
Abstract
Background:
Drug-related problems (DRPs) are a significant concern in hospitalized patients. In Ethiopia, DRPs occur at a rate of 9.2 per 100 admissions and 9.4 per 1,000 patient days; however, pediatric-specific data are limited.
Objective:
This study assessed the magnitude, types, and predictors of DRPs and evaluated the acceptability of pharmacist-led interventions in pediatric intensive care units (PICUs) in Northwest Ethiopia.
Design:
A multicenter prospective interventional study
Methods:
All pediatric patients admitted to the PICU during the study period were consecutively enrolled. The study was conducted from January 1, 2025 to March 31, 2025 across four specialized hospitals, resulting in a total of 394 participants. DRPs were identified through medical record reviews, caregiver interviews, and direct bedside assessment by a clinical pharmacist. Each DRP was classified according to the Pharmaceutical Care Network Europe (PCNE) classification system version 8.01. Binary logistic regression was performed to identify independent predictors of DRPs.
Results:
Of the patients, 251 (63.7%) experienced at least one DRP, with 522 DRPs identified (mean 1.3 ± 0.8 per patient). The dominant domains were treatment effectiveness (54.6%) and treatment safety (30.3%), and 97.7% were deemed preventable. Drug and dose selection were the main causes (46.0% and 43.8%, respectively). Independent predictors included age 29 days–1 year (AOR = 2.2, 95% CI: 1.0–4.8), polypharmacy (⩾5 medications; AOR = 1.7, 95% CI: 1.0–2.8), multiple prescribers (AOR = 1.8, 95% CI: 1.1–2.9), prolonged ICU stay (⩾10 days; AOR = 2.4, 95%CI: 1.2–4.7), circulatory system disease (AOR = 3.5, 95% CI: 1.4–9.0), the use of anti-infectives (AOR = 5.0, 95% CI: 2.0–13.7), and antiepileptics medications (AOR = 2.1, 95% CI: 1.0–4.3) were independent predictors of DRPs.
Conclusion:
DRPs were common in PICU but predominantly preventable. Despite a modest mean number of DRPs per patient, the type and causes identified indicate opportunities for optimizing medication use. Younger age, polypharmacy, multiple prescribers, prolonged PICU stays, circulatory system disease, and specific drug classes were independent predictors. The high acceptance and effectiveness of pharmacist-led interventions underscore their crucial role in improving medication safety and optimizing pharmacotherapy in resource-limited intensive care settings.
Plain language summary
Drug-related problems (DRPs) are common in hospitalized children and can affect treatment effectiveness or cause harm. In Ethiopia, little is known about how often these problems occur in pediatric intensive care units (PICUs). This study looked at 394 children admitted to PICUs in four hospitals in Northwest Ethiopia to find out how frequently DRPs occur, what types are most common, what factors increase the risk, and whether pharmacist-led interventions are helpful. We found that nearly two-thirds of the children (64%) experienced at least one DRP, most commonly related to treatment not working as expected or potential medication side effects. Almost all of these problems could have been prevented. Children younger than one year, those taking five or more medications, those with multiple doctors involved in their care, longer ICU stays, cardiovascular conditions, and those receiving antibiotics or antiepileptic medications were more likely to experience DRPs. Pharmacists proposed 687 interventions to address these problems, and over 80% were accepted by the care team, resolving most of the DRPs. These findings show that DRPs are frequent but largely preventable in critically ill children. Pharmacist involvement is highly effective in identifying and resolving these problems, helping to make medication use safer and more effective in pediatric intensive care, especially in resource-limited settings.
Keywords
Introduction
Drug-related problems (DRPs) are preventable events that occur during drug therapy and can negatively affect treatment effectiveness and patient outcomes. Over recent decades, DRPs have become a major global health concern, contributing to avoidable morbidity, mortality, and healthcare costs.1–4 Globally, more than half of all prescribed and dispensed medicines are used inappropriately. 5 In the United States alone, an estimated 98,000 deaths each year are attributed to preventable medication-related incidents. 6 Furthermore, DRP may occur at any stage of the medication-use process, including prescribing, dispensing, administration, and monitoring. This problem frequently manifests as clinical complaints, abnormal laboratory findings, or adverse drug reactions (ADRs).7,8
Pediatric patients are disproportionately vulnerable to DRP. Evidence indicated that children are nearly three times more likely than adults to experience medication-related harm. 9 This increased risk is associated with limited pediatric-specific drug safety data, inadequate availability of age-appropriate formulation, developmental pharmacokinetic variability, and high prevalence of off-label prescribing.10,11 The pediatric intensive care unit (PICU) is a particularly critical setting due to complex care needs and frequent use of high-risk medications.12–14 Reported DRP prevalence in this setting was extremely high, reaching up to 89.6% in the neonatal intensive care unit (NICU). 15 Multiple risk factors, such as younger age, polypharmacy, specific disease categories, prolonged hospitalization, and exposure to high-risk drug classes, have been identified,16–18 although finding remains inconsistent across studies.19,20
In Ethiopia, data on pediatric DRPs are scarce and largely limited to single-center, cross-sectional studies in general pediatric wards,20–22 where incidences have been reported at 9.2 per 100 admissions and 9.4 per 1000 patient days. 23 No prior study has comprehensively evaluated DRPs in the PICU setting. International evidence demonstrates that integrating a clinical pharmacist into the ICU team improves medication safety, reduces errors, and optimizes dosing practice. 24 In addition, pharmacist-led intervention is widely accepted and has yielded clinically meaningful benefits. 25 However, within the Ethiopian PICU context, the role and impact of clinical pharmacists on medication safety have not been systematically studied. Given the heightened risk among critically ill children to DRPs and limited local evidence, this interventional prospective study was therefore aimed (1) to determine the magnitude, types, and predictors of DRPs and (2) to evaluate the impact of pharmacist-led interventions in PICU in Northwest Ethiopia. The finding is expected to inform evidence-based strategies that pharmacist-led interventions could enhance medication safety in resource-limited pediatric critical care settings.
Methods
Study setting, design, and study period
A multicenter, prospective interventional study was conducted from 1 January 2025 to 31 March 2025 across four comprehensive specialized hospitals in Northwest Ethiopia: Debre Tabor Comprehensive Specialized Hospital, the University of Gondar Comprehensive Specialized Hospital, Tibebe Ghion Comprehensive Specialized Hospital, and Felege Hiwot Comprehensive Specialized Hospital. Collectively, these institutions serve an estimated population of more than 15 million people across the Amhara region. Eligible participants were prospectively followed from PICU admission to discharge, transfer, and death to monitor their clinical progress and identify DRPs. Guidelines from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) 23 checklist were followed in preparing this manuscript, and the completed checklist is provided as Table S1.
Study populations and eligibility criteria
The study population comprised all pediatric patients admitted to the PICU in the selected hospitals during the study period. Eligible participants include pediatric patients under 18 years old who were admitted to the PICU for more than 24 h and received at least one medication during the PICU stay. Patients were excluded if they were readmitted to the PICU during the study period, if parents or guardians refused consent, or if they were younger than 29 days admitted to the NICU as per hospital protocol.
Sample size and sampling techniques
Sample size was determined using the single-population proportion formula, 24 assuming a 50% prevalence of DRPs, a 5% margin of error, and a 95% confidence level. After adding a 10% contingency, the final estimated sample size was 422. Hospitals were allocated samples proportionally based on pediatric admissions recorded in the preceding 5 months, and consecutive sampling was employed. In total, 394 patients were included in the final analysis, with 28 excluded. A flow diagram is provided in Figure 1.

Diagrammatic representation of the sampling procedure at the PICUs in Northwest Ethiopia.
Study variables
The primary outcome of the study was the incidence of DRPs. Explanatory variables encompassed socio-demographic characteristics (age group, gender, health insurance status, residence, and nutritional status), clinical factors (presence of comorbidity, number of conditions, primary admission diagnosis, length of PICU stay, discharge outcome, and use of mechanical ventilation), and treatment-related factors (number of medications, therapeutic class, and number of prescribers).
Operational definitions
DRPs were defined and categorized according to the Pharmaceutical Care Network Europe (PCNE) classification. 25 Pediatric age groups categorized according to internationally accepted 129 classification: infants (1 month to 1 year), toddlers (>1 to ⩽3 years), preschool children (>3 to ⩽5 years), school-age children (>5 to ⩽10 years), and adolescents (>10 to <18 years). 26
Polypharmacy was defined as the concurrent use of ⩾5 medications. 27 Comorbidity defined as the presence of two or more medical conditions occurring simultaneously in a patient. 28
Study outcomes
Primary outcome: Proportion of patients with ⩾1 DRP.
Secondary outcomes:
DRP types and causes
Acceptance rate of interventions
DRP resolution
Preventability
Data collection tool and procedures
Data were collected using a structured, pretested abstraction tool adapted from previous DRP studies.1,16,29–31 The instrument captured demographic characteristics, clinical information, and medication-related variables. Medications were coded per Anatomical Therapeutic Chemical classification for drugs 32 and diagnoses per International Classification of Diseases (ICD-11). 33 Data were collected on-site at each hospital by one bachelor-level pharmacist, supervised by the senior pharmacist, with all pharmacists working concurrently across the four hospitals. Consistency and inter-rater reliability were ensured through a calibration exercise and double-coding of 10% of randomly selected records (Cohen’s κ ⩾0.82) every 72 h. Pharmacists did not engage in routine prescribing or general patient care.
DRP classification
DRPs were classified using the PCNE V8.01 system. 25 Although PCNE V9.1 is available, it was not adopted because its expanded subcategories and increased coding granularity require standardized electronic documentation, which is limited in our predominantly narrative and paper-based PICU records. Furthermore, V8.01 is routinely applied in our hospital, and pharmacists involved in this study were specifically trained in its use to ensure coding consistency. Importantly, the core PCNE domain, problem, cause, intervention, and outcome are stable across versions, ensuring V8.01 did not compromise detection of clinically relevant DRPs. Studies from similar resource-limited settings have also used PCNE V8.x, supporting comparability.34–37
Identification and evaluation of DRPs
DRPs were identified through a structured assessment comprising drug interaction, dosing accuracy, guideline adherence, and additional evidence-based safety checks. Drug–drug interactions (DDIs) were screened daily using UpToDate®, 38 and merely clinically significant interactions (categories C-X) were documented. ADR causality was determined using the Naranjo Probability Scale. 39 Dose appropriateness was evaluated using Ethiopian Standard Treatment Guidelines (2021), 40 WHO Pocketbook of Pediatric Hospital Care, 41 Nelson Textbook of Pediatrics 21st Ed, 42 and Harriet Lane Handbook, 22nd Ed, 43 considering age, weight, and organ function, applying a ±10% threshold for dosing errors. 44 Evaluation also comprised assessment of guideline adherence, contraindications, therapeutic duplication, antimicrobial spectrum, IV compatibility, and monitoring for high-risk medications. To ensure categorical coherence, all DRPs were classified according to PCNE categories, with ADRs, DDIs, and dosing errors mapped to their respective domains. Preventability of DRPs was assessed independently by a clinical pharmacist and pediatrician, following the Schumock and Thornton criteria, 45 and categorized as “definitely preventable,” “probably preventable,” or “not preventable.” Each criterion was assessed using a binary (yes/no) response. A DRP was classified as definitely preventable if at least one Part I criterion was “yes”; if all Part I responses were “no” but at least one Part II criterion was “yes,” it was classified as probably preventable. DRPs with no positive responses in either Part I or Part II were classified as not preventable.
Flow of the pharmacist-led intervention process
The pharmacist-led intervention process followed a standardized, stepwise workflow across all participating PICUs. Upon PICU admission, eligible patients were prospectively enrolled and underwent daily medication review by the assigned bachelor-level clinical pharmacist. This review involved a systematic assessment of medication orders, medical charts, laboratory results, nursing notes, and bedside clinical status, with additional caregiver interviews (Supplemental File S1) when required. Identified DRPs were documented and classified using the PCNE V8.01 framework.
For each identified DRP, the pharmacist formulated evidence-based recommendations, including dose optimization, drug modification, initiation or discontinuation of therapy, or monitoring strategies, guided by national and international pediatric references. Urgent or high-risk DRPs (e.g., dosing errors in critical medications, serious DDIs, or suspected ADR) were immediately communicated verbally to the responsible PICU physician, while non-urgent DRPs were discussed during routine clinical rounds or documented in the patient chart.
All proposed interventions were reviewed collaboratively with PICU physicians, and acceptance or rejection was recorded according to PCNE acceptance categories. Implemented interventions were followed longitudinally until DRP resolution, patient discharge, transfer, or death. Outcomes of interventions, including resolution status and preventability, were subsequently evaluated and documented. Centralized supervision by senior pharmacists and the use of standardized operating procedures ensured consistency of the intervention process across all study sites (Supplemental File S2). A schematic flow diagram illustrating patient enrollment, DRP identification, pharmacist intervention, clinician response, and outcome assessment is presented in Figure 2.

Flow diagram of the standardized pharmacist-led intervention process in the PICUs.
Statistical analysis
Data were entered into EpiData version 7.1 (developed and maintained by the EpiData Association, Odense, Denmark) and analyzed using STATA version 17 (developed and distributed by StataCorp LLC, College Station, Texas, USA). Descriptive statistics were used to summarize the characteristics of study participants. The Pearson χ2 test evaluated the association between categorical variables. Multicollinearity was assessed using the variance inflation factor, and model goodness of fit was evaluated using the Hosmer–Lemeshow test. Predictor of DRPs was examined using a binary logistic regression, with variables showing p < 0.20 in the bivariate analysis entered into the multivariable model. Statistical significance was set at p < 0.05.
Results
Study population and patient flow
During the study period, 422 children were initially considered for inclusion. After applying exclusion criteria, 28 patients were excluded: 12 declined participation, 8 were hospitalized for less than 24 h, 3 were lost to follow-up, and 5 were readmissions, resulting in a final cohort of 394 children admitted to the PICU. Of the included patients, 167 (42.4%) were admitted via the emergency department, 180 (45.7%) were transferred from medical wards, and 47 (11.9%) were postoperative admissions. At PICU discharge, 286 patients (72.6%) survived while 108 (27.4%) died. Among survivors, 210 (53.3%) were transferred back to the general medical ward, and 76 (19.3%) were discharged directly to home.
Socio-demographic characteristics of the study participants
In this study, 394 patients were included, of whom 220 (55.8%) were male. Infants (29 days–1 year) constituted 28.4% of the cohort, the overall median age was 3.0 years (IQR: 0.97–8). More than half of the participants (53.6%) resided in rural areas. The median body weight was 12 kg (IQR: 7–19). The majority, 330 patients (83.8%), had no previous history of ADR (Table 1).
Socio-demographic characteristics among patients admitted to the PICU of Northwest Ethiopia, 2025 (N = 394).

ADR, adverse drug reaction; DRP, drug-related problem; PICU, pediatric intensive care unit.
Clinical and treatment-related characteristics of the study participants
Overall, 242 patients (61.4%) presented with at least one comorbidity, with a total of 313 conditions identified based on the WHO-ICD, 11 system. The most frequently observed comorbidities were severe acute malnutrition (ICD: 5B50), affecting 24.0% of patients, and anemia (ICD: 3A00), reported in 18.4% (Figure S1). The median PICU length of stay was 6 days (IQR: 3–9; Table 2). Diseases of the respiratory system (ICD: CA00–CJ9Z) were the leading cause of PICU admission (28.4%), followed by infection and parasitic diseases (ICD: 1A00–1F9Z; 24.2%), and disease of the nervous system (ICD: 8A00–8E7Z; 19.8%; Figure 3). The most frequently prescribed medication classes were systemic anti-infective medications (93%), analgesic-antipyretics (78.3%), and gastrointestinal medications (35.2%; Figure 4). The medications most commonly implicated in DRPs were gentamicin (10.4%), meropenem (8.8%), and vancomycin (8.0%; Table S1).
Clinical and treatment characteristics of the study participants admitted to the PICU of Northwest Ethiopia, 2025 (N = 394).

DRP, drug-related problem; PICU, pediatric intensive care unit.

Reason for admission based on ICD-11 among the study participants admitted to the PICU of Northwest Ethiopia, 2025 (N = 394).
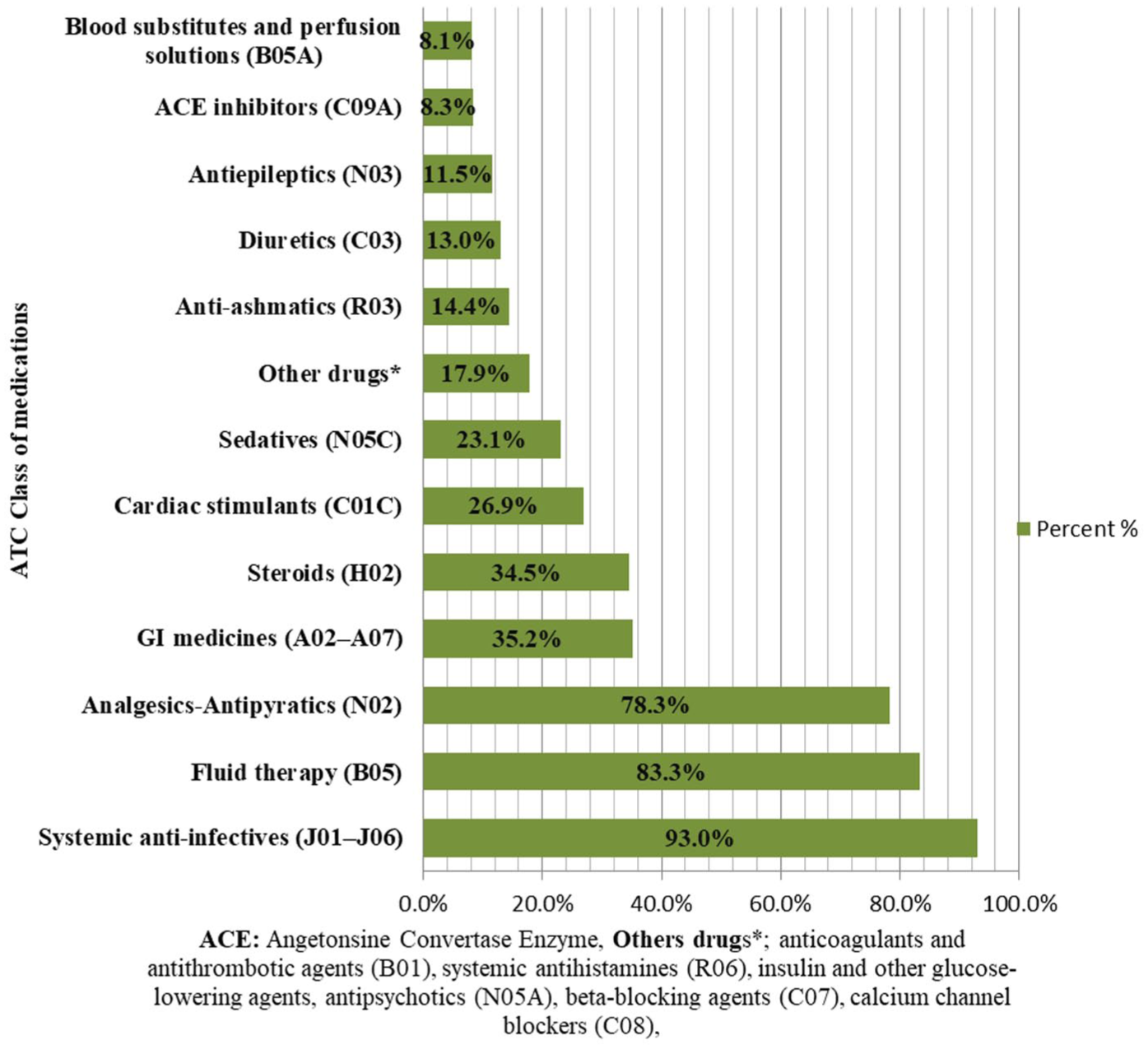
Drug therapeutic classification of study participants admitted to the PICU of Northwest Ethiopia, 2025 (N = 394).
Polypharmacy was significantly associated with the occurrence of DRPs (χ2 = 6.266, p = 0.012), with a significant linear trend observed as the number of medications increased (χ2 = 6.250, p = 0.012). Similarly, the number of disease conditions demonstrated a significant positive trend with DRP occurrence (χ2 = 5.387, p = 0.020; Table 3).
Association of comorbidity burden and medication count with DRPs.

Indicates spastically significance.
DRP, drug-related problem.
Clinical pharmacy classification of identified DRPs according to the PCNE V8.01
A total of 4582 medication orders were reviewed by the clinical pharmacists. Among the evaluated patients, 251 (63.7%) experienced at least one DRP, resulting in 522 identified DRPs. The mean number of DRPs per patient was 1.3 ± 0.8. Just over half of the affected patients (50.2%) experienced two DRPs. Problems related to treatment effectiveness accounted for the largest proportion of DRPs (54.6%), primarily due to suboptimal drug effect (34.8%) and untreated indications (16.5%). Treatment safety-related DRPs comprised 30.3%, while unnecessary drug therapy contributed 12.4% of all identified DRPs. A total of 665 underlying causes of DRPs were identified. The most frequent cause domains were drug selection (46.0%) and dose selection (43.8%). Low-drug dosing was the single most common cause, contributing to 24.7% of all identified causes, followed by inappropriate drug or drug combination selection (16.3%; Table 4). Clinically relevant DDIs were limited to category C and D classifications, with no category X interactions detected (Table S3).
DRPs, causes, and interventions by clinical pharmacists according to the PCNE V8.01 classification.
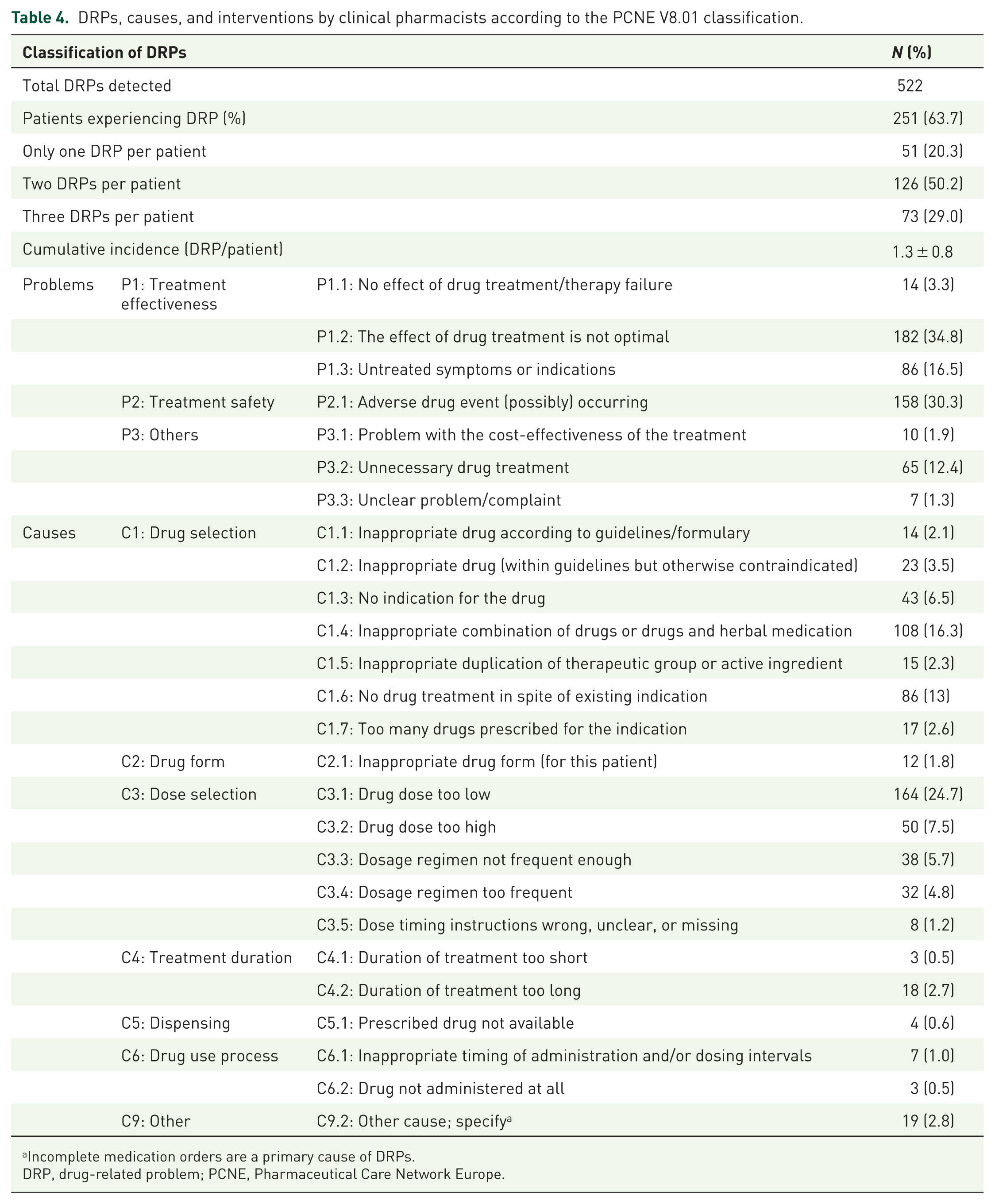
Incomplete medication orders are a primary cause of DRPs.
DRP, drug-related problem; PCNE, Pharmaceutical Care Network Europe.
A total of 665 identified causes. It is important to note that a single problem may have multiple underlying causes
Interventions, acceptance, and status of the performed interventions
A total of 687 pharmacist-led interventions were proposed to manage 522 DRPs. Most interventions were conducted at the drug level (83.4%), primarily involving dosage modification (38.4%), initiation of new therapy (12.5%), and changes in instruction for use (10.5%). The acceptance rate of pharmacist recommendations was 83.4% (n = 573). Among accepted interventions, 493 (86.0%) were fully implemented. Overall, 450 DRPs (86.2%) were completely resolved. Unresolved DRPs (11.7%) were mainly due to prescriber disagreement (6.3%) or lack of feasible therapeutic alternatives (4.6%; Table 5). Some reported pharmacist interventions are described in Table S4.
Interventions made by pharmacists, along with their acceptance and their status of intervention proposals, were classified based on PCNE V8.01.

The term “intervention” describes the actions taken by a clinical pharmacist to address DRPs. A single problem may require multiple interventions.
As many prescriptions were incomplete, the drugs’ doses were calculated by clinical pharmacists.
DRP, drug-related problem; PCNE, Pharmaceutical Care Network Europe.
Preventability of the DRPs
Overall, 97.7% of the identified DRPs were preventable, with only 2.3% were classified as unavoidable. Among the preventable DRPs, 78.6% were linked to dosage, frequency, and drug selection issues, followed by inappropriate medication choice (12.5%) and insufficient preventive measures (8.3%; Figure S2).
Factors associated with the occurrence of DRPs in the PICU
Variables with a p value <0.20 in the bivariable analysis were entered into the multivariable logistic regression model. Multivariable analysis identified several independent predictors of DRPs among pediatric patients admitted to the PICU.
Children aged 29 days to 1 year were approximately 2.2 times more likely to experience DRPs [adjusted odd ratio (AOR) = 2.2, 95% CI: 1.0–4.8] compared with older children. The presence of multiple prescribers increased the likelihood of DRPs by 1.8-fold (AOR = 1.8, 95% CI: 1.1–2.9). Patients exposed to polypharmacy (⩾5 medications) had a 1.7 times higher risk of DRPs (AOR = 1.7, 95% CI: 1.0–2.8) compared with those receiving fewer medications. A prolonged PICU stay (>10 days) was associated with a 2.4-fold (AOR = 2.4, 95% CI: 1.2–4.7) increased risk of DRPs.
In addition, patients with circulatory system disease had 3.5-fold higher likelihood of experiencing DRPs (AOR = 3.5, 95% CI: 1.4–9.0]. The use of anti-infective medications was associated with a fivefold increase (AOR = 5.0, 95% CI: 2.0–13.7), while the use of antiepileptic medications was associated with a 2.1-fold higher risk of DRPs (AOR = 2.1, 95% CI: 1.0–4.3; Table 6).
Multivariate logistic regression analysis of the predictors of DRPs in the PICU of Northwest Ethiopia, 2025.
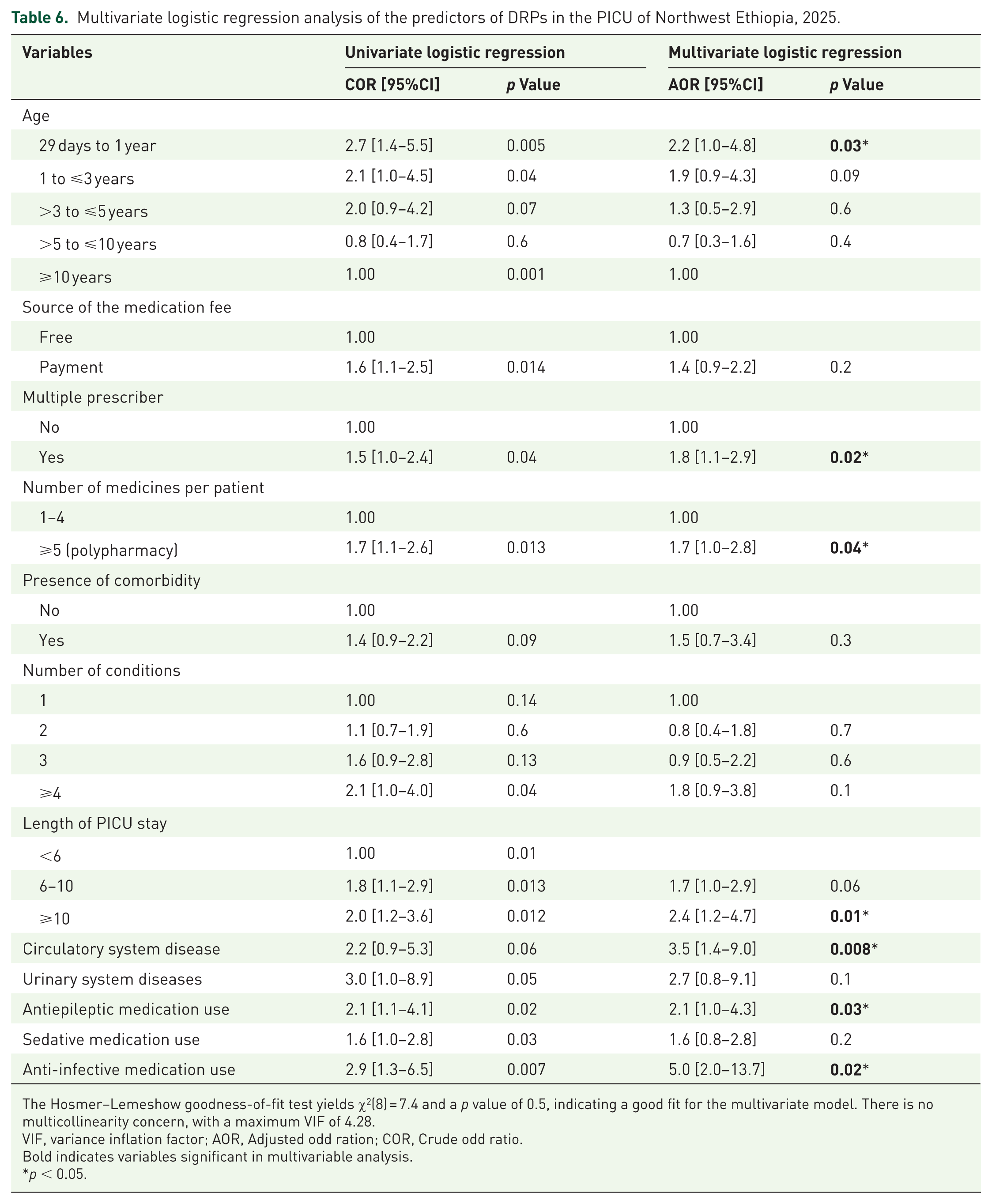
The Hosmer–Lemeshow goodness-of-fit test yields χ2(8) = 7.4 and a p value of 0.5, indicating a good fit for the multivariate model. There is no multicollinearity concern, with a maximum VIF of 4.28.
VIF, variance inflation factor; AOR, Adjusted odd ration; COR, Crude odd ratio.
Bold indicates variables significant in multivariable analysis.
p < 0.05.
Discussion
This prospective observational study, conducted in the PICU in Northwest Ethiopia, evaluated the impact of clinical pharmacist intervention on the identification and resolution of DRPs. We found that nearly two-thirds of admitted patients experienced at least one DRP. Unlike many previous studies, our investigation captured multiple dimensions of DRPs, including problems related to treatment effectiveness, safety, and prescribing quality. This comprehensive assessment provides a more holistic understanding of medication-related challenges in the PICU and is crucial for designing targeted, evidence-based pharmacist-led intervention strategies aimed at reducing DRPs among hospitalized pediatric patients.
The study found that two-thirds (63.7%) of PICU patients experienced at least one DRP, and the mean number of DRP per patient was 1.3 ± 0.8, which was comparable to findings from Turkey (1.36), 37 but lower than reports from Iran (1.7) 34 and Saudi Arabia (1.9). 46 These higher estimates in those settings may partly reflect smaller sample sizes (72 and 75 PICU patients, respectively), differences in patient acuity, and variation in clinical documentation quality. Even with daily reviews and multidisciplinary validation, underdetection of DRPs remains possible, as real-world clinical environments often involve incomplete records, dynamic patient trajectories, and subtle ADRs that may not be captured in routine documentation.14,47
The prevalence of DRPs of this study (63.7%) is consistent with findings from Southwestern Ethiopian (64.01%) 48 and Wolaita Sodo University Hospitals (60.2%), 19 both of which applied Cipolle’s method among medical pediatric patients. Comparable rates have also been reported in Vietnam (65.5%) among pediatric outpatients using PCNE V9.1, 15 in Brazil among NICU patient (60.5%), 13 and in a Turkish ICU patients (71.5%) using PCNE V8.02. 37 By contrast, our prevalence exceeds that observed in critically ill pediatric cohort in Saudi Arabia (25%), 46 and general pediatrics population in the United Kingdom and Saudi Arabia (45.2%), 49 Hong Kong (21%), 35 Malaysia (52.2%) 36 using PCNE V8.02, and King Abdulaziz Medical City, Jeddah (35.9%) using the PCNE V7.0. 50 These higher rates might be due to difference in patient acuity, as many of aforementioned studies focused on general pediatrics ward where medication intensity and physiological instability are lower than in PICU setting. 51 Conversely, PICU patients commonly present with multiple organ dysfunctions, require high-risk medication to sustain vital organ function, 52 and undergo frequent dose titration, all of which heighten their susceptibility to toxicity, dosing errors, and potential drug interactions. 53
Conversely, the DRP rates observed in our study were lower than those reported in studies from Iran PICU (80.4%) using PCNE V8.01, 34 China (89.9%) using PCNE V9.1, 54 and two Ethiopian hospitals, Dessie Referral Hospital (87.7%) and Jimma University Medical Center (74.3%), which applied Cipolle’s method.55,56 Such discrepancies may be explained by differences in the sample size, study design, extent of pharmacist involvement, medication utilization pattern, and institutional prescribing practice. Importantly, variation in the DRP classification system further contributes to heterogeneity. PCNE version differs in structural depth and coding granularity, with the newer version (e.g., V9.1) requiring more detailed and standardized documentation to classify problems, cause, and interventions. By contrast, Cipolle’s method is broader and may identify a wider spectrum of DRPs even when documentation is less detailed. Furthermore, variation in reference standards, for instance, the use of international guidelines, Micromedex, local formularies, or institutional protocols, can influence the detection of dosing, safety, and guideline deviations across studies. Furthermore, the reference sources utilized for dose, guideline, and safety assessment may also contribute to the inconsistency in DRP identification and reporting across studies. Notably, the prevalence in this study was lower than that observed in reported in an Egyptian NICU (89.8%) 11 using PCNE V9.01, reflecting the well-established difference between NICU and PICU populations. Neonates have high inter-individual variability, immature organ function, and frequent off-label medication use, all of which heighten the risk of dosing errors and drug interactions. 57
The primary causes of DRPs in the PICU of this study have shown that most of the DRPs were linked to inappropriate drug selection (46.0%) and dosing issues (43.8%). These findings were comparable with those of prior studies, with drug selection being the primary cause of DRPs.12,58,59 However, this pattern contrasts with other research; for example, in the UK-Saudi cohort, dosing problems accounted for 54% of DRPs. 49 Again, studies conducted in Hong Kong found that 22.2% drug selection and 44.2% dosing problems. 35 Another study conducted in a Turkish ICU reported 44% of dose selection and 36.8% of drug selection. 60 In another study conducted in the NICU, the most common causes of DRPs were dose selection (72.1%) and drug selection (14%). 34
The high rate of drug selection-related DRPs in our study was primarily due to a considerable percentage of patients (16.5%) who did not receive drug therapy despite the existing indication. This finding was in congruence with the Iranian study (13.1%). 34 While this figure is slightly lower than the findings from Mettu Karl Referral Hospital (25.09%) 48 and Dessie Referral Hospital (25.2%), 56 it was markedly higher than the rate observed in Hong Kong (3.7%). 35 This discrepancy may be attributed to differences in the healthcare professional’s knowledge and experience regarding appropriate drug indications and selection. Furthermore, contextual factors such as local diagnostic capacity, workload pressure, patient comorbidities, and specific clinical conditions could have contributed to these observed differences across institutions.
According to the PCNE V8.01 classification, the most frequent DRP identified in our study was a lack of treatment effectiveness, which accounted for 54.6% of all DRPs. This finding is consistent with previous research conducted on pediatric and critical care settings. For instance, a study conducted in Brazil among cardiac neonates reported a comparable rate of 49% for treatment effectiveness issues. 61 Similarly, investigations in the United Kingdom and Saudi Arabia found treatment effectiveness issues in 54% of all cases. 49 In the Brazilian NICU, this category was also predominant, with a recorded rate of 54.2%. 57 Moreover, a study conducted in an Iranian PICU demonstrated that treatment effectiveness problems affected in 51.3% of patients. 12
In particular, in the current investigation, this suboptimal treatment was primarily associated with low drug dosage, responsible for 24.7% of the DRP cases. This finding is similar to the Ethiopian study, which reported dosing problems at 42.5%, with low doses being the most frequent issue at 34.9%. 16 Comparable results were also reported in studies conducted in another region of Ethiopia, where low dosages accounted for 27.52% and 28.5% of DRPs.19,55 An Iranian study also reported a similar rate of 29.8%. 12 Nonetheless, this rate of low dosage was higher than those reported in Brazilian 61 and Hong Kong studies, 35 which found rates of 13.1% and 19.5%, respectively. This pattern suggests persistent challenges in accurate weight-based dosing, often influenced by inconsistent weight measurement, limited reference materials, and altered renal function among critically ill patients.62,63
High-dose prescribing was less common but still clinically significant, accounting for 7.5% of the cases in this study. This finding was relatively consistent with a study from another region of Ethiopia, which reported a rate of 3.9%. 19 However, our rate is lower than those reported in studies from Hong Kong (15.9%) and Saudi Arabia (16.1%).35,50 This discrepancy might reflect the differences in prescribing practices, patient populations, or clinical guidelines across different healthcare systems.
Drug safety problems the second most common DRPs, accounting for 30.3%. This proportion is comparable to findings from a Brazilian study (41.4%), 57 and an Iranian PICU (38.5%). 12 However, it contrasts with other reports from Iran and Ethiopia, where treatment safety was the most common DRP, occurring at 43.5%. In an Iranian study, this was followed by treatment efficacy, specifically when the therapeutic effect was not optimal, which was reported at 36.8%. 34 Furthermore, in an Ethiopian study, highlighting a drug safety due to high dose was the most prevalent problem recorded at 34.7%, followed by a dose too low at 19.8%. 64 These discrepancies underscore the influence of patient characteristics, prescriber experience, and medication-monitoring practices across settings.
The study also found that unnecessary drug therapy occurred in 12.4% of cases, which is consistent with findings from another Ethiopian pediatric ward study that reported rates of 11.7% and 16.8%, respectively.19,56 This highlights a significant problem of prescribing medications that offer no clinical benefit, potentially leading to ADR and increased healthcare costs. This highlights the need to strengthen deprescribing practice and antibiotic stewardship to reduce avoidable harms and resource wastage.
In this study, younger age, polypharmacy, and prolonged PICU stay were significant predictors of DRPs. Children younger than 1 year had twice the risk of DRPs compared with those older than 10 years, consistent with previous studies,15,50 although some studies have reported no significant age association 16 supporting contextual variability. Polypharmacy was independently associated with DRPs, in line with prior studies.19,49,55 Critically ill children often require multiple medications for organ support, infection management, sedation, and metabolic stabilization, with each additional drug increasing the risk of prescribing errors, guideline deviations, or DDIs. Prolonged PICU stay (>10 days) was another strong predictor, reflecting cumulative exposure to high-risk drugs, multiple regimen modifications, and evolving clinical complications. This trend has been consistently observed in Ethiopian and Brazilian studies.13,19,55 These findings emphasize risk-based medication review and proactive pharmacist integration in PICU teams, using risk markers to prioritize patients, optimize therapy, and reduce preventable DRPs.
According to this study, children with more than one prescriber also double the odds of DRPs. Teaching hospital environments, where interns, residents, and nurses are actively involved in prescribing, may increase this risk, particularly in the absence of robust medication reconciliation and structured clinical handovers. 65 Previous studies have repeatedly linked a multi-prescriber environment with polypharmacy, unnecessary drug therapy, and inconsistent dosing.66,67 In addition, children with circulatory system disease exhibited a higher DRP risk, consistent with reports indicating frequent extrapolation from adult dosing, narrow therapeutic indices, and altered drug clearance requiring frequent dose adjustments.13,68
The use of systemic anti-infective medications was the most frequently implicated drug class, consistent with global reports.35,49 Their extensive use in PICUs, driven by high infection burden, empiric prescribing, and limited microbiological diagnostics, 69 creates multiple opportunities for dosing errors and unclear indications. 56
Gentamicin was the single most common medication linked to DRPs involving treatment effectiveness, consistent with previous studies,35,57 likely due to high inter-patient variability in serum concentrations among critically ill children. 70 Meropenem was the second most frequently implicated medication, aligning with prior findings, 57 and reflecting its complex pharmacokinetics and the difficulty achieving therapeutic exposure in patients with fluctuating renal function. 71 These findings reinforce the importance of dose optimization and therapeutic drug monitoring where feasible.
The use of antiepileptic medications was also a major contributor to DRPs. Phenobarbital was frequently implicated due to high rates of DDIs and inappropriate selection.16,72 Given their narrow therapeutic window and susceptibility to pharmacokinetic interactions, antiepileptics require close pharmacist involvement in regimen review and monitoring.
In the present study, pharmacist intervention generated 687 recommendations, most commonly dosage modification. Findings were consistent with reports from pediatric and neonatal ICU care in Egypt 11 and Hong Kong, 35 underscoring reproducibility across diverse contexts. Acceptance (83.4%) and implementation (86.0%) rates indicate effective interdisciplinary collaboration, evident even in resource-limited settings where such teamwork is still developing. Higher rate reported in specialized children’s renal and neonatal cardiac settings.13,61,73 This difference possibly reflects more established multidisciplinary structures in specialized centers versus general hospital settings. Nonetheless, the resolution of 86.2% of identified DRPs further showed practical values of pharmacist involvement, consistent with the Egyptian NICU study. 11 Therefore, pharmacists support early detection and proactive management of DRPs through dose individualization, identification of DDIs, validation of therapeutic indications, and guidance on medication discontinuation. Routine inclusion of pharmacists in pediatric and neonatal ICU teams may offer opportunities to strengthen medication safety and optimize pharmacotherapy. 22
Limitations and strengths
The study has several strengths. Its multicenter prospective design improves generalizability and provides a robust representation of tertiary care public hospitals in Ethiopia. Daily active surveillance allowed timely identification and resolution of DRPs, and pharmacist–pediatrician consensus reduced classification bias. However, several limitations exist. First, the finding may not be generalizable to private healthcare institutions. Second, incidence rates for specific DRP categories were not calculated, limiting the ability to perform risk prioritization analyses. Third, the economic impact of pharmacist interventions was not assessed, despite being a key driver for policy adoption. Lastly, the study did not examine pharmacist roles in complex areas such as parenteral nutrition and electrolyte compounding, critical services in PICUs that require further investigation. Although PCNE V8.01 was used to align with local documentation practices, reliance on an older version may reduce comparability with studies using newer versions.
Conclusion
This multicenter prospective study found that DRPs were common among children admitted to PICUs, with treatment effectiveness issues, predominantly due to suboptimal dose selection, being the most frequent. Although the average number of DRPs per patient was modest, the observed pattern indicates opportunities to optimize medication use. Independent predictors were grouped into patient factors (younger age, circulatory system disease), treatment factors (polypharmacy, the use of systemic anti-infectives or anticonvulsant medications), and care factors (prolonged PICU stay, multiple prescribers). Pharmacist-led interventions were well received and largely implemented, underscoring their role and practical relevance in this setting. Overall, the findings indicate the potential benefit of integrating clinical pharmacists into multidisciplinary PICU teams to support medication optimization and patient safety. Further research should examine long-term outcomes, economic implications, and the potential value of expanded pharmacist roles, including antimicrobial stewardship and management of high-risk therapies.
Supplemental Material
sj-docx-1-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-1-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-2-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-2-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-3-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-3-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-4-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-4-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-5-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-5-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-6-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-6-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-docx-7-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-docx-7-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-tiff-8-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-tiff-8-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Supplemental Material
sj-tiff-9-taw-10.1177_20420986261422800 – Supplemental material for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia
Supplemental material, sj-tiff-9-taw-10.1177_20420986261422800 for The magnitude of drug-related problems, typology, and predictors among patients admitted to the pediatric intensive care unit: impact of pharmacist-led interventions in Northwest Ethiopia by Abel Temeche Kassaw, Getachew Yitayew Tarekegn, Tigabu Eskeziya Zerihun, Abaynesh Fentahun Bekalu, Samuel Agegnew Wondm, Tilaye Arega Moges, Woretaw Sisay Zewdu, Fasil Bayafers Tamene, Desalegn Addis Mussie and Samuel Berihun Dagnew in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
The authors would like to express their gratitude to Debre Tabor University and the data collectors for their invaluable contributions to this study. In addition, I want to express my appreciation for the Northwest Ethiopian Comprehensive Specialized Hospitals.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.