
Abstract
Objectives
To implement an identification and brief advice (IBA) intervention to detect low-risk/hazardous alcohol consumption.
Design
Implementation was guided through the use of quality improvement tools and training.
Setting
This study was conducted over an 18-month period from April 2010 to September 2011 on a 42-bed acute medical unit at a central London acute hospital.
Participants
All medical patients over the age of 18 admitted to the acute assessment unit were eligible; any patient unable to provide a medical history either through language barriers or due to illness was excluded.
Main outcome measures
Percentage of medical patients admitted each week to the acute assessment unit who were screened for low-risk/hazardous alcohol consumption.
Results
Weekly data were analysed in time series run charts and cross-referenced to the date of educational sessions and their effect on the uptake of screening monitored. A demonstrable change in the mean percentage number of patients screened was observed in different time periods, 67.3–80.1%, following targeted teaching on the AAU.
Conclusions
Our study demonstrates the successful use of quality improvement methodology to guide the implementation of Alcohol Use Disorders Identification Test-Consumption (AUDIT-C), an IBA intervention, in the acute medical setting. The incorporation of the AUDIT-C into an admission document has been well accepted by the junior doctors, attaining an average (mean) of 80% of patients being screened using the tool. Targeted teaching of clinical staff involved in admitting patients appears to be the most effective method in improving uptake of IBA by junior doctors.
DECLARATIONS
This article presents an independent research commissioned by the National Institute for Health Research (NIHR) under the Collaborations for Leadership in Applied Health Research and Care (CLAHRC) programme for North West London. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
This work was supported by the National Institute for Health Research (NIHR) Collaboration for Leadership in Applied Health Research and Care (CLAHRC) for Northwest London and the Chelsea and Westminster Hospital Foundation Trust. SR Woodrow, a Darzi Fellow, was funded by NHS London partnered by the London Deanery and the King's Fund (with Manchester Business School).
Ethics approval was not required for this work as it is part of a service evaluation and improvement project.
SRW
VPBG, MRF originally conceived the study; SRW and JL undertook the implementation work; SRW wrote the first draft; all authors contributed in the revision of the manuscript.
Jens Skogen
Introduction
The United Kingdom faces an epidemic of alcohol-related liver disease with rising mortality, increasing use of our healthcare services and consequently a rise in the NHS costs incurred.1,2 In 2008, more than 78% of costs for alcohol use were directly related to hospital-based care. 3 People with alcohol use disorders who commonly present to secondary care with alcohol-related problems demonstrated a 71% increase in hospital admissions of patients with chronic liver disease, largely related to alcohol liver disease, over the past 25 years. 4 Patients rarely seek help for their alcohol problem, which is compounded by the fact that frequently patients may not have an adequate alcohol history taken by clinical staff on admission to hospital. 2 The failure to identify patients with a concurrent alcohol use disorder on admission to hospital represents a significant missed opportunity to address their lifestyle issues early. Consequently when identified at a later date, these problems can become chronic and harder to treat.
Screening for alcohol consumption provides one potential solution. It can aid in the identification of alcohol as a factor in the diagnosis of a patient's presenting complaint and provide an opportunity to educate patients about the risks of their alcohol use. Brief advice is an opportunistic intervention directed at excessive drinkers who have presented with problems not related to alcohol. 5 Brief advice takes approximately 5 min to deliver and includes information on the levels of risk associated with the patient's own drinking behaviour and encouragement to cut down whilst incorporating suggestions on how the patient might achieve this. 6 Identification and brief advice (IBA) is considered to be one of the most cost-effective strategies for preventing alcohol-related harm, with one in eight patients who receive brief advice reducing their drinking to within low-risk levels. 7
On an individual level, it can reduce risk and harm and, if widely used, can bring benefits at a population level over time.8,9 Screening and referral for brief intervention has demonstrated reductions in the number of emergency department (ED) attendances and by inference this would incur direct cost savings. 10 However, routine screening as part of the admission process is not often incorporated into everyday practice within acute care. 11
In the UK, London Boroughs have high rates of alcohol-related admissions, with the borough of Hammersmith and Fulham having one of the highest rates in London. 12 Chelsea and Westminster Hospital NHS Foundation Trust primarily serves four Primary Care Trusts, including Hammersmith and Fulham. IBA is being incorporated into routine practice in local primary care as well as in the ED. However, they are rarely used when admitting a patient to the ward. Moreover, the national drive to reduce ED waiting times in England may have had the unwanted effect of removing the opportunity to perform IBA before patients are transferred to the acute assessment unit (AAU), a short-stay admissions unit. Junior doctors and other front-line clinical staff offer a potential solution to this conundrum by providing IBA in the AAU and other clinical environments away from the ED, where these patients often present. 13 This necessitates the appropriate training of staff to identify patients with potential alcohol problems and to subsequently provide brief advice and referral to an alcohol health worker (AHW) for a more detailed discussion, lasting up to 20 min, known as brief intervention, as recommended by the National Institute for Clinical Excellence (NICE).2,13
There is evidence of the positive effectiveness of IBA, as demonstrated in a recent meta-analysis looking at 56 controlled trials as well as in a recent Cochrane Collaboration review. However, barriers exist to the implementation of IBA in routine practice within the AAU, including the perceived complexity and chaotic nature of admission units. There is also little information available on how to implement IBA in routine care in the acute medical setting.7,11 We sought to evaluate the success of embedding IBA in the routine assessment of all patients in the AAU.
Methods
Setting
This study was conducted over an 18-month period from April 2010 to September 2011 on an AAU at Chelsea and Westminster Hospital. Patients, over 18 years of age, are admitted either as an emergency through the ED or as a direct specialty referral to the AAU. The AAU is a 42-bed unit that accepts all specialty admissions and has nine high dependency beds. The AAU team comprises a Consultant general physician supported by junior doctors, involved in a patient's admission from the start and, provided they receive the right training, offer a multicontact resource in the holistic care of a patient.
Selection of an IBA intervention
An important consideration for selection of the screening tool in this study, from the array of available screening tools, was the ability of the tool to detect low risk’ and ‘at risk’ or heavy drinking behaviour as well as its validity in an acute medical setting. The Alcohol Use Disorders Identification Test (AUDIT), an alcohol screening tool, was originally designed by the World Health Organization to be used in the primary care setting.14,15 AUDIT has been shown to be effective in identifying patients likely to demonstrate current low-risk drinking behaviour as well as the more serious heavy drinking behaviour (where secondary alcohol-related problems have developed). 16 The AUDIT tool has also been validated in the acute medical setting. 17
The AUDIT-C (Alcohol Use Disorders Identification Test – Consumption) comprising only three questions has been found to be as effective as the 10-question AUDIT as a screening tool for hazardous and harmful drinking or dependence. 18 A limitation of the full AUDIT is the length and time required to complete the assessment and, with this in mind, the AUDIT-C was chosen as the screening intervention. A positive result using the AUDIT-C, which is a score greater than five, should result in the delivery of brief advice by the admitting clinician and onward referral to the AHW for brief intervention. The brief advice delivered by the junior doctors consisted of a short conversation with the patient structured against the FRAMES (Feedback, Responsibility, Advice, Menu of options, Empathy and Self Efficacy) approach recommended by NICE. 5
Implementation of IBA intervention using quality improvement methodology
Quality improvement (QI) techniques are increasingly being recommended for implementing change within healthcare organizations by institutions such as the NHS Institute for Innovation and Improvement in the UK and the Institute of Healthcare Improvement in the USA. Quality improvement techniques are intended to help iteratively guide the implementation of an intervention within a complex and unpredictable local setting in a practical and sustainable way.19,20 The implementation of IBA in the AAU was undertaken by a team including a Gastroenterology specialist registrar, an AHW, a Hepatology Consultant, an Addictions Psychiatrist and members (authors) of the NIHR CLAHRC for Northwest London, a quality improvement programme. The team was initially provided with training on QI methodologies using the ‘model for improvement’ as a central tool. 21 Subsequent quarterly and ad-hoc training took place over the 18-month duration of the project, which included training on the practical application of quality improvement tools, as well as on-going analytical support reviewing weekly data collection.
Delivery of an IBA intervention
All patients admitted to the AAU are clerked in by a junior doctor using a specific clerking pro forma to guide them through the medical history. Following discussions between the implementation team and the AAU consultant, the pro forma was modified to include the three AUDIT-C questions as part of the patient's medical history, an opportunity to record the score for each question and whether the patient was provided with brief advice from the junior doctor and referred to the AHW, where appropriate. Developing the infrastructure to deliver the intervention was followed by planned educational sessions to raise awareness of the use of the AUDIT-C and how to deliver brief advice and onward referral.
Eligibility for screening
All medical patients admitted to the AAU were eligible to be screened using AUDIT-C; any patients unable to give a history either through language barriers or due to illness were excluded.
Measuring for improvement
The uptake of the AUDIT-C screening tool by the junior doctors was assessed and monitored through weekly data collection, to demonstrate the effectiveness of training sessions in encouraging use of the tool. Approximately 140 patients are admitted via the AAU each week and it was deemed too resource intensive to audit all patients, so a convenience sample of 20 patients’ notes were assessed each week. Twenty patients’ notes were selected from those available on the unit on the day of sampling. Information about the completion of AUDIT-C was recorded from each of the 20 patients’ notes. The sample data were analysed weekly using Statistical Process Control, which is capable of using a relatively small sample to identify a detectable change in the processes associated with the delivery of educational sessions to increase the use of the AUDIT-C tool. 22
Results
Implementation of the AUDIT-C screening tool
The IBA intervention was initiated in August 2010 and data were subsequently collected for 55 out of the 60 weeks (406 days) until September 2011. The data were analysed on a weekly basis by generating time series run charts (Figures 1 and 2). The run chart was cross-referenced to the date of the various educational sessions with a view to associating specific training activities with improved uptake of the screening tool (Figures 1 and 2).
Percentage of eligible patients screened using the AUDIT-C tool over the duration of data collection period (August 2009 to September 2011). The start of data collection coincides with the introduction of routine screening using the AUDIT-C on the acute assessment unit. The delivery of specific educational sessions is indicated by arrows; C refers to specific junior doctor or registrar/consultant training; D refers to AAU team training. A significant amount of variation was observed throughout the data collection period as indicated by the low lower natural process limits (31.1) and high upper natural process limits (1 09, not shown on chart). Event A indicates a rule break-seven points above the mean line; Event B indicates a special cause variation – a point outside the upper or lower limits.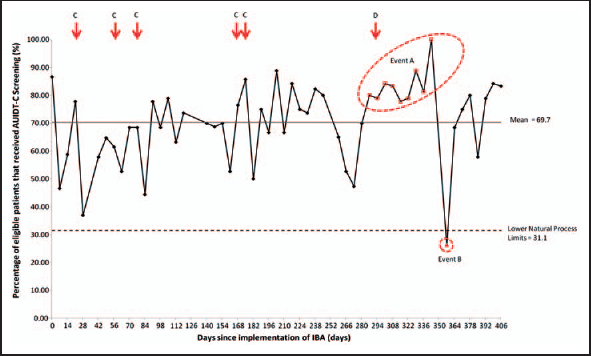
A detectable change in the process of screening eligible patients using the AUDIT-C tool over the duration of data collection period (August 2009 to September 2011). The start of data collection coincides with the introduction of routine screening using the AUDIT-C on the acute assessment unit. The delivery of specific educational sessions is indicated by arrows; C refers to specific junior doctor or registrar/consultant training; D refers to AAU team training. As previously demonstrated a break in the rules of run, i.e. seven data points above the mean line, occurred at day 287. The chart shows an increase in the mean percentage of patients screened from 67.3% to 80.1% between day 0–280 and 280–406, respectively.
Using the concept of plan-do-study-act (PDSA) cycles linked to the data collection, educational sessions were delivered to different healthcare professionals and their effect on the uptake of the screening tool monitored. Weekly analysis of the data, shown in Figure 1, initially demonstrated little impact of the training session on the screening of patients. This evidence led to the delivery of training to different audiences (labelled C in Figures 1 and 2), including consultants and registrars, as well as junior doctors and included the wider AAU team (labelled D in Figures 1 and 2). The AAU training, which targeted the specific junior doctors who admitted patients to the AAU, rather than generic training to all junior and senior doctors which had taken place prior to this, resulted in a detectable change in the process at day 287. This detectable change in process is indicated by a run of nine data points above the average (mean) line of the dataset and fulfils one of the rules of Statistical Process Control (i.e. a run of more than seven consecutive data points above or below the mean) and suggests a change in the process (Event A). This positive change was shortly followed by special cause variation, a data point outside of the lower limits of the run chart at day 357 (Event B) when junior doctors rotated. This is often associated with a reduction in performance. 23 Nonetheless, with a rule break, a change in process has occurred and the process is re-calculated, as shown in Figure 2, demonstrating a change in the mean percentage of patients screened during the different time periods from 67.3% to 80.1%.
Discussion
Strategies for quality improvement/change
Our study has shown that the incorporation of the AUDIT-C tool into an admission document has been well accepted by the junior doctors, with an average of 80% of patients sampled screened using the tool. The regular educational sessions maintained the moderately high level of patients being screened. The largest change in the junior doctors’ performance of alcohol screening was following the targeted educational session of the AAU team, specifically comprising junior doctors involved in admitting patients and other clinical support staff. This finding supports the observations of previous authors in the effectiveness of teaching staff where patients present. 13 The implementation of this method for training junior doctors (and subsequent effectiveness as demonstrated by the data in Figure 2) has led to alcohol educational session being embedded in their AAU training. However, inclusion of the AUDIT-C in the pro forma will not guarantee the completion of the screening tool without continued support through educational sessions.
The use of Statistical Process Control to detect valuable changes in a process, namely the proportion of patients being screened using the AUDIT-C, has provided an opportunity to improve the delivery of an intervention considering the complexity of the infrastructure and healthcare setting.
Strengths and weakness
The study demonstrates the ability to routinely collect data to indicate the relative success, or not, of the implementation of an intervention delivered in the acute medical setting. Timely collection and analysis of data to demonstrate improvement, a fundamental requirement of quality improvement, can often pose a challenge in a range of clinical settings. The collection of these data has limitations in terms of the inferences that can be drawn, especially relating to the effectiveness of such an intervention, and therefore should either be limited to evidenced interventions such as the AUDIT-C, or requires further robust data collection, due to the potential bias of the convenience sample collection. Only data relating to the process of screening were available for analysis. No data were available on the delivery of the brief advice component of the intervention or subsequent referral to support services, again affecting our ability to draw conclusions about the effectiveness of the intervention per se.
Lessons and messages
Many studies have demonstrated the frequency of alcohol problems amongst patients in hospital wards.1–3,6 These patients, who are often admitted with problems not related to their alcohol use, do not usually require specialist treatment by hepatologist or gastroenterologists and may miss an opportunity to have their alcohol use addressed.
The benefit of multi-contact BA in primary care has been demonstrated as an effective public health strategy. 24 The public health white paper ‘Healthy Lives, Healthy People’ (2010) advocates ‘a more innovative, integrated and dynamic approach to improving public health.’ 25
Admission to hospital provides patients with time, access to multi-disciplinary teams and the opportunity for a period of reflection. As a result, secondary care has the potential to play a key role in the public health strategy against alcohol. Currently, training in IBA is being focused on primary care and the ED but changes within the patient pathway, following the introduction of the four-hour wait target in England, means that patients are often moved through the ED rapidly to be assessed and discharged from assessment units.
Introducing the AUDIT-C into the AAU admission document offers an easy structured way for junior doctors to perform screening on every patient for hazardous, or low-risk, alcohol consumption. The current training of junior doctors necessitates their frequent rotations through different specialties with many junior doctors only spending three or four months on an AAU. This can be challenging when introducing improvements to a clinical area. Targeted teaching of clinical staff involved in admitting patients appears to be the most effective method in improving IBA by junior doctors and will help to sustain this strategy over the junior doctor rotations.
Approximately 7000 new doctors qualify annually in the UK and there is a lack of confidence in providing IBA that reflects a deficit in training. Although no analysis was undertaken of the delivery of the brief advice component of the intervention, many junior doctors involved in this study reported a lack of confidence in providing brief advice, even when a screening suggested it was necessary. These doctors, through their roles on the AAU, represent an ideal opportunity to tackle the increasing problem of drinking in patients admitted to hospital. This study highlights the benefits that can be gained from ongoing training in this group of individuals with the aim of reproducing the potential benefits in subsequent specialties that they rotate through. 26 Future studies are planned to see if these gains can be maintained over the longer term.
Footnotes
Acknowledgements
The authors thank AAU Medical and Nursing Team at Chelsea and Westminster Hospital; Dr Thomas Woodcock, Cathal Doyle and Professor Derek Bell, NIHR CLAHRC for Northwest London; and Professor Azeem Majeed and Dr Chris Millet, Department of Primary Care and Public Health, Imperial College London.