
Abstract
DECLARATIONS
None declared
None declared
Written informed consent was obtained from the patient for publication of the
EK
AK and EK performed the surgery and drafted the paper. VN performed a literature search and provided the images. GV drafted and revised the paper.
Accessory parotid gland tumours are rare and should be included in the differential diagnosis of neoplasms in the midcheek region.
Case presentation
A 56-year-old man presented to the outpatient clinic of a tertiary referral center with a painless mass in the left midcheek region. The patient reported that the mass appeared two years earlier with gradually increasing size. He had visited a general surgeon 14 months earlier and an open biopsy of the neoplasm had been performed. In the medical report, the histopathological diagnosis of a glomus tumour was made. Past medical history was unremarkable. The mass was lying subcutaneously in the left cheek, was hard on palpation and non-adherent to the surrounding tissues. Ipsilateral facial nerve function was normal.
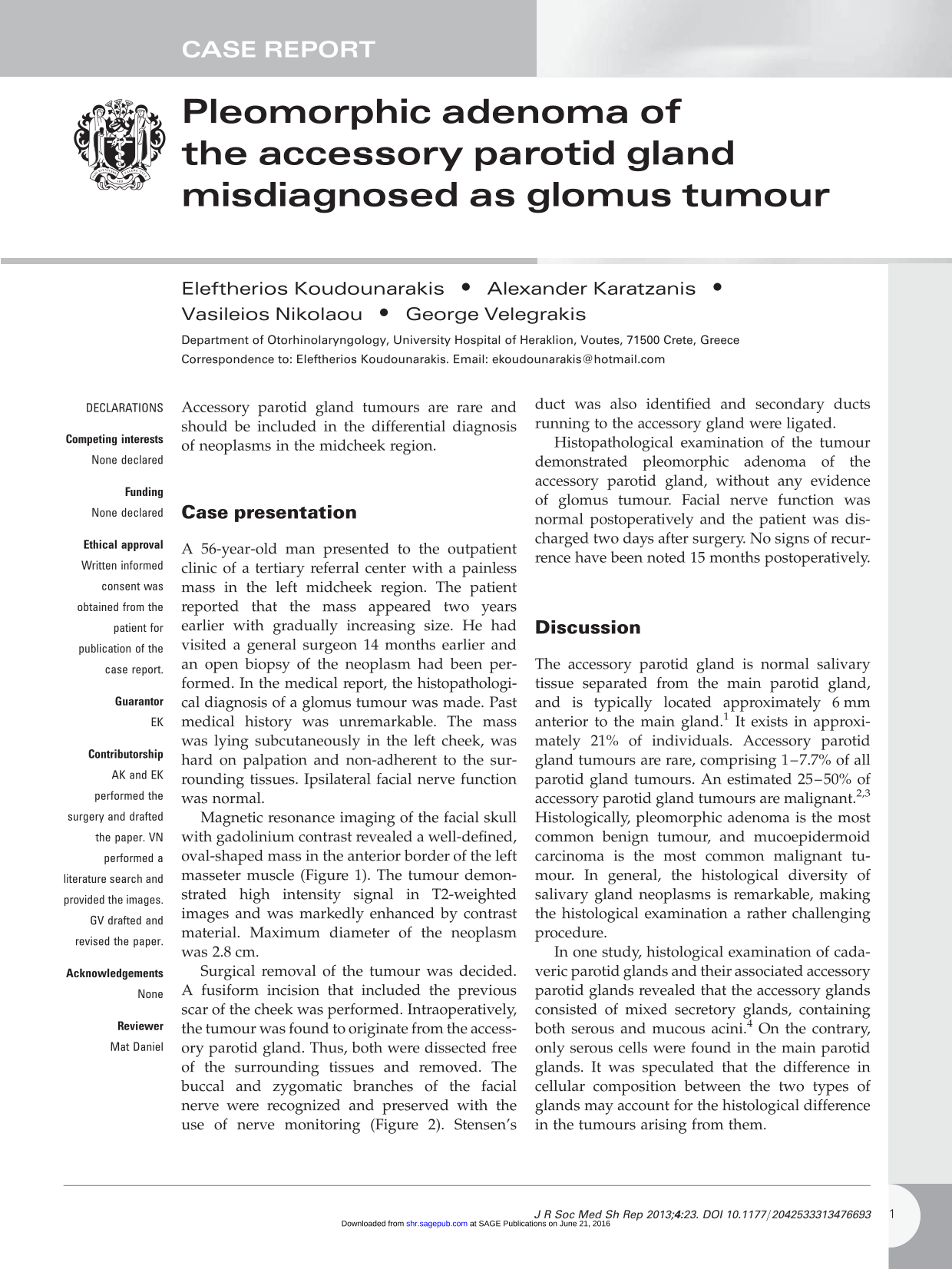
Magnetic resonance imaging of the facial skull with gadolinium contrast revealed a well-defined, oval-shaped mass in the anterior border of the left masseter muscle (Figure 1). The tumour demonstrated high intensity signal in T2-weighted images and was markedly enhanced by contrast material. Maximum diameter of the neoplasm was 2.8 cm.
Magnetic resonance imaging of the face demonstrating an oval-shaped mass in the left midcheek region
Surgical removal of the tumour was decided. A fusiform incision that included the previous scar of the cheek was performed. Intraoperatively, the tumour was found to originate from the accessory parotid gland. Thus, both were dissected free of the surrounding tissues and removed. The buccal and zygomatic branches of the facial nerve were recognized and preserved with the use of nerve monitoring (Figure 2). Stensen's duct was also identified and secondary ducts running to the accessory gland were ligated.
The tumour is exposed through a fusiform incision in the left cheek. The nerve stimulator (black probe) is used to identify the peripheral branches of the facial nerve
Histopathological examination of the tumour demonstrated pleomorphic adenoma of the accessory parotid gland, without any evidence of glomus tumour. Facial nerve function was normal postoperatively and the patient was discharged two days after surgery. No signs of recurrence have been noted 15 months postoperatively.
Discussion
The accessory parotid gland is normal salivary tissue separated from the main parotid gland, and is typically located approximately 6 mm anterior to the main gland. 1 It exists in approximately 21% of individuals. Accessory parotid gland tumours are rare, comprising 1–7.7% of all parotid gland tumours. An estimated 25–50% of accessory parotid gland tumours are malignant.2,3 Histologically, pleomorphic adenoma is the most common benign tumour, and mucoepidermoid carcinoma is the most common malignant tumour. In general, the histological diversity of salivary gland neoplasms is remarkable, making the histological examination a rather challenging procedure.
In one study, histological examination of cadaveric parotid glands and their associated accessory parotid glands revealed that the accessory glands consisted of mixed secretory glands, containing both serous and mucous acini. 4 On the contrary, only serous cells were found in the main parotid glands. It was speculated that the difference in cellular composition between the two types of glands may account for the histological difference in the tumours arising from them.
An accessory parotid-gland tumour usually presents as an asymptomatic cheek mass. The tumour is usually found at the midpoint of an imaginary line extending from the tragus to a point midway between the ala of the nose and the vermilion border of the upper lip. Proper preoperative evaluation includes a careful physical examination, diagnostic imaging and fine needle aspiration cytology. 5 Currently, the best imaging technique available for defining soft tissue lesions is magnetic resonance imaging with paramagnetic contrast material. With combined coronal and axial views, the nature of the lesion and its location can be readily differentiated from parotid gland and Stensen's duct lesions. 5
The role of open biopsy in cases of head and neck neoplasms is limited and is generally not included in the diagnostic work-up of salivary gland tumours due to its potential complications. These include facial nerve damage, haematoma, fistula formation and tumour seeding. 6 In the case of pleomorphic adenoma, violation of the tumour pseudocapsule leads to high recurrence rates, even if the tumour is totally resected after the open biopsy. Thus, definitive treatment with total excision of the tumour at first surgery is preferable in salivary gland neoplasms. 7
Fine needle aspiration gives a more clearcut result in cases of cystic lesions. It can provide definitive data but can also seed malignant cells. 8 However, high sensitivity and specificity of fine needle aspiration cytology in salivary gland diseases has been demonstrated. 9 The differential diagnosis for midcheek soft-tissue neoplasms includes inclusion cysts, lymphadenopathy, hae-mangiomas, lipomas, neurofibromas, schwanno-mas, neurilemmomas, fibromas, metastasis of malignancies and sialocoeles. 10
In the case presented here, a detailed pathology report of the first biopsy was not available. Thus, it was not possible to study the exact histopathological findings that led to the previous diagnosis of glomus tumour. Glomus tumour of the facial region is a very rare entity. 11 Pathological features of glomus tumours include glomus cells, vasculature and smooth muscle cells, whereas pleomorphic adenomas are composed of a mixture of epithelial, myoepithelial and stromal components. The stroma contains myxoid, condroid, fibroid and osteoid elements. Pleomorphic adenomas have no true capsule, but exhibit pseudopods. Immunohistochemistry aids in the differential diagnosis from pleomorphic adenomas, since the latter stain positively for epithelial markers, like the epithelial membrane antigen. 12 The mesenchymal areas stain with S100 and actin. On the other hand, the immunohistochemical profile of glomus tumours includes positive staining for vimentin and muscle-specific actin. Immunostaining for desmin, myoglobin, S-100 protein, neurofilaments and factor VIII-related antigen is negative. 12
Surgical resection is the treatment of choice for accessory parotid gland tumours. Three surgical approaches have been described: an incision in the cheek overlying the tumour, a peroral approach and a standard preauricular incision. 10 Among these approaches, the preauricular incision provides sufficient exposure for dissection of the facial nerve and excision of the accessory parotid gland. However, the wound is larger than that of the other two procedures. In the case of our patient, an incision in the cheek was preferred because of the previous open biopsy, removing simultaneously the scar of the skin, while the use of nerve monitoring provided sufficient identification of the peripheral branches of the facial nerve.
Recurrence rates after removal of accessory parotid gland tumours are low, even in cases of malignancy, ranging from zero to 9%.3,13
Footnotes
Acknowledgements
None