
Abstract
Aim:
Quarantine due to the COVID-19 pandemic altered the supply and demand of health services. This, together with the ‘infodemic’ and generalized panic, could alter the patterns of self-medication in the population. The objective was to characterize the patterns of self-medication in four cities of Colombia during mandatory preventive isolation in 2020.
Methods:
This was a cross-sectional study done in four Colombian cities during mandatory national preventive isolation between June and September 2020. A sample of 397 adults who responded to an online survey, based on the Instrument for Systematic Data Collection for Self-medication (Instrumento de Recolección Sistemática de Datos para la Automedicación–IRIS-AM), was obtained. The use of social networks (including WhatsApp) as the source of information about medications was explored.
Results:
The 397 people surveyed had a median age of 31.0 years, and 58.2% were women. The prevalence of self-medication during lockdown was 34.3% (n = 136). Medications targeting the nervous system (n = 117; 86.0% of those participants with self-medication) and the musculoskeletal system (n = 68; 50.0%) were the most commonly used. Ten (7.4%) of the self-medicated patients reported doing so to prevent COVID-19, and 15 (11.0%) named social networks as the source of information.
Conclusion:
More than one-third of the participants reported self-medication during COVID-19 lockdown, mainly with analgesic-type nervous system medications. People who reported self-medication to prevent COVID-19 often got their information from social networks, the Internet, and WhatsApp.
Plain Language Summary
Self-medication during mandatory COVID-19 isolation
Introduction
The COVID-19 pandemic has affected all aspects of society, in particular the health of people, both physical and mental. Fear, anxiety, depression, and stress are common psychological reactions to the current pandemic1,2 and are promoted and perpetuated by a wide spectrum of variables, such as disinformation, social distancing measures, the economic crisis, and exposure to media.3–5 The overwhelming amount of information and the lack of precise conclusions generate confusion and panic and lead to distorted interpretations of the facts, 5 promoting behaviors that negatively affect health, 6 including self-medication. 7
Self-medication is defined as the use of medications, herbs, or home remedies on one’s own initiative or on the recommendation of another person, usually a friend, family member, neighbor, or pharmacist, without prior consultation with a doctor. 8 This large-scale phenomenon constitutes a public health problem associated with adverse outcomes that ultimately create an economic burden on health services.9,10 Multiple similar scenarios of misinformation and rumors amplified by social networks and media have been presented, with alleged potential therapies not approved for the treatment of COVID-19, such as hydroxychloroquine/chloroquine, chlorine dioxide solution, azithromycin, antiretrovirals, such as ritonavir and lopinavir, and nonsteroidal anti-inflammatory drugs such as ibuprofen.7,10,11 In previous epidemics, self-medication has increased in the general population, 12 and the current ‘infodemic’ of false news and rumors may also contribute to its increase in the current pandemic.
In Colombia, the first case of COVID-19 was recorded on 6 March 2020. 13 From then until 14 December 2021, more than 5,095,000 people have been infected in Colombia, 14 and the infection rate triggered strict mandatory preventive isolation during the first 6 months of the pandemic.15,16 During this period, the free movement of citizens was severely restricted, and many commercial, academic, and school activities as well as some health services were forced to close or operate through virtual means, 17 which caused, as in other countries, a drastic fall in the supply of health care. This, together with the generalized panic at the beginning of the pandemic and the fear of sanctions for violation of quarantine, led to a decreased demand for health services and the seeking of alternatives for the treatment of pathologies.18,19
Self-medication can generate complications ranging from medication shortages to bacterial resistance or to adverse reactions that can even lead to death.20,21 The characteristics of self-medication in the COVID-19 pandemic in Colombia are not well known and are reported mainly by unofficial sources, so this study sought to determine the self-medication practices during times of mandatory isolation for COVID-19 in a group of people in Colombia.
Methods
Study design and population
A cross-sectional descriptive observational study was conducted to characterize self-medication patterns in a population of the city of Pereira (Risaralda) and its surrounding area (including the neighboring cities: Dosquebradas, Santa Rosa de Cabal, and La Virginia).
Data were collected online through self-completed surveys built on the Google Forms platform, based on the Instrument for Systematic Data Collection for Self-medication (Instrumento para la Recolección de Información Sistemática en Automedicación–IRIS-AM)© prior authorization by the authors, 9 modified according to the variables of interest for this study. Nonprobabilistic convenience sampling was performed. The online data collection instrument was sent and publicly disseminated by social networks (Facebook, WhatsApp) and the advertising bulletins of two universities in the region and was available to the general population from June 30 to September 14, 2020. Age 18 years or older and agreement to participate in the study were the inclusion criteria. People who claimed to be health professionals were excluded.
The following groups of variables were included: (1) sociodemographic: age, sex, type of affiliation to the health system (subsidized, contributory, and other), educational level (highest completed: none, basic (primary and high school), technical, advanced (professional and postgraduate)), socioeconomic stratum (six strata grouped into low (1–2), medium (3–4), and high (5–6)), as well as area of residence, and so on; (2) prevalence of self-medication: use of medications without medical prescription: sometime in life and during isolation due to COVID-19; (3) nature of self-medication: name of medications used; type of medication used according to the ATC classification – Anatomical Therapeutic Chemical Classification System); (4) signs or symptoms that motivated self-medication, including prevention of COVID-19; (5) reasons for nonuse of health services; (6) source of information driving their decision and the source of the medication; and (7) comorbidities and comedications of the patient, for example, high blood pressure, ischemic heart disease, diabetes mellitus, dyslipidemia, cancer, hypothyroidism, asthma, chronic obstructive pulmonary disease, autoimmune diseases, HIV infection, smoking, and obesity.
Analysis
The data collected were exported to Microsoft Excel 2013 and analyzed with the statistical package SPSS Statistics version 26.0 for Windows (IBM, USA). Descriptive statistics are used to present the results. The χ 2 test was used to detect relationships between the consumption of medications to prevent COVID-19 and the other categorical variables. The level of statistical significance was set at p < 0.05.
The protocol was approved by the Bioethics Committee of the Universidad Tecnológica de Pereira in the category of ‘research without risk’, according to resolution No. 8430 of 1993 of the Ministry of Health of Colombia. The ethical principles and confidentiality of information established by the Declaration of Helsinki were respected. The participants granted their consent at the time they completed the electronic questionnaire.
Results
A total of 427 people initially answered the virtual questionnaire, and 397 questionnaires met the selection criteria and were analyzed. Of these, the median age of respondents was 31.0 years (interquartile range: 24.0–41.0 years), and the majority were women (n = 231; 58.2%) and resided in the city of Pereira (n = 256; 64.5%). The main socioeconomic level was medium (n = 235; 59.2%), most of them belonged to the contributory regime of the health system (n = 288; 72.5%), and most had a high educational level (advanced n = 268; 67.5%; Table 1).
General characteristics of the sample, discriminated by groups according to the history of self-medication since the beginning of isolation.
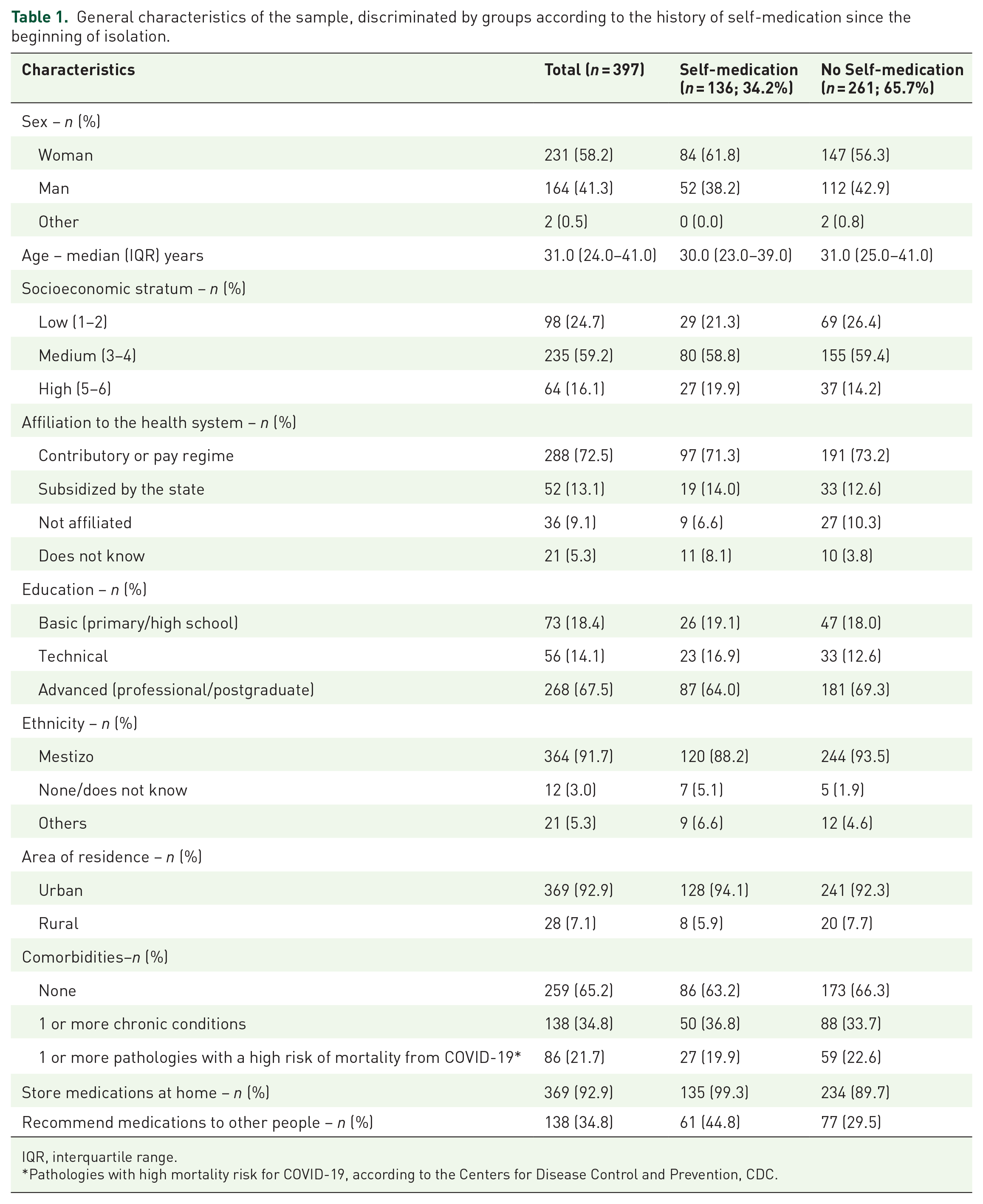
IQR, interquartile range.
Pathologies with high mortality risk for COVID-19, according to the Centers for Disease Control and Prevention, CDC.
Of all the participants, 136 reported having self-medicated from the beginning of preventive isolation until the time of the survey, indicating a prevalence of self-medication in this period of 34.3% (95% confidence interval (CI): 29.6–39.2%) (Table 1). Most reported having self-medicated at some point in life (n = 342; 86.1% 95% CI: 82.4–89.4%). Likewise, 92.9% (n = 369) kept medications at home, and 34.8% (n = 138) recommended medications to other people. Storing medications at home (odds ratio (OR): 15.58; 95% CI: 2.09–115.92; p < 0.001) and having recommended medications to other people (OR: 1.94; 95% CI: 1.26–2.99; p = 0.002) were associated with self-medication during quarantine.
Table 2 shows the number of people who self-medicated with at least one drug from each pharmacological group. On average, 3.3 ± 1.9 self-medicating drugs were reported per person who self-medicated. Among the most commonly used pharmacological groups were nervous system medications (n = 117; 86.0% of those participants with self-medication reported during quarantine), mainly in the form of analgesics (i.e: of acetaminophen). Drugs for the musculoskeletal system (n = 68; 50.0%) and for the respiratory system (n = 56; 41.2%) were next in frequency.
Number of self-medicated people for each pharmacological group (n = 136).

SD, standard deviation.
Excluding sex hormones and insulins (corticosteroids for systemic use).
Among the other variables collected in relation to self-medication during lockdown, the most frequent reasons for self-medication were pain (n = 113; 83.1%), respiratory symptoms (n = 62; 45.6%), and systemic symptoms (n = 45; 33.1%; Table 3). The main reasons for not consulting a doctor (and choosing to self-medicate) were knowledge about the treatment for their discomfort (n = 113; 83.1%) and fear of contracting COVID-19 (n = 39; 28.7%).
Characterization of self-medication during mandatory preventive isolation (n = 136).

Approximately half of the participants indicated that the source of information for their selection of self-medicating drugs was medical formulas from previous consultations (n = 59; 43.4%). Other sources also stood out, such as the reference of a relative, friend, neighbor, or acquaintance and popular customs, each reported by 48 participants (35.3%). A total of 15 people (11.0%) also reported having received information on social networks, the Internet, and WhatsApp (Table 3).
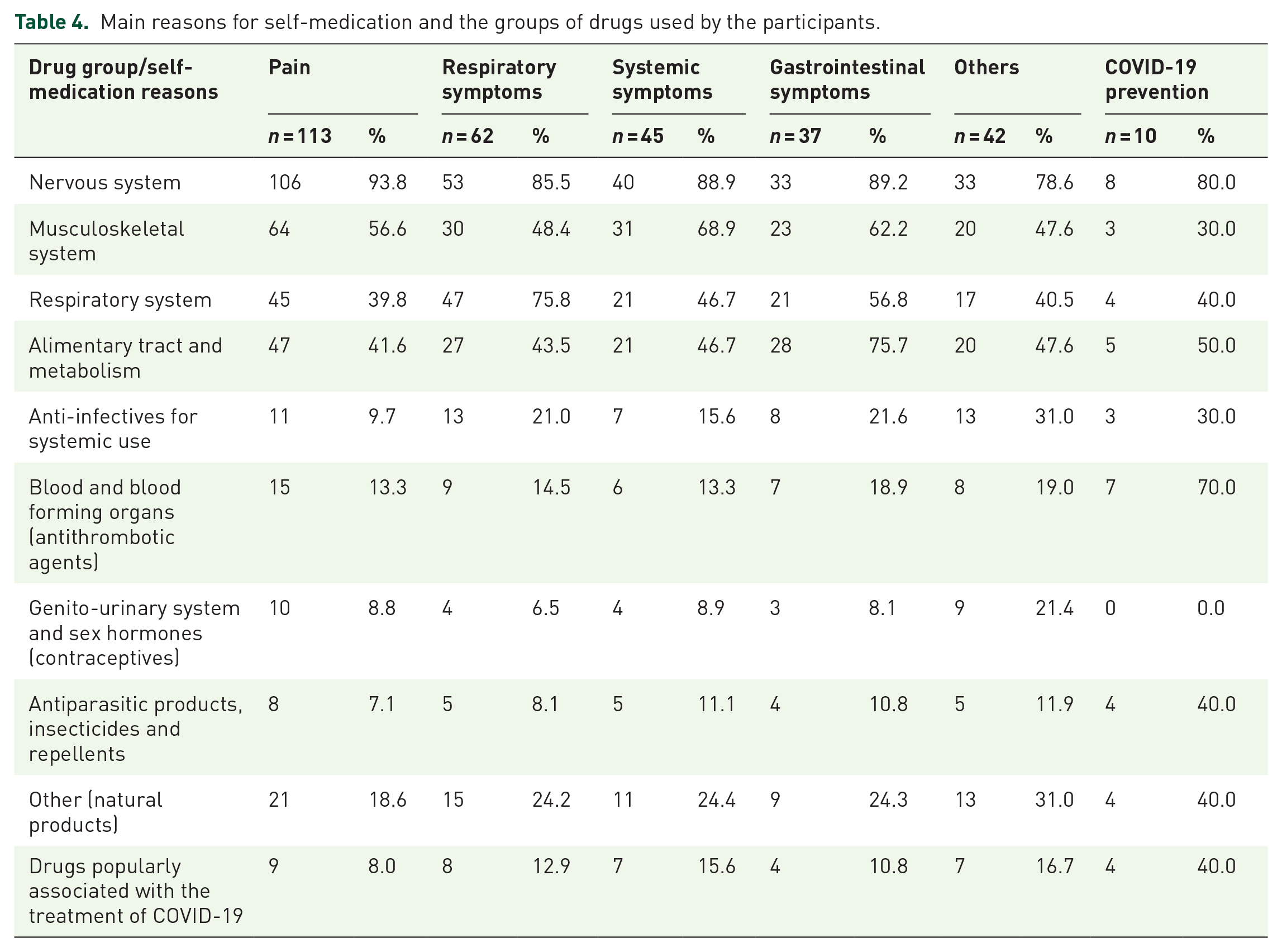
Table 4 shows the main reasons for self-medicating according to the subgroup of medication, taking into account that the same patient could report more than one group of medications and more than one reason for self-medication. From the questions about the behaviors taken against different hypothetical symptoms, it was found that the participants preferred to self-medicate for headache, menstrual cramps, flu symptoms, abdominal pain, indigestion symptoms, or muscle pain, while they would prefer to consult a doctor about dyspnea, other symptoms they associated with infections, or dysuria (Figure 1).
Main reasons for self-medication and the groups of drugs used by the participants.
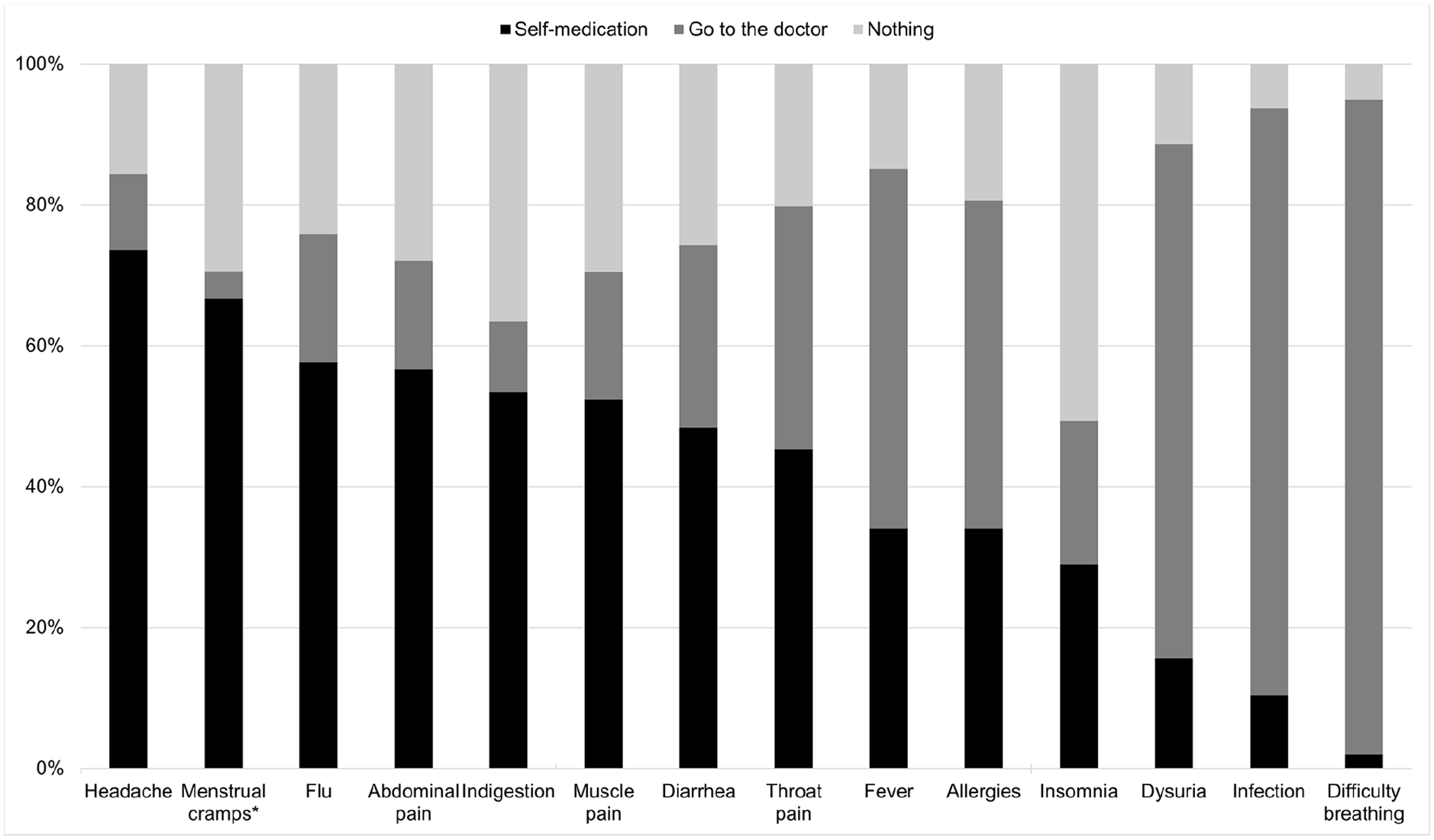
Behaviors taken against different hypothetical symptoms by the study participants (n = 397).
Ten patients (7.4%) specifically reported taking medications to prevent COVID-19, and five of them reported that the source of information was social networks (OR: 11.6; 95% CI: 2.87–46.94; p = 0.002). The other sources of information were not correlated with the consumption of drugs for this type of prevention. All patients who took chloroquine, hydroxychloroquine, and ivermectin cited prophylaxis against COVID-19, as did one of the patients who took azithromycin (1/7 = 14.3%). The other patients who took azithromycin indicated its use for fever, flu, and other types of infections. Finally, the taking of drugs for the prevention of COVID-19 was also related to distrust in health personnel or institutions (OR: 10.4; 95% CI: 2.05–52.49; p = 0.013) and fear of being sanctioned or fined for leaving the house (OR: 7.29; 95% CI: 1.54–34.41; p = 0.026).
Discussion
This study determined the prevalence of self-medication in general and during lockdown in response to the COVID-19 pandemic in a group of people from Colombia. Approximately 7% of respondents resorted to self-medication to protect against COVID-19, and this practice was related to the use of social networks, the Internet, and WhatsApp as a source of information. These data may be of interest to government entities and health service providers to promote better education of the population on issues of medications and self-medication during the current pandemic or similar situations.
When comparing the prevalence of self-medication with previous data from Colombia, similar values were found for both general self-medication (at any time in life) and recent self-medication. A 2013 study in Colombia described a prevalence of self-medication in the last 30 days of 32%, 9 similar to the 34% of this study during lockdown. This indicates that there do not seem to be significant variations in prevalence in terms of recent self-medication despite the current pandemic. This contrasts with findings reported in Kenya, where self-medication went from 36% before the pandemic to 60% during the pandemic, 22 although the population analyzed was health workers, a profession excluded from this analysis. In the previous Colombian study, people who kept medications at home and who recommended the use of medications to others were more likely to self-medicate, 9 which was also reflected in this population analyzed during the pandemic. Other factors reported in association with self-medication (in a study focused on antimicrobials) include, for example, level of education or age. 23
In a study conducted in Peru, it was found that 33.4% of the population surveyed had self-medicated during isolation due to the COVID-19 pandemic, 7 a value very similar to that of this study. However, this report specifically asked about self-medication with drugs probably used for the management or prevention of COVID-19, including azithromycin and hydroxychloroquine. 7 These medications, along with chloroquine and ivermectin, have been popularly proposed for the management and prevention of COVID-19, but they raise the risks of important adverse events, such as the prolongation of the QT interval. 24 In this study, respondents also reported the unprescribed consumption of these molecules.
Other studies have measured the prevalence of self-medication in the context of the pandemic, both at the level of medications in general and those specifically focused on preventing COVID-19. For example, in Togo during the first part of the pandemic, self-medication had a prevalence of 34.2%, 25 while in Nigeria it reached 41.0%, 26 in both countries coming mainly from the consumption of vitamin C. In this study, high values of vitamin consumption were also found, although the main drugs used in self-medication corresponded to analgesics, as has been seen in other publications.7,9
A high percentage of the respondents indicated the presence of respiratory symptoms as a reason for self-medication, mainly to help fight flu-like symptoms. Similarly high proportions of patients reported self-medication as an initial management alternative for diarrhea, sore throat, and fever. This is worrisome in the context of the pandemic because since it started, there has been a call to notify the health system of these symptoms to schedule medical consultations and to define the need for sampling for COVID-19, isolation, or hospitalization.27,28 On the contrary, the majority of the participants indicated that, in case of breathing difficulty, they would seek medical consultation as a first option.
Self-medication with anti-infective agents is a special point of attention. In this study, approximately 15% of participants who self-medicated used an antibiotic or an antifungal without a medical prescription. In a study that evaluated the practices of antibiotic consumption in a sample of patients from a health institution in Uganda, more than 20% had used antibiotics at some time without a medical prescription. 29 This was associated with some variables of interest, such as religion, which was not assessed in this study. A meta-analysis published in 2015 found an overall prevalence of antimicrobial self-medication of 39% in developing countries; however, the figures are highly variable, ranging from 4% to 91% according to the country. 23
Taking antibiotics without medical indication or evaluation represents serious problems for health care systems due to possible adverse reactions and the appearance of antibiotic resistance, 30 which may be even more serious in the context of the current COVID-19 pandemic. 31 Reports in France have described that adverse reactions to medications related to self-medication increased from 1.6% in 2019 to 3.7% during the pandemic, which highlights the importance of analyzing this type of situation in the current public health context. 32
Although few participants self-medicated to prevent COVID-19, they usually chose to do so based on information from social networks and WhatsApp. The COVID-19 infodemic is reflected not only in aspects of self-medication but also in other areas of vital importance to public health, such as the use of masks and the acceptance of vaccines, and an epidemiological model has even been proposed to try to mitigate its effects early through specially designed information surveillance systems. 33
The study has limitations inherent to its observational design. The sample size was small even though the questionnaire was disseminated through social networks and official channels of two higher-education institutions in the city. Likewise, the sample was a convenience sample, and the survey was self-administered precisely because of the COVID-19 lockdown situation. This could also have limited the access of some population groups to the survey and therefore the generalizability of the results. As a strength, this study used an instrument previously used in research on self-medication, and it included specific questions about COVID-19 and questions on the sourcing of information from social networks during the lockdown.
Conclusion
More than one-third of the participants reported self-medication during the preventive isolation time for COVID-19, mainly with analgesics. A fairly high proportion of people who reported self-medication to prevent COVID-19 cited social networks, the Internet, and WhatsApp as sources of information driving their choice. These data support the need to improve the education of the general community about the appropriate use of medications, improve access to reliable health information, and even convey the importance of seeking medical advice and reporting symptoms suggestive of COVID-19 instead of self-medication.
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.