
Abstract
Background:
Medication errors (MEs) by caregivers at home are a cause of morbidity and mortality, shortly after discharge from the hospital.
Objectives:
The objective of this study was to determine the rate and types of MEs at the homes of children discharged from a hospital in Ghana and to explore the factors associated with these errors.
Design:
This was a cross-sectional study of infants and children discharged from the hospital to review medication administration practices.
Methods:
Caregivers of children discharged from the hospital after at least 24 hours of admission were interviewed at their homes about medication administration practices. The study assessed potential harm associated with MEs made by caregivers using the Harm Associated with Medication Error Classification tool. The Least Absolute Shrinkage and Selection Operator regression were used to identify the variables associated with MEs.
Results:
A total of 95 children (mean age: 28.6 months, 52.6% female) and their caregivers were included. Overall, 65 (68.4%) children experienced one or more MEs. Out of a total of 232 medications reviewed, 102 (44.0%) (95% CI: 37.6–50.4) were associated with a ME. The top two errors, wrong time errors and errors in the frequency of dosing were, 45.1% and 21.6%, respectively. Understanding the information on the disease condition being treated and the medicines dispensed was associated with committing fewer MEs. The number of medicines prescribed was associated with a higher likelihood of MEs. Out of 102 MEs, 48 (47.1%) were assessed as posing potentially no harm, 26 (25.5%) minor harm, 15 (14.7%) moderate harm, and 13 (12.8%) serious harm to the patients. Importantly, none of the MEs were assessed as posing potentially severe or life-threatening harm to the patients.
Conclusion:
MEs in children following discharge are high, and systems should be developed to prevent these errors.
Plain language summary
Why was this study done? Medication error in the home occurs when there is a mistake in how a person’s medicine is taken or given. Examples of medication errors in the home could involve taking the wrong medication, taking the wrong dose, taking the medicine at the wrong time, or giving the medicine more or less often. Sometimes, when caregivers take care of children at home after they leave the hospital, they make mistakes with how medicines are given to the children. These mistakes can make the children sick or cause some of them to die. This research wanted to find out how often these mistakes happen in the homes of children who are discharged from a hospital in Ghana, what kinds of mistakes are made, and why they happen.
What did the researchers do? We talked to caregivers of children within 7 days after they were discharged from the hospital. We asked them questions about how they give medicines to the children at home. We also used a special technique to find out which things might be responsible for the mistakes while they give the medicines to their children.
What did the researchers find? We visited the homes of 95 children (average age 28.6 months, 52.6% girls, the rest were boys). In general, 65 out of the 95 children (about 68%) had at least one mistake made by their caregivers while giving them their medicines. In the homes we visited, 232 medicines were given to the 95 children with 102 out of the 232 (about 44%) having a mistake. The two most common mistakes made by the caregivers were giving medicines at the wrong time (45.1%) and mistakes with how often the medicine is given (21.6%). Caregivers who understood more about the sickness of their children and the medicines made fewer mistakes. Also, in cases where the doctors prescribed more medicines to the children, the caregivers made more mistakes when giving the medicines to the children.
What do the findings mean? A lot of mistakes happen with medicines when children leave the hospital to their homes. Governments and regulatory authorities need to create better systems so that patients or their caregivers can report these errors. This will lead to actions being taken to prevent these errors from happening in order to keep children safe.
Background
Medication errors made by patients and caregivers in homes are potentially serious and similar to those made by healthcare professionals. A recent systematic review of 19 studies worldwide on pediatric medication errors by parents or caregivers at home found an error rate of between 30% and 80%. 1 Most literature available on medication errors from African countries focused on errors committed by healthcare providers in hospital settings. 2
Hospital discharges are high-risk periods for potential medication confusion and errors, especially the first few days following hospital discharge. 3 A study by Solanki et al. 4 among neonates up to 3 months of age discharged from a Neonatal Intensive Care Unit in India showed an error rate of 66.3% by parents with three types of medication errors, namely, errors in frequency of dosing, errors in dose administration, and discontinuation of medication. In Massachusetts, United States, Walsh et al. 5 reviewed 280 medications following 52 home visits in patients with sickle cell disease and seizure disorders and found that medication errors occurred in 22% of the medications reviewed, with 3% of errors resulting in actual patient harm and 11% being potentially harmful. Most of the errors were missed doses or failures to fill prescriptions. A study in the northeastern and southeastern United States found an error rate of 30% in 242 medication administration during 92 home visits. 6
Factors associated with medication errors by patients or their caregivers were polypharmacy or the number of medications,4,7,8 multiple health conditions, 4 cost-related barriers to medical services or medicines, 8 age of the caregiver,7,8 health literacy, 9 and language barriers. 10 Other contributory factors found to contribute to medication errors were problems with the use of support tools and measures to help in medication use 5 and measuring devices.11,12
Most of the studies on medication errors by caregivers have been done in high-income countries and there is a paucity of studies, especially from low- and middle-income countries (LMICs). Such studies are particularly important as it has been suggested that medication errors by patients or caregivers may be more frequent in LMICs because overcrowded outpatient clinics and low health literacy may be contributory factors to a higher rate of medication errors. 13 This is because overcrowded outpatient clinics may provide inadequate interaction between healthcare providers and caregivers. Furthermore, patients with low health literacy are more likely to find medication labeling confusing leading to misunderstanding of usage instructions. 14 Studies are therefore needed to inform on measures and interventions to reduce medication-related harm at home. The primary objective of this study was to determine the rate and types of medication errors by caregivers in homes of infants and children discharged from a hospital in Ghana. The secondary objectives were to explore the possible factors associated with medication errors, caregivers’ understanding of the information provided before discharge, and the potential harm associated with these errors.
Methods
Study design
This was a cross-sectional study of infants and children between the ages of 1–60 months discharged from the Child Health Department of the Greater Accra Regional Hospital, Ghana with at least one medication to be given at home. The reporting of this study conforms to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement. 15
Setting
The Greater Accra Regional Hospital was a 620-bed capacity hospital with a full complement of specialist services. The hospital provided a secondary-level healthcare service within the healthcare setting in Ghana. It was a major referral center in the Greater Accra region serving an estimated population of more than 5.4 million based on the 2021 Housing and Population Census. 16 The Department of Child Health was a 97-bed capacity facility that delivers healthcare to children from day 1 of life to 12 years of age. The average annual outpatient department attendance was 14,408 with 1500 annual admissions. The 6 units within the Department of Child Health were Emergency, Oncology, Pediatric Intensive Care, Neonatal Intensive Care, General Wards, and Specialist Clinics.
Participants
The study population consisted of infants and children between the ages of 1 and 60 months discharged from the Department of Child Health between May 2022 and October 2022. Infants and children were included when they were admitted for at least 24 h, lived within a 15-km radius from the hospital, and were prescribed at least one medication to be given at home. There were no specific exclusion criteria.
Variables and definitions
Patient and caregiver demographics: Data on patient characteristics during the cross-sectional study were obtained from the patient’s medical records, including the child’s gender, child’s age, diagnosis, and the number of drugs per prescription. Other variables, such as birth order, type of measuring device used, support tools as reminders, caregiver’s age, caregiver’s education, and caregiver’s health literacy, were collected during home visits.
Definitions: A medication error was defined as any deviation between the medication prescribed and that administered17,18 and the term ‘prescribed’ meant medicines which are used at home, either dispensed from the hospital pharmacy or a community pharmacy with a physician’s order. A caregiver is defined as any person who is responsible for administering the prescribed medicines to the child and may include a parent, grandparent, or a close relative.
The definitions of the various types of medication errors monitored during the home visits are in listed Table 1.
Definitions of medication errors monitored during the home visits (mutually exclusive categories).

Data sources
Data were extracted from the children’s medical records and during interviews with caregivers at their homes. The children were followed up to their homes by a study pharmacist within 7 days of discharge from the hospital. Elements of information on medicines to be given at home after discharge were obtained from the patient’s medical records. The parent or the caregiver who administered the medicine(s) to the child was interviewed about how the medicines were administered at home, the frequency of administration, possible missed doses, storage or management of the medicines, understanding of the information provided relating to the prescribed medicine(s) before discharge, and health literacy. The drug, doses, route of administration, and frequency of the medicines as reported by the caregiver were matched against those prescribed in the child’s hospital records to identify possible medication errors.
A three-member panel consisting of a consultant pediatrician, a pharmacist, and a nurse assessed the harm associated with medication errors using the Harm Associated with Medication Error Classification (HAMEC) tool, by considering factors such as the patient’s medical condition, other medications, clinical particulars, and side effect profiles of the medicines. The panel was chaired by the consultant pediatrician.
The data collection tool was designed based on earlier studies on medication errors by caregivers of infants and children4,23 and the short form of the health literacy measurement tool developed by the Agency for Healthcare Research and Quality, the Rapid Estimate of Adult Literacy in Medicine. 24 The data collection tool was pre-tested with 10 pilot home visits to assess misunderstandings, ambiguities, and difficulties participants may have understanding the questions. The data collection tool is provided as Supplemental Material.
We also adopted the HAMEC tool developed by Gates et al. 25 to explore potential harm associated with medication errors. The HAMEC tool categorized errors into potential severity of harm, ranging from ‘no harm’ to ‘severe harm’.
Study size
The sample size (i.e. total number of medicine administrations to be observed during the home visits) was determined to be 385 using Cochran’s formula

where Z is the standard normal variate which is 1.96 at a 5% level of significance (α = 0.05), P is the rate of medication errors by patients or caregivers in African homes which was estimated to be 50%, and e is the margin of error which is 5%.
Since the total population size of the patients was 583 based on the admission data of infants and children between 1 and 60 months to be admitted within 6 months at the Greater Accra Regional Hospital for 2022, the estimated sample size was reduced using finite population correction factor as follows
By substituting n = 385, N = 583, our final sample size for the study was 233.
We therefore estimated to visit 63 homes assuming each patient takes an average of 3.7 medications at home based on a study by Mirza et al. 27 in India to determine prescribing patterns in a pediatric outpatient department.
Statistical methods
Descriptive statistics in the form of frequencies and percentages were used to describe the background characteristics of study participants and caregivers. The dosage form and type of medication error were reported using frequencies and corresponding percentages.
We calculated the percentage of children with at least one medication error by dividing the number of medication errors by the number of home visits multiplied by 100 and the rate of medication error was calculated as the number of administrations with one or more errors divided by the total number of medications reviewed and multiplied by 100. 28 We also determined the 95% confidence intervals (CIs).
As a result of the high dimensionality of the data (larger number of independent variables relative to the sample size), that is 9 and 95, respectively, and with lower medication error rate, the multivariable Double Selection Poisson Regression model with independent variable selection and standard error adjustment using the Least Absolute Shrinkage and Selection Operator (LASSO)29,30 was used to identify independent variables associated with medication errors. The nine independent variables selected were known to influence medication errors from the literature. These were the child’s gender, child’s age, birth order, number of drugs per prescription, and measuring device. Others were support tools as a reminder, caregiver’s age, caregiver’s education, and caregiver’s health literacy. We initially fit a LASSO-based Poisson model with all the nine independent variables included and Bayesian information criteria (BIC) as the selection criteria based on the likelihood function of the model. It introduces a penalty turn for the number of parameters in the model. In using the BIC to compare models, the smaller value among the different estimated BIC values is chosen as the best model. In other words, lower BIC values indicate lower penalty terms and a better model.
All statistical analyses were conducted using Stata MP version 17 (StataCorp, College Station, TX, USA) and a p-value of less than 0.05 was considered statistically significant.
Understanding of the information by caregivers before discharge from the hospital was assessed with a list of nine questions with answers ‘yes’, ‘partial’, and ‘no’, developed, and reviewed by the authors. Understanding of the information was calculated as frequencies and percentages. A Fisher’s exact test was used to examine the association between the list of questions and medication errors by caregivers.
Harm associated with medication errors was identified by categorizing all errors into potential harm by adopting the five scales by Gates et al. 25 , namely, ‘no harm’, ‘minor’, ‘moderate’, ‘serious’, and ‘severe’. Each category of potential harm was calculated as frequency with the corresponding percentage.
Results
Of the 140 eligible caregivers of patients approached, 136 (97.1%) consented to participate in the study. Out of those who consented 95 (69.9%) were visited because the remaining 41 (30.1%) gave inaccurate phone numbers, the phones were off at the time of the scheduled home visit, or they provided the wrong address and/or direction to their homes.
In the 95 homes visited, the mother was responsible for administering medications in 92 (96.8%) of the cases with the father only 3 (3.2%). The mean age of the children was 28.6 months (SD 17.9). Table 2 provides the demographic details of the patients and their caregivers.
Demographic characteristics of patients and their caregivers.
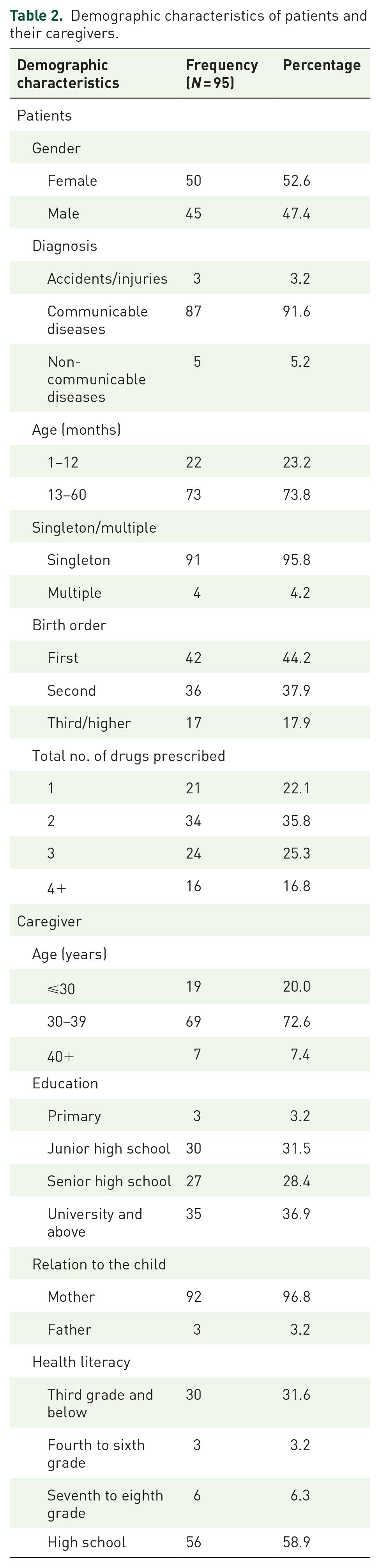
The average number of medicines prescribed for a child to be taken at home was 2.5 with communicable diseases as the highest reason for admission in 87 (91.6%) of the children followed up, 5 (5.3%) non-communicable diseases, and 3 (3.1%) accidents. The mean duration of hospital admission per child was 4.4 days (SD 1.4). We also found that 18 (18.9%) of the parents used a support tool or measures to help as reminders on when to give the medication(s) to their children. Support tools or measures used included mobile phone alarms, the time the child goes to bed at night, the time a program is aired on a local television, and sticker labels to indicate the time medicines are to be given.
The rate and types of medication errors
In the 95 homes visited, we found 65 of the children have been subjected to at least one of seven types of medication errors out of the nine monitored. The percentage of children who had been exposed to a medication error by caregivers was therefore 68.4% (95% CI: 59.1–77.8). A total of 232 medications were reviewed with 102 medication errors observed; thus, the rate of medication error in the home of the children was 44.0% (95% CI: 37.6–50.4).
The most commonly occurring type of medication error was wrong time error which occurred at a frequency of 46 (45.1%) out of the 102 errors committed with the least being error due to wrong medication occurring at a frequency of 1 (1.0%). During the home visits, nine different types of medication errors were assessed. Among these, seven types were observed, while the remaining two, wrong patient and error in route of administration were not encountered.
Table 3 shows the frequencies of the seven types of medication errors with examples.
Types of medication errors committed by caregivers following 95 home visits with examples.

We also found that a total of 45 different medicines were used with 29 (64.4%) of these having errors and the remaining 16 (35.6%) having no errors.
The generic names of medicines that contributed to the errors observed during the home visits with their associated frequencies and percentages are shown in Table 4.
Generic names of medicines that contributed to the errors observed during the home visits, along with their associated frequencies.

Of the 232 medications reviewed, 174 (75.0%) were syrups/suspensions, 26 (11.2%) tablets, and 16 (6.9%) suppositories. The remaining 12 (5.2%) and 4 (1.7%) were liquid oral drops and topical (or eye) ointments (or creams), respectively. This, therefore, represents 212 (91.4%), 16(6.9%), and 4(1.7%) of the medicines given by the oral, rectal, and topical routes, respectively. Table 5 shows the routes of administration with corresponding medication errors.
Route of administration and medication error.

The number of medicines per prescription and reminder tools emerged as the independent variables with the lowest BIC. A unit increase in the number of medicines prescribed was associated with an approximately 16% increase in the incidence rate ratio (IRR) of medication error [adjusted IRR = 1.16, 95% CI (1.01–1.13; p = 0.042)].
Understanding of information before discharge
We assessed caregivers’ understanding of the information provided about their children’s medication before discharge from hospital and found that 93 (97.9%) of them self-reported that they clearly understood the language in which information was provided to them before discharge, 81 (85.3%) were clear about the instructions on how to give their medicines but 6 (6.3%) were not and 8 (8.4%) indicated they were partially clear about information on how to give the medicines (Table 4).
We also assessed the association between the caregivers’ ‘understanding of information’ and the risk of medication errors. Our findings indicated that ‘clarity of information provided before discharge’ and ‘understanding the general information including how long to give the medication and the disease condition being treated’ were associated with fewer errors with corresponding p-values of 0.028 and 0.002, respectively. Table 6 provides the association between caregivers’ understanding and the risk of medication errors.
Caregiver’s understanding of information before discharge and the risk of medication errors.

Fisher’s exact test.
Potential harm associated with medication errors
We classified the potential harm associated with medication errors by caregivers using the HAMEC tool and found that out of the 102 medication errors, 48 (47.1%) were no harm, 26 (25.5%) were minor harm; 15 (14.7%) were moderate harm; and 13 (12.8%) were serious harm. None of the medication errors reviewed was classified by the three-member panel as posing severe harm to the patients. Examples of medication errors classified as having the potential for serious harm included all medication errors relating to the storage of antibacterial suspensions intended for refrigeration but stored at room temperature. The three-member panel unanimously agreed that these errors have the potential to lead to the deterioration of these medicines resulting in failure of therapy. For instance, during the home visits, the study pharmacist found that flucloxacillin and amoxicillin + clavulanic acid suspensions were discolored after 4 days of being kept at room temperature. Mothers were advised to buy new medications. An example of no harm medication error was when a mother forgot to give metronidazole suspension until an hour later than the scheduled time to a 24-month-old child who was diagnosed with acute gastroenteritis.
Discussion
The study showed that medication errors were common in children at home following discharge from the hospital, with more than half of the patients experiencing at least one of the seven types of medication errors. Caregivers who understood the information before discharge from the hospital were less likely to make medication errors. A higher number of medicines was associated with a higher rate of medication errors.
Mothers were responsible for the administration of medications in most homes which outlines the role of the mother or women in general as health managers or promoters within the family. Our finding is consistent with earlier studies in the United States 5 and India. 4 Communicable diseases (e.g. malaria, acute upper respiratory tract infections, gastroenteritis, and bronchopneumonia) were common reasons for admission which is not surprising as infectious and parasitic diseases represent the highest causes of admission in Africa. 31
The medication error rate in our study was twice the rate reported in similar studies in the United States.5,6 A systematic review of 33 studies mainly from high-income countries found an error rate of 1.9–33% 7 but our rate was within the range reported in another systematic review. 1 The higher error rate in our study could be due to the relatively small number of caregivers using support tools. The medication error rate was 19% in our study compared with 38% in the study by Walsh et al. 5 Support tools have been found to reduce the rate of medication errors. Differences in medication error rates could be due to methodological differences between studies, such as the definition of errors and the type of errors included. In our study, we included nine different types of medication errors. Also, reported error rates were likely to be underestimated, 32 and differences in data collection methods have an impact on the rate of medication errors.
Other studies found errors in frequency of dosing, discontinuation error, and dose deviation as the most common types of errors4,5 but wrong time errors and errors in management or storage have not been discussed in these studies. Errors in management or storage may lead to the deterioration of medicines because of the high temperature in Ghana. The homes where medicines were stored at room temperature did not have refrigerators. Although the reasons have not been investigated, they may vary from power outage, lack of electricity connection, and lack of financial resources to acquire a refrigerator. Our findings are very relevant, as these errors may cause therapeutic ineffectiveness resulting in the disease being untreated and antimicrobial resistance.
The majority of caregivers understood the information given, including information on the condition being treated and how long to give the medications. However, only one caregiver stated that information on the possible side effects of the medicine was provided and less than a quarter asked questions about their medicines. This suggests that the majority of caregivers were not eager to find out from their healthcare providers information on the safety of their medications. The reason may be because they were unaware that they had the right to ask questions or they were not encouraged to do so; a South African study found a similar situation. 33
Although our study showed that none of the medication errors by the caregivers posed serious or life-threatening harm, the study showed a high level of medication errors made by caregivers just as those made by healthcare providers among inpatients in African hospitals. 2 This therefore calls for the establishment of systems to prevent these errors. However, there are limited interventions to prevent errors in the home compared to hospital settings. An earlier study found limited systems in African countries for patients to report these errors for appropriate action. 34 To prevent medication errors, caregivers in our study have adopted tools and support systems that were found to reduce these errors as shown in an earlier study. 5
To reduce medication errors by patients and caregivers at home, the authors propose the following; first, advocate for the use of support tools, including mobile apps, and alarm reminders on cellphones to help remind patients and caregivers about when to take or give the medications. 5 This may help significantly reduce wrong time errors, which is the highest type of error detected in our study. Our study also found the use of other support tools or systems to reduce medication errors such as the time the child goes to bed at night, the time a program is aired on a local television, and sticker labels to indicate the time medicines are to be given which have not been previously reported.
Second, healthcare professionals need to be sensitized to the seriousness of the problem and the need to provide patients and or their caregivers with clear and unambiguous verbal and written instructions on how to take their medications at home before discharge from the hospital. 3 The use of pictographic diagrams to demonstrate the correct dosing before discharge from the hospital may also be helpful. 35
Third, patients and caregivers should be empowered to ask their healthcare provider or pharmacist any questions they may have about their medication, including dosing instructions, and possible side effects. 36
Finally, interventions to reduce medication errors which have the potential to lead to therapeutic ineffectiveness and deterioration of medicines that were inappropriately stored should include prescription of medicines that do not need refrigeration such as dispersible tablets instead of powder for suspensions which are reconstituted and stored in the refrigerator.
Strengths and limitations of the study
This study contributes to the scarce knowledge on medication errors by caregivers in the homes of infants and children discharged from a hospital in Africa. The limitations of the study are the modest sample size and the fact that the study was conducted in only one urban hospital in Ghana. This may make it difficult to generalize the findings beyond the study setting because caregivers included in the study and their chances to commit medication errors may be unique to this hospital. We also noticed that wrong time errors may be difficult to measure in the home setting. However, this was reduced by asking caregivers if they had ever forgotten to give any of the medicines to their wards and the time it took them to remember (in hours).
Conclusion
The study showed a high level of medication errors made by caregivers in the homes of children discharged from the hospital, which is a major concern. The findings should be used by healthcare professionals, patients, and the pharmaceutical industry to formulate strategies to improve medication safety in the home and treatment outcomes. It should be noted that the results presented in this study are self-reported, and no objective measures have been used to determine the frequency of errors.
Supplemental Material
sj-docx-1-taw-10.1177_20420986231225850 – Supplemental material for Medication errors by caregivers in the homes of children discharged from a pediatric department in Ghana
Supplemental material, sj-docx-1-taw-10.1177_20420986231225850 for Medication errors by caregivers in the homes of children discharged from a pediatric department in Ghana by George Tsey Sabblah, Florence van Hunsel, Katja Taxis, Mahama Duwiejua, Seth Kwaku Seaneke and Eugène van Puijenbroek in Therapeutic Advances in Drug Safety
Footnotes
Acknowledgements
Dr. Yvonne Nana Ama Brew helped organize and supervise data collection at the Greater Accra Regional Hospital. Mr. Anthony Godi assisted with data analysis using Stata MP version 17 (StataCorp, College Station, TX, USA).
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.