
Abstract
Objectives
To evaluate the appropriateness of proton pump inhibitor (PPI) prescribing by conducting an audit of medical inpatients against recommended guidelines.
Design
Questionnaire-based study. All medical wards were audited and different information was documented by patients' medical records review (both hospital visit notes and general practitioner's letters) and short interview, where we asked them to name the clinical reason for using PPI.
Setting
This study was carried out in the setting of a regional hospital (537-bed, secondary care referral centre) in Ireland.
Participants
The study participants were all consecutive medical patients admitted to the medical wards at Waterford Regional Hospital, Waterford.
Main outcome measures
The appropriateness of PPI usage in our regional hospital by assessing the level of its prescribing against published guidelines (NICE, 2000).
Results
During the audit period, 205 consecutive medical inpatients were assessed. Seventy-nine percent (162 out of 205) of the studied patients were found to be using PPI. For 45% (n = 73) of patients, there was no documentation of valid indication for being on PPI. Overall, 64% of patients were prescribed PPI by hospital doctors, either during their current or previous admissions. We noted that 31% (n = 51) of patients were taking PPI for ≥2 years and another 25% of patients were using PPI for about one year. Only 12% (n = 20) of patients had undergone endoscopy procedures.
Conclusion
Inappropriate use of PPI remains common in hospital practice. The risks of using long-term PPI must be weighed against the benefits.
Introduction
With the advent of proton pump inhibitors (PPI), the treatment of different acid-related gastrointestinal disorders has revolutionized. These are the most potent anti-secretary agents of hydrochloric acid into gastric lumen. PPI are indicated for the treatment of gastric or duodenal ulcer, dyspepsia, NSAIDs induced ulcer, for the treatment and maintenance of gastro-oesophageal reflux disease, and for the eradication of helicobacter pylori and hypersecretory disorders, such as Zollinger Ellison syndrome. Because of these common medical problems, PPI are one of the most widely prescribed medications across the globe, and also there is a common belief that PPI have very low levels of toxicity and high levels of efficacy. However, evidence is mounting that these medications can lead to some troublesome and even serious side-effects. In 2000, the National Institute for Health and Clinical Excellence (NICE) published guidelines and recommended the doses and duration of PPI usage in different clinical indications. 1 However, the inappropriate prescription of PPI continues to rise every year, and this also significantly affects the total health expenditure.
We tried to evaluate the appropriateness of PPI usage in our regional hospital by assessing the level of its prescribing against published guidelines. 1 Based on the reports from other institutions, we hypothesized that PPI are over-prescribed or inappropriately prescribed in the study institution. Hence, we carried out an audit of medical inpatients to assess: (1) the clinical condition for which PPI were prescribed; (2) duration of therapy; (3) any investigations performed to confirm the diagnosis; and (4) the extent of patient's knowledge of their treatment by asking them to name the clinical reason for using this drug.
Methods
This study was carried out in the setting of a regional hospital (537-bed, secondary care referral centre) in Ireland. The study participants were all consecutive medical patients admitted to the medical wards at Waterford Regional Hospital, Waterford. All six medical wards were audited and the prescription charts were surveyed to identify patients on PPIs; this was carried out over a period of two weeks. Inclusion criteria were all consecutive patients admitted to the medical wards. Patients excluded from this audit were: those under the age of 18 years; patients who did not speak English; patients with learning difficulties; patients with a mini mental state result of below 12 points; and patients who were deemed to be too ill to talk to. We devised a structured pro forma for documenting different information. To our knowledge, there is no validated questionnaire available to assess the inappropriate use of PPI. In the first step, patient's medical records (both hospital visit notes and general practitioner's letters) were reviewed for following information: demographic details; name, dosage and duration of the PPI; whether PPI was started during this admission; who initiated PPI, whether hospital doctors or the general practitioner (GP); any endoscopies performed to support the diagnosis; and any documentation of indication for prescribing PPI. In the second step, a short interview was carried out with each patient, where we evaluated the extent of patient's knowledge of their treatment by asking them to name the clinical reason for using PPI; this was carried out in an attempt to identify discrepancies between patient reporting and medical records data. Medical record review was used to document the duration of therapy, and GP's surgery was contacted in the case of any missing data. Medical record reviews and interviews were conducted by the authors (MH, FY, SKMG, FA, FW). The study was conducted in adherence with the Declaration of Helsinki and International Committee on Harmonization good clinical practices.
Statistical analysis was performed using the SPSS software, version 17. Significance was defined as P < 0.05 (two-tailed). A chi-square (X 2 ) statistic was used to investigate the distributions of categorical variables, and continuous variables were analysed using Student's t-test. We applied odds ratios (OR) and associated confidence intervals (CI) to measure association between different variables and PPI prescription.
Results
Demographic characteristics and the brief summary of results
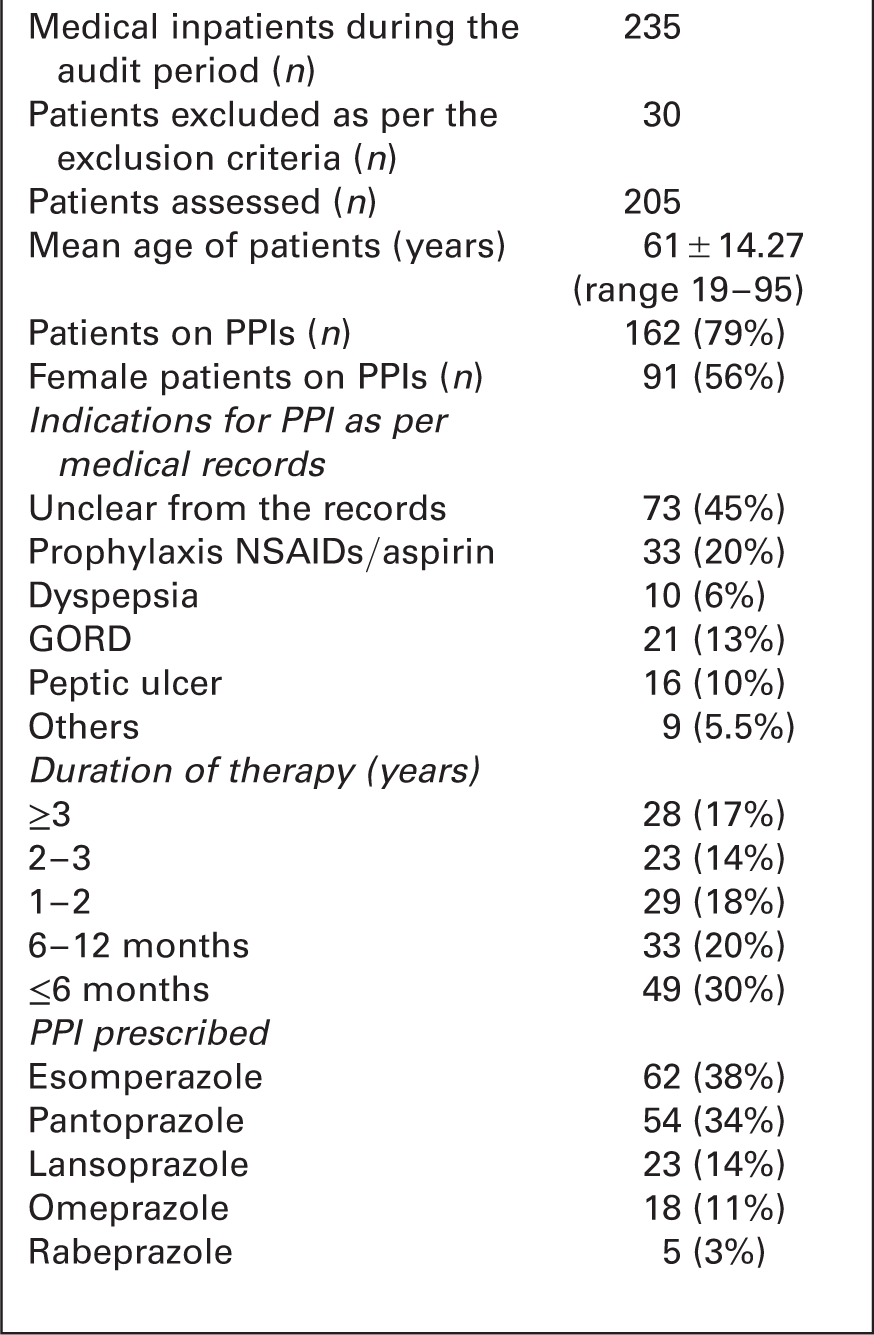
We also documented the doses of PPI used either for healing or maintenance purposes. It was noted that only 14% (23 out of 162) of patients were prescribed recommended maintenance doses of PPIs, and significantly vast majority of patients were using long-term high doses of PPIs. Overall, esomperazole was being used by 38% (n = 62) of patients, pantoprazole in 34% of cases, lansoprazole in 14% of patients, omeprazole in 11% of cases, and rabeprazole was used in only 3% of patients. Out of 33 patients who were commenced on PPI therapy during their current hospital admission, 44% were prescribed pantoprazole, 29% were started on esomperazole, 22% were started on lansoprazole, and omeprazole was prescribed in only 5% patients. Only 12% of patients (20 out of 162), had their upper gastrointestinal (GI) endoscopies for confirmation or justification for being on PPIs. On univariate analysis, only gender was noted to have a statistically significant association with PPI prescription – significant positive association with female gender with OR 2.163, 95% CI 1.083–4.320, P = 0.029.
Discussion
Characteristics of the cohort: PPI users vs. patients who were not prescribed PPI

One major problem identified in our study was poor documentation of indication for being on PPI. Good documentation is essential to assess the evolution of a patient's condition. In a typical hospital setting, many different professionals deal with one patient, either during the same admission or subsequent visits. Therefore, clear documentation and assessment of up-to-date information is vital. Although, there is a continuity of care in a primary care setting, there are obvious difficulties of rationalising the drugs being prescribed and re-issued in subsequent visits to a hospital. We suggest that there should be proper citations of reasons for being on PPI, and a clear advice on when to review the therapy. A clear documented advice in the care report at the outset can avoid future confusions and inappropriate repeat prescriptions.
This study also provides other important information. In contrast to previous studies,3–9 esomperazole and pantoprazole accounted for 72% of overall prescriptions, and omeprazole was used in only 10% of patients. In terms of cost-effective prescribing, this is reassuring as omeprazole was found to be the PPI with the highest ingredient cost under the community drug scheme in 2002; 26 however, we noted that least expensive PPI (rabeprazole) was the least prescribed in our patients. It was alarming that upper GI endoscopies were carried out in only 12% of patients, and a vast majority of patients were prescribed long-term PPI therapy without adequate investigations. This is a matter of concern, as in particular, their potent action can suppress the features and can delay the diagnosis of gastric cancer. Hence, referral to an endoscopy unit is recommended for high-risk group of patients aged over 45 years with new onset of dyspepsia. 27 It is noteworthy that rapid disappearance of dyspeptic symptoms does not make the suspicion of malignancy unlikely, and it should not delay the referral for upper GI endoscopy. We acknowledge that there are few limitations to this study. For example, no history was documented about the usage of non-pharmacologic treatments for acid-related GI disorders, and the potential recall bias, given that some data were obtained from patient interview. Following this audit, a range of measures have been taken to improve the compliance of guidelines. Staff awareness was increased by local presentations. Moreover, protocol has been established to document the indication and the time when to review regarding the dose and duration of therapy. We plan to close the audit loop by repeating the same review of clinical practice in 2 years time in order to establish what improvements in care had occurred in the intervening years.
Acid-related gastrointestinal disorders are extremely common and they make one of the most common reasons for general practice and specialist attendances. These disorders usually occur as a result of inherent abnormalities of gastric secretion homeostasis or a defect in normal anti-reflux barrier. However, these can also occur either as a complication of most of the chronic systemic disorders or being iatrogenic due to certain medications. Proton pump inhibitors are the most potent inhibitors of acid secretion which are available to date. These have become the treatment of choice for different acid-related gastrointestinal disorders, and have completely changed the outlook of these diseases. These drugs have caused the virtual abolition of elective surgery for peptic ulcer disease, and a marked reduction in mortality and morbidity of stress-related ulcers and NSAIDs-induced gastropathy.
Due to their apparently favourable safety profile, PPIs are one of the commonest drugs being prescribed worldwide, and their usage is increasing. Guidelines were proposed in July 2000 and a particular emphasis was given on the duration and the dosage of PPI being prescribed. However, there are ample reports to document inappropriate over prescription of PPI across the globe, in both primary and secondary care.2–9 We noted that 79% of our inpatients were using PPIs. Previous studies have shown lesser percentage of patients using PPIs; this may simply reflect the patterns of PPI prescription during the years. There are two main concerns pertaining to over-prescription of PPIs: drug expenditure issues as PPIs are generally quite expensive, and secondly there are growing safety concerns. As far as the cost issue is concerned, total expenditure under the community drug schemes in Ireland on PPI has risen dramatically. This particular expenditure was €3.24 million in 1993, €7.6 million in 1996, €23.89 million in 2000, and it rose further to €64 million in 2002. With reference to the safety issues, there are growing concerns of their long-term safety. A recent study has linked PPI use to an increased risk of pneumonia. According to this study, hospitalized patients who receive acid-suppression medications such as PPIs have 30% increased odds of developing pneumonia while in hospital. 10 Moreover, there is an increasing body of evidence suggesting that the use of PPIs for ≥1 years is associated with a significantly increased risk of hip fracture and other osteoporotic fractures, with most studies showing a strong dose and duration-response relationship.11–15 Hypochlorhydria due to PPI usage has been implicated in the causation of osteoporotic fractures and vitamin B12 deficiency.16,17 Two recent reports have further confirmed the causal role of acid suppression in the development of nosocomial C. difficile infections.18,19 There are also concerns that their judicial use can delay the diagnosis of gastric carcinoma. 20 Furthermore, there can be acid hyper secretion after stopping PPIs 21 which may potentially cause drug dependence. A recent meta-analysis of seven randomized controlled trials for bleeding peptic ulcers has concluded that there is no 30-day benefit for high doses on rate of re-bleeding, need for surgical intervention, or mortality. 22 These results highlight that high-dose PPIs do not provide additional benefit relative to lower-dose PPIs for patients with bleeding peptic ulcers and that high-dose PPI use among other patient populations could have negative consequences for bone health and C. difficile infections. Moreover, there is growing evidence of the loss of beneficial effects of clopidogrel when used concomitantly with a PPI, leading to adverse cardiovascular outcomes.23,24
In conclusion, we have demonstrated that a vast majority of our medical inpatients were inappropriately prescribed PPIs. As with all medications, the risks of using long-term PPI must be weighed against the benefits, and this depends on specific patient factors. Regular monitoring and re-evaluation by the attending physicians, either in primary or secondary care, regarding the continuing need for PPIs remains vital. Moreover, empowering patients by educating them about their disease and a care plan at the outset before commencing any medications remains crucial as regards any improvement in clinical practice is concerned.
DECLARATIONS
Competing interests
None declared
Funding
None
Ethical approval
Not applicable
Guarantor
MH
Contributorship
All authors contributed equally
Acknowledgements
None
Provenance
Submitted, peer reviewed by Michael Graham