior to the sternocleidomastoid muscle was present with overlying erythema. He had mild trismus and torticollis to the left. There was anterior displacement of the posterior and left lateral pharyngeal wall present on transoral examination. Repeat WCC was 8.6 and CRP was 72. A CT was performed that demonstrated a large RPA with inflammatory and phlegmonous changes into the left parapharyngeal space predominantly and extending inferiorly to the level of the C5 vertebra (Figure 1). An opinion was sought from the otolaryngology department and theatre was booked to secure the airway and drain the abscess.
Contrast CT scan axial and sagittal views. Collection occupying the retropharyngeal space in a 6 week old male.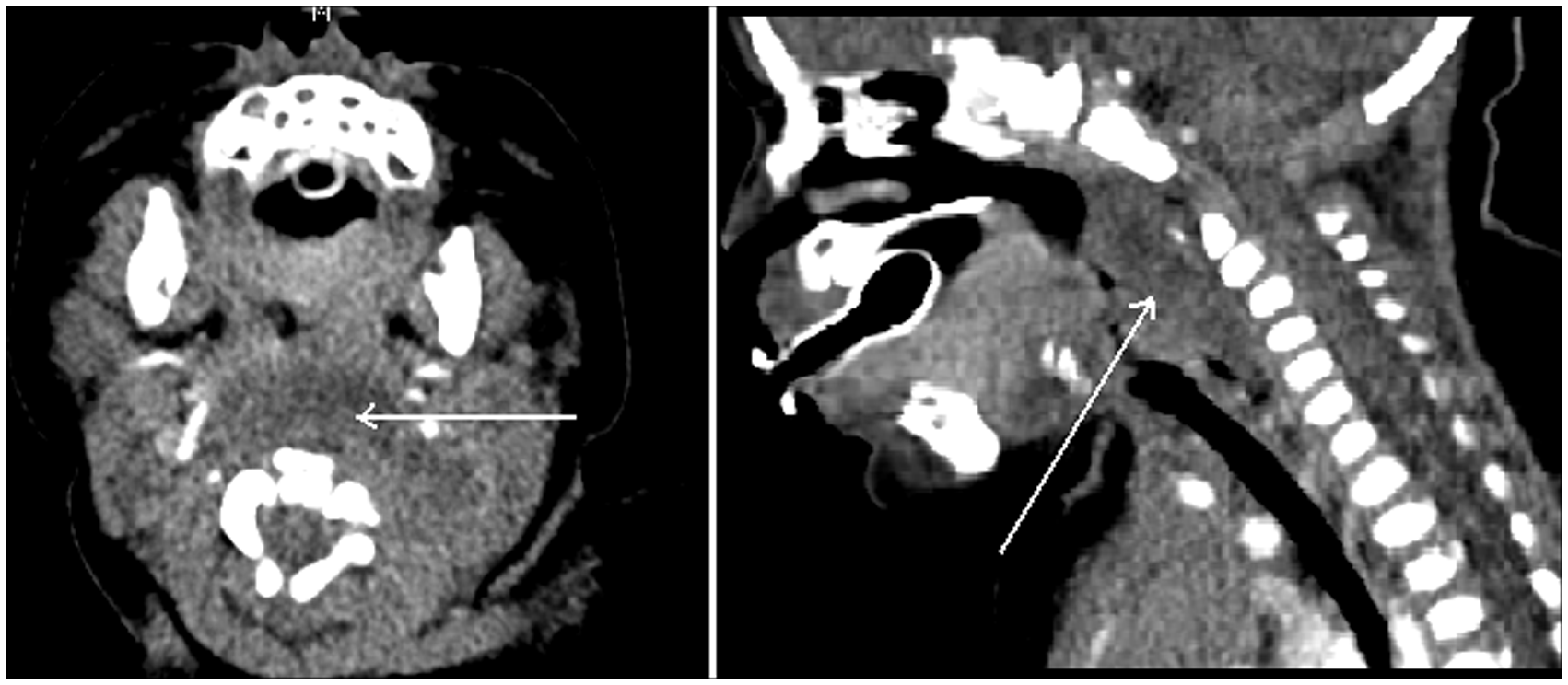
A gaseous induction and a 3.0 oral endotracheal tube were used to secure the airway. A Lindholm laryngoscope was used to visualize the posterior oropharynx and needle aspiration utilizing a spinal needle was performed to confirm the presence of a collection. One millilitre of 1:100,000 xylocaine with adrenalin was used to infiltrate the posterior pharyngeal wall and a 2 cm vertical paramedian incision was made. Blunt dissection into the cavity combined with pressure to the left neck expressed approximately 6–7 ml of pus. Swabs were taken and sent for microscopy, culture and sensitivity. The wound was washed out with hydrogen peroxide and normal saline. A Penrose drain was inserted transorally into the cavity and secured with a 4.0 silk suture to the posterior pharyngeal wall adjacent to the incision.
Post-operatively, the patient was admitted into the paediatric intensive care unit (ICU) and was continued on IV vancomycin, cefotaxime and metronidazole. The patient remained intubated, while the swelling resolved and was fed via nasogastric tube. The Penrose drain was removed on day 2 post-op in ICU and the child was extubated on day 3. Staphylococcus aureus sensitive to cephalothin, clindamycin and fluxloxacillin was cultured. IV vancomycin and cefotaxime was continued for five days with oral flucloxacillin for a further five days. Feeds were commenced as normal on day 5. He was transferred back to the peripheral hospital the following day without further complication.
Discussion
Paediatric RPA is an uncommon entity and is often associated with an antecedent upper respiratory tract infection. 1 Suppurative adenitis of the retropharyngeal lymph nodes in younger patients, often the precedent to abscess formation, reflects the immature immune response in this population. 2 The incidence of RPA has increased in recent years, the reasons for which are not clear but are thought to be due to evolving bacteriology as well as improving investigative modalities. 1
RPA commonly occurs between the ages of 1 and 6 years; 1 however, patients can present at any age including neonates. Typically, children less than one year present with agitation, fever, lymphadenopathy and a neck mass and their length of symptoms prior to admission tends to be shorter than older children (approximately 3 days). 3 RPA in early infancy is described in the literature albeit very uncommonly. The presentation of this subpopulation is variable and can include submandibular swelling, inconsolable irritability, poor feeding, stridor and severe to complete airway obstruction. 4
The age of our patient (6 weeks) offered a unique management challenge. On review of the literature, very few specific case reports have been described of a patient this young. Traditional management of this early age group has included prompt surgical intervention, usually a transoral incision and drainage of the abscess. Controversially, there has been increasing debate regarding the role of conservative management with some authors reporting success managing patients with intravenous (IV) antibiotics alone. 2
Similar to other cases, 4 a trans-oral approach was used for our patient. Uniquely however, a drain was inserted transorally and secured to the pharynx, analogous to what occurs with external drainage. While this is not typical practice for routine transoral drainage, in this case the goal was to avoid a transcervical approach with minimal associated morbidity.
Most RPA are polymicrobial with the most common causative organisms including group A beta-haemolytic Streptococcus (GABHS), S. aureus and upper respiratory tract anaerobic organisms.1,5 The increased incidence of RPA in recent years has coincided with an emergence of GABHS and methicillin-resistant S. aureus (MRSA) in various centres in the United States.1,2 A similar rise of GABHS and MRSA has not yet been identified in Australia. Swabs taken at the time of operation grew S. aureus sensitive to cephalosporins and flucloxacillin, which is the most common pathogen in patients with RPA less than age one. 3
Notably in this case, there was delay in receiving treatment from the onset of symptoms. Although there is a 4-h-wait government initiative in NSW, limited resources in ED results in breaching of this legislation, prolonged wait periods and patients leaving the ED without review. Complicating the clinical picture, the patient’s family were non-English speaking and from an at-risk population group. These above factors contributed to both delayed presentation and treatment of the child.