
Abstract
Objective
To evaluate the hormone receptor status and human epidermal growth factor receptor 2 (HER2)/neu gene expression among Jordanian women with breast cancer. To classify our patients into molecular subtypes and to correlate the results with age of the patients and tumour grade.
Design
Evaluation of estrogen receptor (ER), PR and HER2/neu was done by standard immunohistochemical technique and subclassification into molecular subtypes.
Setting
Jordan University Hospital, Amman, Jordan.
Participants
One hundred and ninety-three cases of breast cancer diagnosed at Jordan University Hospital.
Main outcome measures
Molecular subtypes of breast cancer, age and tumour grade.
Results
All the cases were divided into two groups: the young age group less or equal 50 years of age and the older age group more than 50 years of age. The cases were subclassified into luminal A, luminal B, basal cell like (BCL) and Her2/neu+. In older age group, the most common subtype was luminal A (72%). In this age group, most of the cases (48%) were of grade II. In younger age group, 47% of the cases were of luminal A subclass. In this age group, 42% were of grade I.
Conclusions
Molecular subtyping of breast cancer is an essential predicting factor of tumour response to hormonal therapy. This fact puts increased stress on the urgent need for the development of reliable and reproducible classification systems.
Introduction
Breast cancer (BC) is the most common cancer among women in Jordan and it is the leading cause of cancer death. 1 There are several clinical and histopathological prognostic parameters that have been studied. 2
Among the most important are expression of estrogen receptor (ER) progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER2). 3 ER status is used in clinical practice as an indicator of endocrine responsiveness and as prognostic factor for early recurrence. 4 ER positive tumours (ER+) comprise the majority of breast cancer, accounting for up to 75% of all cases particularly in postmenopausal women (>50 years). 4
It was found that ER is probably the most powerful single predictive factor in breast cancer. 5 Progesterone receptor (PR) positive tumours comprise 55–65% of breast cancers and have been shown to have a better prognosis than PR negative tumours and can help to predict the response to hormone treatment. 6
Although ER expression is the main determinant of response to hormone therapy in breast cancer, lack of PR expression in ER positive tumour may contribute to resistance to hormone therapy as it was noticed that ER+/PR− tumours are generally less responsive than ER+/PR+ tumours. 7
HER2/neu gene amplification/protein overexpression is a predictor of poor response to systemic chemotherapy and thus prognosis. 8 HER2/neu overexpression occurs in 18–20% of all breast cancers. 9 HER2 expression shows an inverse relationship with both ER and PR expression. 10
Following the development of humanized monoclonal antibody against HER2 (trastuzumab), the use of anti-HER2 agents in HER2 positive breast cancer patients became mandatory. 11 It has been reported that HER2 positivity is associated with relative, but not absolute resistance to endocrine therapies in general 12 and is a predictor of poor prognosis. 13
Studies showed that molecular classes of breast cancer are variable; therefore, several attempts to validate and translate these molecular classes into defined groups can be identified in routine practice. 14 Most classifications used a combinational expression of immunohistochemical (IHC) markers including ER, PR and HER2 with or without additional markers such as basal markers and proliferation markers. BC was categorized into four main groups: luminal A (ER+ and/or PR+, HER2−), luminal B (ER+ and/or PR+, HER2+), basal cell like (BCL) ((triple negative phenotype), ER−, PR−, HER2−) and HER2 positive tumours (ER−, PR−, HER2+). 15
Luminal A tumours were shown to be associated with good prognosis and less aggressive behaviour if compared with the BCL or HER2 positive groups. 16 BCL subtype has been associated with aggressive behaviour, lack of response to hormonal therapy and shorter survival. 15
Routine IHC evaluation of breast cancers may therefore an alternative to costly genotyping assays. These classifications have been extensively studied worldwide 17 ; however, only few if any studies have investigated the molecular subtypes of breast cancer in our area. In the present study, we therefore tried to classify our patients according to molecular subtypes and to compare to other ethnicities.
Material and methods
Retrieval of patients
This is a retrospective study that tried to evaluate breast cancer in Jordan with regard to molecular characteristics.
One hundred and ninety-three cases of infiltrating ductal carcinoma diagnosed at Jordan University Hospital were obtained from histopathology department archives between 1 January 2007 and 31 December 2011. All the cases were routinely evaluated immunohistochemically for estrogen and progesterone hormone receptor status and for HER2/neu gene expression using standard immunoperoxidase method, i.e. avidin-biotin complex peroxidase method (vector peroxidase ABO kit-PK4001 and PK4002; Burlingame, CA, USA). Adequate tissue fixation in 10% neutral buffered formalin for minimum 6–48 h was routinely ensured. The antibodies used for ER, PR and HER2/neu were monoclonal mouse anti-human estrogen receptor, BioGenex, USA (clone ID5; ready to use), monoclonal mouse anti-human progesterone receptor, BioGenex (clone PR 88, ready to use) and anti-HER2/neu (C-erb B-2) (clone CB11, Novocastra).
A positive control with a tissue sample known to express the antigen of interest was included on each histologic slide. Evaluation of IHC staining was routinely done by the reporting local pathologists according to international guidelines. With regard to the hormone receptors, the results were expressed as positive or negative, whereas for HER2 expression, the results were reported according to the guidelines of the FDA-approved HercepTest. Results were included in the histopathologic diagnostic report communicated to the clinicians.
BCs expressing ER and PR in >5% of neoplastic cells were considered as positive for hormone receptor expression. For Her2/neu, tumours were scored as negative if the membrane staining was negative or weak and incomplete (score 0 or 1+) whereas cases with strong complete membrane staining were scored as positive (score 3+). All cases with ambiguous expression of Her2 (score 2+) were considered as negative or positive according to the results of FISH analysis carried out on sections obtained from the same tissue samples as those for hormone receptors.
Classification of breast cancer
Molecular classification of breast cancer subtypes.
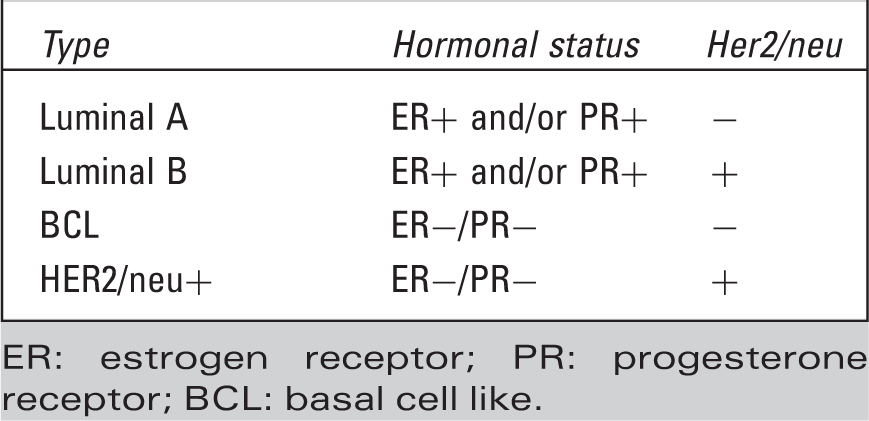
ER: estrogen receptor; PR: progesterone receptor; BCL: basal cell like.
Histological grade of the tumour based on the Nottingham combined histological grade was used and abstracted from the pathology records. The tumours were histologically graded into grades I, II and III, respectively.
Results
Distribution of molecular subtypes of breast cancer by age groups.

Distribution of molecular subtypes by grade in young age group (≤ 50 years old).

Distribution of molecular subtypes by grade in older age group (> 50 years old).

Discussion
The prognostic and therapeutic implications of ER, PR and HER2/neu status in breast cancer are well-established. 19 As gene expression profiling analysis is getting easier and cheaper, breast cancer can be classified into molecular subtypes utilizing routinely done markers. Although IHC-based assays do not provide as much biological insight into tumour biology as gene-based ones do, they allow classification of tumour at affordable costs and in the absence of fresh tissue specimens. 20 Our data demonstrate that the majority of all the cases were classified as luminal A (60%) which offers the best prognosis of all subtypes. It is higher than what is reported by Salhia et al. 21 in Egypt (44.3%) and by Ben Abdelkrim et al. 22 in Tunis (51.5%). Luminal A subtype was also predominant in Asian Americans. 23
Thirteen percent of all our cases were classified as luminal B subtype which was similar to figures previously reported in North American and European women (6–19%) 24 and Tunisian women (16%) 22 but in contrast to what was found in Egyptian women (24.6%) previously reported by Salhia et al. 21 Luminal B tumours are prognostically less favourable than luminal A tumours but still less aggressive than BCL tumours. 25 In our cases, it appeared to be more prominent in the younger age group (23%) compared to the older age group (5%). This might indicate that when tumours in the younger age group are positive for hormone receptors there is more likelihood to be positive for Her2/neu gene mutation than in the older age group. Fifteen percent of our cases were classified as BCL subtype similar to the incidence in Sudan (15.9%) 26 which is slightly less than in Egyptian and Tunisian women (19% and 18%, respectively).21,22 The incidence of BCL subtype in our cases was slightly higher than what was reported in Moroccan breast cancer patients (12.6%) 27 but almost double than that of American Chinese (8.5%), triple than that of American Flipino (5.9%) and American Japanese (5.7%). 23 BCL cases in our study were evenly distributed in the two age groups (15% vs. 14%), respectively, and lower than the incidence of BCL subtype in African American women (21.2%). 28
The percentage of our cases classified as HER2/neu+ (12%) was similar to that in Asian American (12%) 23 and Egyptian women (12%) 21 and African American women (11.6%) 28 but slightly lower than in Tunisian women (14.5%). 22 However, the frequency of HER2/neu+ subtype in Saudi cases was more than double our cases (28%). 29 The HER2/neu+ subtype was more prominent in the younger age group (15% vs. 9%, respectively) which might be indicative of the role of HER2+ mutation in the development of breast cancer at younger ages. When the molecular subtypes correlated to the tumour grade (Tables 3 and 4), it appeared that luminal A tumours were most frequently of grade I, 42% of all cases in the younger age group while luminal A tumours in the older age group were most frequently of grade II (48%) indicating that the age of the patient might impact on the aggressiveness of the tumour within the same subclass. In BCL and HER2/neu subtypes, most of the cases were of grade III in both age groups (71% and 57% respectively in the younger age group) and none of the cases were of grade I. This correlation between the tumour grade and molecular subtype is evident in both age groups indicating that these two subtypes are more aggressive in behaviour and tend to present at higher grade from the start.28,29
Conclusion
Luminal A is the most prominent subtype of female breast cancer in the Jordanian population. HER2 gene mutation might play a role in the development of breast cancer at a younger age. Although this classification could be useful in the clinical practice as an indicator of the behaviour and response to therapy, there are questions that still remain unanswered and which should be studied in future.