
Abstract
DECLARATIONS
None declared
None declared
Written informed consent to publish the article was obtained from the patient or next of kin
LL
LL wrote and edited manuscript including literature review. SE: treating physician and helped in preparation of manuscript. MT: histopathologist and helped in preparation of manuscript
This case examines two synchronous tumours and the importance of investigating for dual diagnosis when presented with atypical disease distribution.
Case report
A 55-year-old man with known chronic obstructive pulmonary disease, hypertension and a 40-pack-a-year smoking history, presented to the cardiology clinic with exertional dyspnoea. Examination revealed a raised jugular venous pressure, systolic murmur and peripheral oedema. Severe tricuspid regurgitation was confirmed on echocardiogram. Spirometry showed an FEV1 of 41%.
Five years later he was referred to the colorectal surgeons with a two-year history of intermittent diarrhoea 6–7 times per day, two stone weight loss and a 5 cm craggy liver edge. He denied flushing or night sweats.
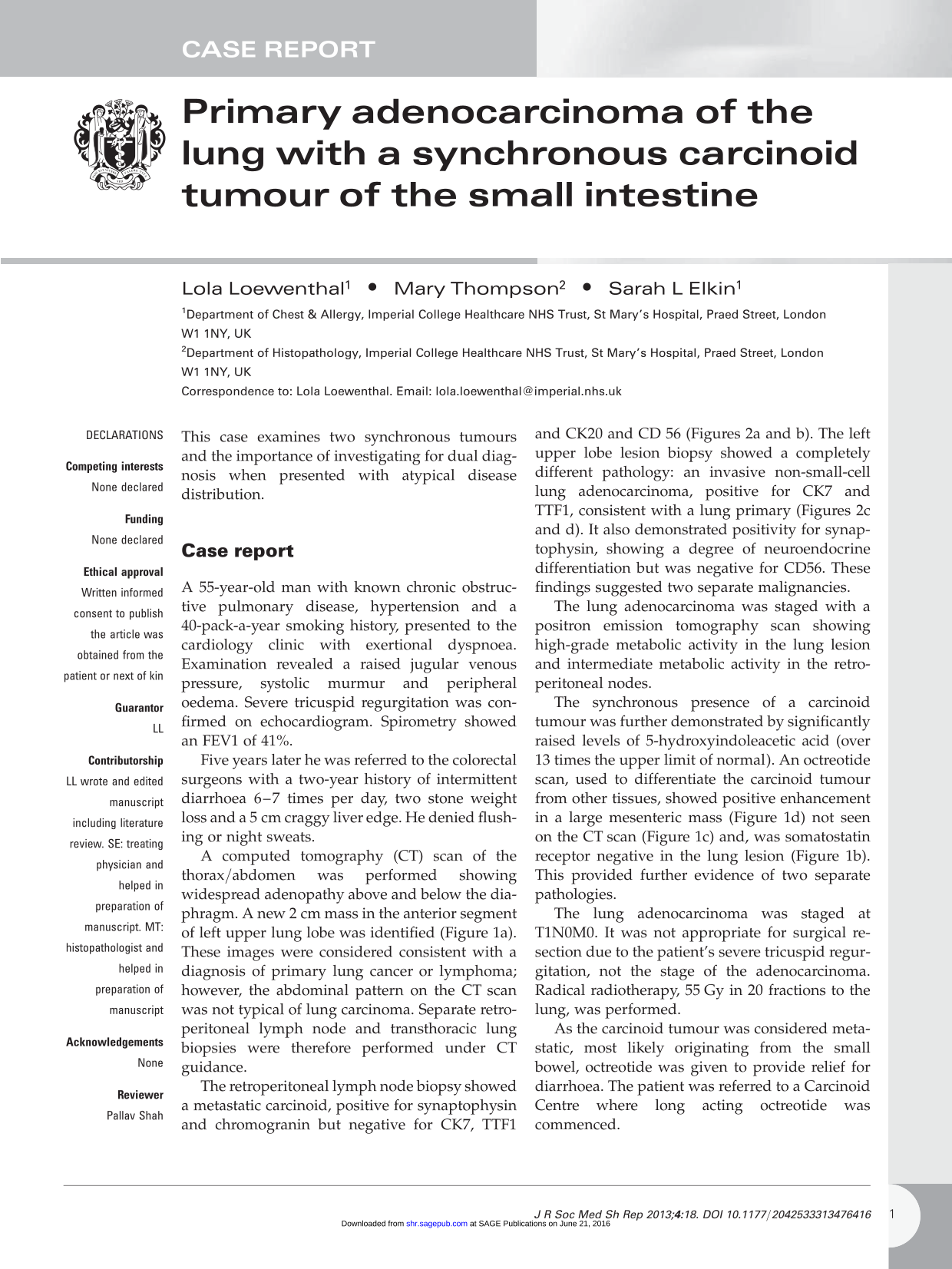
A computed tomography (CT) scan of the thorax/abdomen was performed showing widespread adenopathy above and below the diaphragm. A new 2 cm mass in the anterior segment of left upper lung lobe was identified (Figure 1a). These images were considered consistent with a diagnosis of primary lung cancer or lymphoma; however, the abdominal pattern on the CT scan was not typical of lung carcinoma. Separate retroperitoneal lymph node and transthoracic lung biopsies were therefore performed under CT guidance.
Computed tomography and octreotide scans showing the lung and mesenteric masses: a Computed tomography scan showing the 2 cm left upper lobe lung mass (arrow) b Octreotide scan showing the lung lesion to be somatostatin receptor negative (arrow). c Computed tomography scan showing the mesenteric nodal mass (cross) d Octreotide scan showing the mesenteric nodal to be somatostatin receptor positive (cross)
The retroperitoneal lymph node biopsy showed a metastatic carcinoid, positive for synaptophysin and chromogranin but negative for CK7, TTF1 and CK20 and CD 56 (Figures 2a and b). The left upper lobe lesion biopsy showed a completely different pathology: an invasive non-small-cell lung adenocarcinoma, positive for CK7 and TTF1, consistent with a lung primary (Figures 2c and d). It also demonstrated positivity for synaptophysin, showing a degree of neuroendocrine differentiation but was negative for CD56. These findings suggested two separate malignancies.
The lung adenocarcinoma was staged with a positron emission tomography scan showing high-grade metabolic activity in the lung lesion and intermediate metabolic activity in the retroperitoneal nodes.
The synchronous presence of a carcinoid tumour was further demonstrated by significantly raised levels of 5-hydroxyindoleacetic acid (over 13 times the upper limit of normal). An octreotide scan, used to differentiate the carcinoid tumour from other tissues, showed positive enhancement in a large mesenteric mass (Figure 1d) not seen on the CT scan (Figure 1c) and, was somatostatin receptor negative in the lung lesion (Figure 1b). This provided further evidence of two separate pathologies.
The lung adenocarcinoma was staged at T1N0M0. It was not appropriate for surgical resection due to the patient's severe tricuspid regurgitation, not the stage of the adenocarcinoma. Radical radiotherapy, 55 Gy in 20 fractions to the lung, was performed.
As the carcinoid tumour was considered metastatic, most likely originating from the small bowel, octreotide was given to provide relief for diarrhoea. The patient was referred to a Carcinoid Centre where long acting octreotide was commenced.
Discussion
While many synchronous tumours are seen there is a paucity of literature on the subject of it being necessary for the medic to be open to dual diagnosis.
This case highlights the importance of suspecting dual pathology in patients with lung cancer where the pattern of disease is atypical. Here, multiple enlarged mediastinal lymph nodes are commonly seen on radiological investigations for lung masses secondary to metastases. In this case the CT spread of disease was not typical for primary lung cancer. It was found that being open to dual diagnosis and not just accepting atypical metastatic spread allowed for appropriate investigations, including biopsies from multiple areas, and the patient's management to be appropriately tailored.
Carcinoid tumours are rare, with over 70% from the intestinal system.
1
By contrast adeno-carcinoma of the lung is a common malignancy, with 85% being non-small-cell lung cancer.
2
Carci-noid tumours have been shown to be associated with synchronous non-carcinoid tumours.
3
This is thought to be due to a combination of: genetic predisposition, failure of immunological surveillance and skewed observations reflecting the indolent growth pattern of carcinoid tumours.3,4
Biopsy results from the metastatic carcinoid and lung adenocarcinoma: a metastatic carcinoid, H&E b Metastatic carcinoid, immunostaining for TTF-1, c lung adenocarcinoma, H&E, d lung adenocarcinoma, immunostaining for TTF-1H&E, hematoxylineosin; TTF-1, thyroid transcription factor-1
However, while there would appear to be anecdotal evidence, this is the first reported case in the literature of adenocarcinoma of the lung occurring simultaneously with a carcinoid tumour outside of the lung.
Management of such synchronous tumours tends to focus on the carcinoma. The mean survival of stage T1N0M0 non-small-cell lung cancer is 13.7 months 5 with no intervention and a five–year survival rate of 19% with radical radiotherapy. 6 The prognosis of metastatic carcinoid tumour is determined by the site of the primary, histology and particularly the presence of carcinoid heart disease. Predicted five-year survival rate of small intestinal carcinoid is 76%. 7 The adenocarcinoma was therefore treated aggressively. Distinguishing between adenocarcinoma of the lung and synchronous tumours through imaging and multiple biopsies has allowed the patient to receive radical treatment for both conditions, where he may otherwise have been palliated.
In conclusion, to the best of our knowledge, this is the first time a small bowel carcinoid tumour in association with lung adenocarcinoma has been described in the literature. It highlights the importance of the multidisciplinary team being aware of synchronous cancers and investigating for them appropriately to allow the optimum treatment to be delivered.