
Abstract
Objectives
To investigate the importance of incorporating secondary care input to aid commissioning following National Health Service reforms which will see the replacement of Primary Care Trusts with Clinical Commissioning Groups; to determine barriers that might arise given that this issue had been raised during public consultations and to explore ways to improve this input.
Design
Qualitative project with semistructured one-to-one interviews which were audio recorded, transcribed and analysed using thematic content analysis by two investigators. The findings were discussed and organized into a framework.
Setting
Bradford and Airedale, UK.
Participants
We interviewed 19 participants from primary care, the medical directorship and a range of specialties.
Main outcome measures
One-to-one semistructured interviews allowed a flexible dialogue to discuss planned questions and any other themes which participants brought up. This elicited a variety of experiences and ideas which provided the basis for in depth theoretical analysis required for our objectives.
Results
There was an almost universal agreement that the integration of secondary care advice is important in commissioning. The main perceived barriers were obstacles to good communication and relationships, conflicts of interest and financial pressures. Participants suggested varied and innovative ways to improve communication and integration, and suggestions for organisations.
Conclusions
Our results support the importance of secondary care input and highlight communication, organisation and integration as three goals for organisations to work towards. Successful achievement of these objectives could have financial implications for organisations as well as benefits for patient care.
DECLARATIONS
All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: GF is employed by NHS Airedale, Bradford and Leeds, an organisation for which the reforms may have implications; no other relationships or activities that could appear to have influenced the submitted work
YJN received a grant from the University of Leeds School of Medicine Thorpe Awards in Forensic Medicine and Public Health; this funder had no other involvement. No other funding
The project was deemed to be a service evaluation by NHS Research and Development. It then received ethical approval from the joint Health Sciences Leeds Institute for Genetics, Health and Therapeutics (LIGHT) and Leeds Institute of Molecular Medicine (LIMM) research ethics committee (HSLTLM/10/030)
GF
All authors designed the study. YJN designed the interview questions, carried out the interviews, transcribed the electronic records, analysed the data, drafted and revised the paper. CA analysed the data, drafted and revised the paper. GF acted as a gatekeeper, validated the interview questions, and helped to draft and revise the paper
Yannis Pappas
Introduction
The Health and Social Care Bill 1 which has been passed by the United Kingdom Parliament will see the abolition of Primary Care Trusts (PCTs) in the National Health Service (NHS). These organisations are currently responsible for commissioning services in the NHS, a complex role which involves purchasing services for a population and responsibility for the appropriate use of funds. 2 Commissioning will be taken over by Clinical Commissioning Groups comprised of general practitioners (GPs) alongside a nurse and specialist from another geographical area.
Public consultations have highlighted the integration of secondary care advice as an area requiring further clarification and amendment. 3 It is expected that organisations called Clinical Senates and Clinical Networks will provide specialist input from the broader base of secondary care clinicians in their geographical area. Yet how these bodies will work has not been fully explained 4 and these bodies will probably not be the sole means of integrating secondary care advice.
We carried out a qualitative survey-based service evaluation in the Bradford and Airedale area to provide further information about professionals’ opinions of the importance of seeking secondary care advice, the barriers that might arise as well as potential solutions to overcome these barriers.
Methods
Sampling and setting
We used purposive sampling to select the individuals most likely to provide relevant information to achieve our aims. 5 GF, a public health consultant from NHS Airedale, Bradford and Leeds acted as the gatekeeper, which involved suggesting potential participants and facilitating access to these individuals. 6 We selected 31 professionals from primary care, secondary care and the medical directorship as we felt that this spread of stakeholders would allow triangulation of perceptions from different participants 7 to provide a more cohesive understanding of the topic and increase the validity of the study. As far as possible we tried to recruit similar proportions from each group. Potential interviewees were sent an approach email containing an information sheet explaining the project.
Data collection
We chose one-to-one interviews to obtain in-depth opinions from participants. 8 We developed an interview question schedule (Appendix A) using open-ended questions to elicit as much information as possible. We validated the questions through discussion with consultants in public health and submitted them for review by an ethics committee. We then sent the schedule to potential participants before interviews.
Interviews were carried out by YJN. He used a neutral reflective style throughout the interviews to minimize interviewer bias. 8 Participants were invited to read the information sheet and ask questions. This was done to ensure that informed consent was obtained; this was recorded on consent forms. The semistructured interviews were done in NHS sites in the region, lasted up to 45 min, and were recorded electronically. The recorded interviews were transcribed and given anonymized identifier codes to maintain confidentiality (GP for general practitioners, Sec for secondary care consultants, Pub for public health consultants and Dir for all others).
Data analysis
We used thematic content analysis to analyse the data. 9 To improve the robustness of our analysis, two investigators (YJN and CA) independently read and coded the interview transcripts, developing the codes directly from the transcripts. After discussion to agree on a coding frame and reading for missed codes, the investigators organized the codes into broader themes. Analysis was completed when no further codes or themes were identified from the data. A draft of this report was sent to participants for feedback. Several participants validated the findings. The code categories developed from the data are included in tables with relevant quotes to demonstrate examples of opinions from our participants.
Results
Participant demographics
We interviewed 19 participants out of the 31 approached. Most of the secondary care consultants and members of the medical directorship we approached took part. GPs were proportionally the least likely to participate. Non-participants often cited a lack of availability within the interview period of the project.
Participants described having various responsibilities relating to commissioning and several described two distinct roles. GPs and secondary care consultants mainly worked in their respective sectors with differing levels of involvement in commissioning activities. Two GPs were also PCT clinical leads, a responsibility which involved advising the PCT through regular meetings and actively developing pathways of care. Medical directors, managers and professionals from commissioning and contracting had all been directly involved in the process of commissioning. Public health consultants had experience advising commissioners.
Importance of secondary care input to aid commissioning
Participants were in almost universal agreement that secondary care input is important (Table 1). Adjectives such as ‘crucial’, ‘vital’ and ‘fundamental’ were frequently used. The other participants either did not give a clear indication of their opinion either way or disagreed by saying that specialist input might not be of benefit in cases where commissioners already possessed secondary care knowledge. From the interviews and the analysis we felt that secondary care clinicians were keen to be involved in commissioning and felt disgruntled at their perceived low level of involvement.
Stated reasons why secondary care input is important

A major theme that emerged from the interviews was that secondary care consultants possess certain attributes which make it more desirable to involve them in the commissioning process. Specialists were described as having ‘expert knowledge’ that could be beneficial and as being key stakeholders in patients’ care. Secondary care consultants were also seen to have good knowledge of local services.
Another theme that emerged was that secondary care input is important to improve the cooperation of the system as a whole. Involvement of specialists was seen to hold potential for streamlining of services, and for improving general understanding of professional roles and pathways.
Interviewees also gave ‘other’ reasons for involving specialists. Secondary care was perceived to be important to help good pathway design, and there was a general feeling that pathways can be helpful in providing coordinated effective care. Participants also said that secondary care input leads to more cost-effective care and better models of care, and that it can improve the quality of referrals to secondary care.
Several interviewees gave a potential reason not to involve secondary care. Some pointed out that conflicts of interest might arise when asking secondary care providers to advise on commissioning because their advice might be influenced by financial interests. The commissioner who disagreed with the importance of secondary care involvement further explained it might be a waste of clinicians’ time.
Barriers to successful involvement of secondary care
There was a general agreement that communication and relationships between primary and secondary care could cause problems (Table 2). Engagement between Clinical Commissioning Groups and secondary care clinicians was seen to be potentially troublesome. Participants felt that this could arise due to a lack of skill or staff affecting the capacity of commissioners. Others perceived a lack of willingness on the part of secondary care or GPs. Several interviewees pointed to poor existing relationships between primary and secondary care and a few felt that there was a poor perception of secondary care within primary care.
Main potential barriers to the integration of secondary care advice

Participants mentioned time constraints as a potential barrier. It was felt that a lack of time on the part of GPs and secondary care consultants could hinder the successful development of the commissioning groups and informal networks.
Potential conflicts of interest were mentioned by many participants. The main type mentioned related to different organisations having conflicting priorities and agendas. Interviewees also mentioned that conflicts might arise if professionals from different sectors had different views on the best course of action. The last type mentioned was conflicts of a personal nature, for example, if individuals were involved in discussions regarding the closure of their service. While several participants felt that including a specialist from another geographical area on a Clinical Commissioning Group would reduce the risk of conflicts of interest, one participant felt that these conflicts might still arise if the consultant worked for a provider with financial interests in the same area.
There was a common perception that financial pressures might present a barrier. These included the need to achieve efficiency savings and the requirement for Foundation Trusts, recently created from local hospital trusts, to be financially viable.
Interviewees mentioned organisational barriers that may present, for example, due to a lack of clarity and consistency of job roles, and redundancy programmes and their effect on staff morale.
‘Other’ barriers mentioned included the uncertainty regarding the exact changes and their implementation and the potential fragmentation of services which might make it more difficult for different services to work closely. A few participants also felt that the single specialist or nurse on each Clinical Commissioning Group would offer a very narrow representation of secondary care and that providers that do not have representatives may not be involved in discussions.
Possible solutions to help integrate secondary care advice
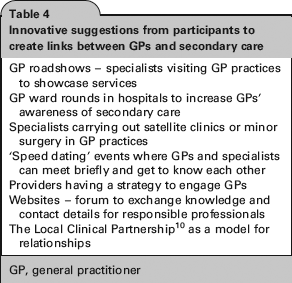
In response to the main potential barriers mentioned most participants felt that communication and relationships will be important following the reforms (Table 3). Good communication between commissioners and providers was mentioned as particularly beneficial. Many methods were suggested to achieve good communication such as regular meetings, smaller focus groups that would be easier to arrange and involve only those specifically required, and informal networks whereby clinicians on the ground can share information. Several participants mentioned innovative ways of creating links between GPs and secondary care to improve the relationship between these groups (see Table 4). Some participants highlighted the importance of having an open and honest dialogue and others believed harnessing the enthusiasm in secondary care could be beneficial.
Main solutions proposed

GP, general practitioner
Innovative suggestions from participants to create links between GPs and secondary care
GP, general practitioner
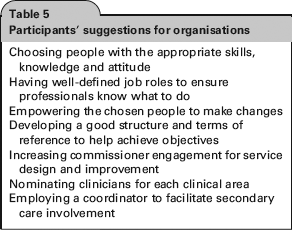
Interviewees gave various solutions for organisations to improve the integration of secondary care advice (Table 5). Several talked about having the ‘right people’ working within the organisation; those who are able and willing to make things work and who were empowered to do so. Others felt it was important to be clear about job roles. A few interviewees pointed to the importance of structure and of clear terms of reference so that organisations are equipped to deal with their organisational priorities. One interviewee suggested that it might be useful to have someone whose role it is to coordinate the processes around seeking secondary care advice.
Participants’ suggestions for organisations
Another theme was the need for the integration of health-care services. It was felt that better cooperation between primary and secondary care could be of benefit. Greater involvement of clinicians was seen to be desirable to ensure that sectors work together as a unit. The whole health economy was described as having shared objectives and as such it was suggested that all sectors should take joint responsibility for the provision of health-care services. Another interesting suggestion involved changing services from a location-based model to a more flexible one where teams work from different sites to achieve their goals. One interviewee pointed to Torbay Care Trust and Birmingham East and North PCT as examples where integration has been tried successfully.
We found a perception that a culture change is required. This included commissioning with ‘vision’ to help design services which could achieve the desired outcomes, and having a patient-centred approach to ensure the service responds to the needs of patients.
Several participants spoke about time as a solution. This could be time given to clinicians in their working week to take on responsibilities related to commissioning, time for commissioners to understand pathways of care or for GP commissioners to develop their skills. It was also said that time is needed for the development of trusting working relationships and to allow the changes to settle down.
Leadership was perceived to be desirable, whether that be clinical, managerial or political. A similar number of participants felt that good pathways would be beneficial. Some explained that a pathway for all sectors would help the different parts of the service work effectively together. Participants also felt that more information about the planned reforms would be useful to help professionals and organisations prepare.
Discussion
Our findings support the importance of secondary care expertise to aid commissioning. They also identify potential obstacles relating to communication, integration and organisation and provide tangible ideas to resolve these difficulties.
Strengths
Our project provided insight into a topic which had previously been highlighted but not investigated. Interviews provided information from a range of perspectives which makes it likely that we elicited a balanced view of professionals’ perceptions. Almost all of the interviewees had relevant experience of commissioning, and may thus have had a clear view of what is needed. Our findings reveal a current and important idea of the views of the professionals who will be affected by the changes to the commissioning process. Innovative suggestions by participants are of particular interest in further developing commissioning in the area.
Limitations
Our findings reflect the views of professionals in the Bradford and Airedale area and thus cannot be generalized to all health-care professionals. The project was student-led and as such was limited by financial, personnel and time constraints. With a response rate of 61%, our sample was not large enough for data saturation to be reached given the complex nature of the issues being studied. It is therefore possible that other stakeholders in the area may have held different views. The small sample size and the fact that most had some previous experience of dealing with the PCT might also affect the representativeness of the sample. The level of knowledge regarding the reforms varied between participants and responses sometimes included out-of-date information.
Link to the evidence
There is some evidence to support the interviewees’ perceptions that secondary care input is important to aid commissioning. A qualitative study found that primary care organisations in which managers work alongside doctors from both primary and secondary care can better develop their service than other organisations in which this engagement is not present. 11 Another paper highlighted the importance of specialists being involved for good service provision. 12 The importance of secondary care involvement is also shown in evidence from Kaiser Permanente, an integrated health-care group in the USA where clinicians from all clinical areas hold joint responsibility for their budgets and service with better outcomes and cost-effectiveness than the NHS.13, 14
This evidence from Kaiser Permanente also supports the view that integration may improve services in the NHS. Torbay Care Trust and Birmingham East and North PCT are examples where integration and cooperation have so far provided good results.15, 16 The evidence from these two areas also supports the perceived importance of communication and relationships as the reports highlight relationships as being crucial to the development of successful integrated systems.
Scott et al. 17 carried out a literature review and found that changes in culture have the potential to effect more general improvements in health care. The authors further point to the importance of leadership in achieving this change in culture. These issues were also raised by the interviewees in our project. However, the review concludes that changes in culture may be difficult to bring about.
Implications
Given the opinions and evidence supporting the importance of secondary care input, we feel that it is crucial for organisations to take measures to maximize the involvement of specialists. With efficiency savings of £20 billion needed in the NHS before 2015, 18 the perception among participants that secondary care involvement can improve cost-effectiveness is of particular interest.
Our findings highlight communication, organisation and integration as three clear goals that organisations can work towards. We suggest that organisations implement participants’ innovative suggestions to improve communication (Table 4) and the steps that organisations can take to improve secondary care input (Table 5). To achieve better integration, the suggestion to use the Local Clinical Partnership 10 as a model for the interaction between GPs and specialists is particularly interesting. This model suggests joint responsibility for improving care, which could reduce the potential conflict of interest by aligning objectives. We suggest that the feasibility of this model requires further research.
We suggest that organisations should try and bring about a change in their culture, for example, through training and implementing organisational processes which favour a positive working culture. For example, we feel that professionals are more likely to engage if they feel their views are being listened to. As such organisations can take steps to encourage greater involvement of stakeholders through meetings and discussions.
It is important to note that the organisational conflicts of interest mentioned are made possible by the purchaser–provider split, which results in primary and secondary care having different agendas. 19 This system was introduced in the 1990s and will remain in place after the reforms. 19 Increasing integration and alignment of objectives across sectors could decrease the potential for conflict.
For the future
Further work is required to investigate how secondary care advice will best be integrated following the reforms. This could be on a national level or a more local one. To resolve the lack of information, we suggest that professionals and organisations take the lead in discussions to explore the issue further. Organisations could set up committees with the specific responsibility of looking into secondary care engagement to provide further clarification.
Footnotes
Acknowledgements
The authors would like to thank the Public Health team at Bradford and Airedale and all participants. Special thanks to Judith Forrest, Mathew Stone and Paul Carder
Appendix A
Interview questions
Please could you describe your current role in the NHS?
What is your current role in commissioning or advising the commissioning of healthcare services?
How important is it that secondary care expertise be sought to aid primary care commissioning?
What is your understanding of the current way in which secondary care advice is sought to aid commissioning?
What is your understanding of the proposed changes to the NHS?
In your opinion, are there any barriers to the integration of secondary care expertise that might arise with the new model of commissioning?
How do you think these barriers might be overcome?
Are there any other ways in which you think the process might be improved?