
Abstract
Aims:
Individuals taking immunosuppressants are at increased susceptibility to viral infections in general. However, due to the novel nature of the COVID-19, there is a lack of evidence about the specific risks of the disease in this patient group. This systematic review aims to summarize the current international clinical guidelines to highlight areas where research is needed through critical appraisal of the evidence base of these guidelines.
Methods:
We conducted a systematic review of clinical practice guidelines about the usage of immunosuppressants during the COVID-19 pandemic. Electronic databases including MEDLINE and the websites of relevant professional bodies were searched for English language guidelines that were published or updated between March 2020 and May 2020 in this area. We assessed the quality and consistency of guidelines. The evidence base underpinning these guidelines was critically appraised using GRADE criteria.
Results:
Twenty-three guidelines were included. Most guidelines (n = 15, 65.2%) informed and updated evidence based on expert opinion. The methodological quality of the guidelines varied, ranging from ‘very low’ to ‘moderate’. Guidelines consistently recommended that high-risk patients, including those who are taking high doses of steroids for more than a month, or a combination of two or more immunosuppressants, should be shielding during the outbreak. Most guidelines stated that steroids usage should not be stopped abruptly and advised on individualized risk–benefit analysis considering the risk of the effect of COVID-19 infection and the relapse of the autoimmune condition in patients.
Discussion:
Clinical practice guidelines on taking immunosuppressants during the COVID-19 outbreak vary in quality. The level of evidence informing the available guidelines was generally low. Given the novel nature of COVID-19, the guidelines draw on existing knowledge and data, refer to the use of immunosuppressants and risks of serious infections of other aetiologies and have extrapolated these to form their evidence base.
Introduction
The novel coronavirus SARS-CoV-2 has spread rapidly across the globe since its discovery in Wuhan, China in December 2019, and was declared a pandemic by the World Health Organization (WHO) in March 2020. 1 COVID-19 is highly transmissible between humans and in moderate to severe cases causes bilateral interstitial pneumonia with associated respiratory failure. High levels of transmission with significant impact relating to COVID-19 have forced governments worldwide to introduce social distancing or lockdown measures. Among those considered most at risk, who are being asked to take even stricter shielding measures, are patients taking immunosuppressant medications.2,3
Immunosuppressants, including corticosteroids, cytokine-targeted therapies, monoclonal antibodies and antimetabolites, are commonly prescribed for a wide variety of chronic conditions such as inflammatory bowel disease (IBD) and rheumatological, neurological and dermatological conditions as well as for the prevention of solid organ rejection in transplant recipients. The prevalence of immunosuppressant use is difficult to ascertain; however, in the US it has been estimated at 2.7–6.2%.4,5 The rationale behind shielding advice for patients taking immunosuppressant medications is their increased susceptibility to viral infections in general. 6
However, due to the novel nature of COVID-19 there is a lack of available evidence about the specific risks of the disease in this patient group. Since the onset of the outbreak, governing bodies and professional societies have produced guidelines to support clinicians in the management of patients taking immunosuppressant medications – both for COVID-19-free patients in the community in the context of the pandemic and for patients with active COVID-19 disease. These guidelines and recommendations are mainly based on available evidence of viral illnesses in immunosuppressed patients, as sufficient evidence specific to COVID-19 is yet to emerge.
This article aims to systematically search the current guidelines available and summarize for clinicians in this area. We also highlight areas where further research is needed by critically appraising the literature cited in these guidelines.
Search strategy/methods
In light of urgent need for evidence synthesis, a focused review of published guidelines was carried out using internet search engines Google and Google Scholar, PubMed, and the websites of relevant national and professional societies, such as the National Institute of Clinical Excellence (NICE) and The British Society for Rheumatology. Search terms used included ‘immunosuppressants’ and its derivatives, ‘guidelines’, ‘COVID-19’ and ‘coronavirus’. Guidelines published in English for use by clinicians or healthcare professionals were included, but guidance or recommendations written and published for patients and the general public were not included. Guidelines which included recommendations for the management of patients who were routinely taking immunosuppressant medications were selected. All publications returned were published or updated between March 2020 and May 2020. The relevant data were collected from the full published guidelines and entered into a summary table. Searches were carried out on 16 May 2020 and rerun on 23 May 2020 to search for any new guidelines. The PRISMA flowchart for guideline inclusion is shown in Figure 1.

PRISMA 2009 flow diagram.
Two reviewers (FBP and TWH) independently assessed the guidelines, and discrepancies were resolved by consulting with another reviewer (PKM).
Public and patient involvement was not specifically sought as this is the review of existing evidence around the use of immunosuppressant agents.
Critical appraisal of guidelines
The following Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) Criteria (https://training.cochrane.org/grade-approach) were used to assess the level of evidence of individual guidelines. Level of evidence was classified as 1: 1a, Systematic reviews (with homogeneity) of randomized controlled trials; 1b, Individual randomized controlled trials (with narrow confidence interval); 1c, All or none randomized controlled trials; Level of evidence 2: 2a, Systematic reviews (with homogeneity) of cohort studies; 2b, Individual cohort study or low-quality randomized controlled trials (e.g. <80% follow-up); 2c, ‘Outcomes’ research; ecological studies; Level of evidence 3: 3a, Systematic review (with homogeneity) of case-control studies; 3b, Individual case-control study; Level of evidence 4, Case series and poor-quality cohort and case-control studies; Level of evidence 5: Expert opinion without explicit critical appraisal, or based on physiology, bench research or ‘first principles’.
We re-categorized the level of overall evidence included in these guidelines as very low (GRADE 5 evidence), low (GRADE evidence level 3a–4), moderate (GRADE evidence level 2a–2c) and high (GRADE evidence level 1a–1c). Where evidence indirectly related to COVID-19 has been generalized, it has been downgraded. For example, a cohort study on the susceptibility to viral infections (not specifically SARS-CoV-2) associated with immunosuppressant use has been downgraded from moderate to low. Where evidence was not cited to support recommendations, we have downgraded as very low, as it is likely to be an expert opinion.
Results
Twenty-three guidelines developed for clinicians managing patients taking immunosuppressive medications during the coronavirus pandemic were identified, of which 15 were from the United Kingdom, four from the United States, two from Australia and two were international guidelines.
Summary of individual guidelines
UK
The UK guidelines for patients on immunosuppressants in COVID-19 are summarized in Table 1. The NICE has issued several guidelines relevant to patients taking immunosuppressant medicines during the COVID-19 pandemic. NICE guideline 169 COVID-19 rapid guideline: dermatological conditions treated with drugs affecting the immune response 7 recommends that in COVID-19-free patients, a risk–benefit analysis should be performed when considering continuing the treatment with immunosuppressant agents or starting a drug which affects the immune system. For immunosuppressive therapies that require monitoring, it advises on ways to reduce hospital visits – either by reducing the frequency of monitoring or by choosing or switching to a drug which does not require monitoring. For patients with known/suspected COVID-19, it recommends that corticosteroids should not be stopped abruptly. Hydroxychloroquine, chloroquine, sulfasalazine, mepacrine and dapsone can be continued, whilst consideration should be given to stopping all other immunosuppressive agents including novel small-molecule immunosuppressants, biological therapies and monoclonal antibodies.
Summary of UK guidelines for patients on immunosuppressants in COVID-19.

Level of evidence 1: 1a, Systematic reviews (with homogeneity) of randomized controlled trials; 1b, Individual randomized controlled trials (with narrow confidence interval); 1c, All or none randomized controlled trials; 2a, Systematic reviews (with homogeneity) of cohort studies; 2b, Individual cohort study or low-quality randomized controlled trials (e.g. <80% follow-up); 2c, ‘Outcomes’ research; ecological studies; 3a, Systematic review (with homogeneity) of case-control studies; 3b, Individual case-control study; 4, Case series and poor-quality cohort and case-control studies; 5, Expert opinion without explicit critical appraisal, or based on physiology, bench research or ‘first principles’.44,45
Many professional societies in the UK, including the British Society of Gastroenterologists, Association of British Neurologists, British Transplant Society and British Society of Rheumatologists have produced guidelines relevant to their patient groups. Guidance from
The
This guideline has updated advice on shielding in October 2020; according to this update shielding has been paused in the UK; however, shielding may continue or be reinstated depending on local restrictions or lockdowns depending on the area.
The
The
General guidance for clinicians treating patients with systemic lupus erythematosus (SLE) or vasculitis is divided into the induction and maintenance phases of treatment. Regarding the induction phase, the RA guideline does not advise swabbing asymptomatic patients for COVID-19 prior to starting treatment but does state that patients should be triaged for symptoms and have their temperature checked. It advises that patients should complete the full induction regime, but when choosing an induction regime, the increased level of immunosuppression combined with additional hospital visits associated with cyclophosphamide should be considered as posing a potential increased risk to patients. Despite this, for vasculitis they recommend using IV rather than oral cyclophosphamide as it is associated with lower infective complication rates. Where IV inductions are not available, oral mycophenolate mofetil (MMF) is recommended due to lower risk for patients with an eGFR >15, instead of cyclophosphamide, and this is supported by a single non-inferiority trial. 18 Similarly, the guidance supports the use of MMF for induction regimes for lupus, informed by a systematic review of the literature. 19 If a rituximab regime is used it advises using one which is steroid sparing, a recommendation supported by a single prospective, single-centre, observational cohort trial. 20 In using steroids, it recommends reducing the dose as soon as possible to reduce risk of infection.
With regards to maintenance therapy, the guideline states that steroids should not be stopped abruptly and that patients who are infection free should continue their usual steroids, immunosuppressants and hydroxychloroquine. Clinicians are advised to consider reducing the frequency of rituximab infusions in patients whose risk of disease flare is low and risk relating to COVID-19 is high. The RA cite a single RCT, the MAINRITSAN2 trial, 21 to support the use of lower doses of rituximab regimes, though it acknowledges that there is currently no evidence that rituximab increases risk of COVID-19. In the event of COVID-19 infection the RA guideline advises individualized risk–benefit analysis ‘balancing the risk of inadequately treated disease, or acute relapse, against the risk of the effect of COVID-19 infection in the individual patient’. 17 Similarly, steroids should not be stopped abruptly, but the guideline also advises against the uses of high-dose steroids. Whilst the guideline cites several trials to support its recommendations on specific drug choices or dosing, it does not state the source of the evidence that has informed the more general guidance. Furthermore, the evidence used relates to infection risk in general and is not specific to COVID-19.
The
The MS-specific guideline 23 advises on each individual drug. It advises that interferon beta 1a, interferon beta 1b, glatiramer, teriflunomide and dimethyl fumarate are all safe to use and can be continued or started during the pandemic. It also recommends that natalizumab is safe to use as COVID-19 is not a neurotropic virus (although acknowledge a single case-report where COVID-19 was detected in cerebrospinal fluid) and extended licensing has been granted by NHS England so that it can be used for more patients in place of other, higher risk therapies during the pandemic. For fingolimod, the guideline recognizes a ‘moderately’ increased risk of COVID-19 but advises for patients established on the drug that it is likely that the risk of discontinuation and disease relapse is higher. Similarly, it advises the risk of COVID-19 is moderately increased with ocrelizumab, and it should only be used when the patient requires a high-efficacy drug but does not meet the criteria for natalizumab. For those on established ocrelizumab treatment, it is recommended that repeated infusions should be delayed where possible. A Swedish study looking at outcomes after interrupted rituximab treatment 24 is used to inform this recommendation. If the risk of viral infection is high in the first 3–6 months after starting alemtuzumab or cladribine, the guideline advises against commencing these drugs during the pandemic, and if a patient is already on these medicines the next round of treatment should be delayed. For patients with active COVID-19 infection, the guideline recommends that if symptoms are mild then disease-modifying treatments (DMTs) should not be withheld. In the event of more severe infection, requiring hospital admission, it recommends ‘pausing all injectables and oral medication, and delaying infusions’. Recommendations are detailed regarding reducing the frequency of blood test monitoring for all drugs. The ABN cited other guidance it has used to help inform this guideline, including that from the Italian MS Society and the European Society for Blood and Bone Marrow Transplantation.
The
United States
The American guidelines for patients on immunosuppressants in COVID-19 are summarized in Table 2. Comparable to the UK, professional societies in the US have produced guidance on the use of immunosuppressants in their patient groups. The
Summary of American guidelines for patients on immunosuppressants in COVID-19.
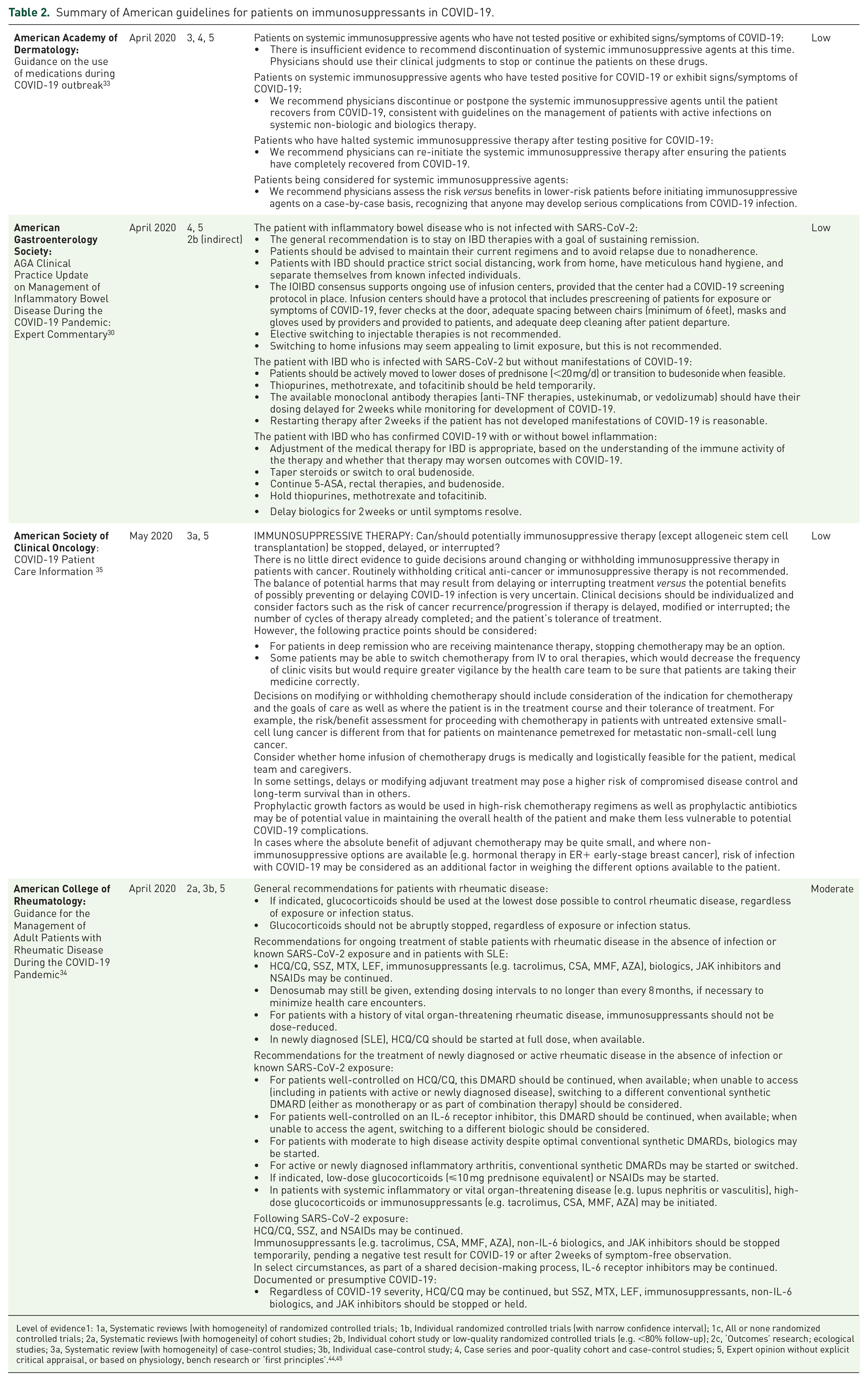
Level of evidence1: 1a, Systematic reviews (with homogeneity) of randomized controlled trials; 1b, Individual randomized controlled trials (with narrow confidence interval); 1c, All or none randomized controlled trials; 2a, Systematic reviews (with homogeneity) of cohort studies; 2b, Individual cohort study or low-quality randomized controlled trials (e.g. <80% follow-up); 2c, ‘Outcomes’ research; ecological studies; 3a, Systematic review (with homogeneity) of case-control studies; 3b, Individual case-control study; 4, Case series and poor-quality cohort and case-control studies; 5, Expert opinion without explicit critical appraisal, or based on physiology, bench research or ‘first principles’.44,45
In the patient with confirmed COVID-19 disease, the guideline recommends that thiopurines, methotrexate, tofacitinib, anti-TNF agents and ustekinumab should all be temporarily withheld, whilst systemic corticosteroids should be avoided and discontinued if possible. It advises that aminosalicylates and oral budenoside are safe and can be continued. There is some discussion regarding research into whether some drugs, such as anti-TNF agents, may be used in the treatment of COVID-19 as their anti-cytokine effects might prevent the progression to respiratory failure. The guideline acknowledges that this data is not yet available but refers readers to get up-to-date information from https://clinicaltrials.gov/.
The
In their publication ‘Guidance for the Management of Adult Patients with Rheumatic Disease During the COVID-19 Pandemic’,
34
the
The
Australia
The Australian guidelines for patients on immunosuppressants in COVID-19 are summarized in Table 3. The
Summary of Australian guidelines for patients on immunosuppressants in COVID-19.

Level of evidence1: 1a, Systematic reviews (with homogeneity) of randomized controlled trials; 1b, Individual randomized controlled trials (with narrow confidence interval); 1c, All or none randomized controlled trials; 2a, Systematic reviews (with homogeneity) of cohort studies; 2b, Individual cohort study or low-quality randomized controlled trials (e.g. <80% follow-up); 2c, ‘Outcomes’ research; ecological studies; 3a, Systematic review (with homogeneity) of case-control studies; 3b, Individual case-control study; 4, Case series and poor-quality cohort and case-control studies; 5, Expert opinion without explicit critical appraisal, or based on physiology, bench research or ‘first principles’.44,45
The Australian group, the
Other international guidelines
The international guidelines for patients on immunosuppressants in COVID-19 are summarized in Table 4. The
Summary of international guidelines for patients on immunosuppressants in COVID-19.

Level of evidence1: 1a, Systematic reviews (with homogeneity) of randomized controlled trials; 1b, Individual randomized controlled trials (with narrow confidence interval); 1c, All or none randomized controlled trials; 2a, Systematic reviews (with homogeneity) of cohort studies; 2b, Individual cohort study or low-quality randomized controlled trials (e.g. <80% follow-up); 2c, ‘Outcomes’ research; ecological studies; 3a, Systematic review (with homogeneity) of case-control studies; 3b, Individual case-control study; 4, Case series and poor-quality cohort and case-control studies; 5, Expert opinion without explicit critical appraisal, or based on physiology, bench research or ‘first principles’.44,45
The
Evidence summary of guidelines
A summary of guidelines and level of evidence base for these guidelines are presented in Tables 1–4. It also outlines details on recommendations for management of immunosuppressive agents during the COVID-19 pandemic. These guidelines were also critically appraised on their level of evidence-base on the recommendations and described as a final grade for the quality of evidence as ‘high’, ‘moderate’, ‘low’ or ‘very low’ based on the strength and quality of underlying evidence for the critically important outcomes based on the GRADE principles. Of the 23 guidelines included, 15 (65.2%) were graded as ‘very low’, three (13.0%) were ‘low’, and five (21.7%) were ‘moderate’. No guidelines were found to be underpinned by a ‘high’ level of evidence.
Discussion
This article summarizes international guidelines relating to the use of immunosuppressive medications for chronic conditions during the COVID-19 pandemic. On several points, there is general agreement amongst the guidance. For example, all advise against routinely discontinuing immunosuppressant medications in the absence of COVID-19 infection, and with respect to shielding guidance there is consistency regarding those who are at highest clinical risk. The guidance from the British Society for Rheumatology, British Association of Dermatologists and the Renal Association is summarized in Table 1, and all identify patients taking ⩾20 mg prednisolone/day for >4 weeks or ⩾5 mg prednisolone/day combined with another immunosuppressant, patients taking a combination of any two or more immunosuppressants, and patients who are taking cyclophosphamide, rituximab or another biologic as being most at risk. The Association of British Neurologists deviate here slightly, advising that an immunosuppressant medicine combined with ⩾10 mg prednisolone/day constitutes high risk whereby patients should be advised to shield. Whilst there is much consensus across the guidelines, there are discrepancies.
Logically, there are variances in the guidance from different medical specialties, due to the difference in relative risk that withholding immunosuppressive treatment would pose to the patient depending on the chronic condition for which they are prescribed. For example, discontinuation of immunosuppressive therapy for a patient with IBD could result in disease flare requiring hospitalization or emergency surgery,26,27 whereas discontinuation in a patient with a dermatological condition might result in a disease flare but is unlikely to lead to hospital admission or emergency intervention. This would perhaps explain why the British Gastroenterology Society and American Gastroenterology Association recommend that all patients without COVID-19 infection should continue their usual immunosuppressive therapies, whilst the American Association of Dermatologists recommend a risk versus benefit analysis for each individual patient when deciding whether to continue or withhold treatments during the coronavirus pandemic. The American guidelines for patients on immunosuppressants in COVID-19 are summarized in Table 2.
Given the novel nature of COVID-19, the guidelines draw on existing knowledge and data pertaining to the use of immunosuppressants and risks of serious infections of other aetiologies and have extrapolated these to form their evidence base. The Australian and international guidelines for patients on immunosuppressants in COVID-19 are summarized in Tables 3 and 4. Many guidelines drew on expert opinion including those from the Gastroenterological Society of Australia, the International MG/COVID Working Group and British Society for Rheumatology. Some guidelines have used more extensive methodology including systematic review of the literature and data from large RCTs, including those from the American College of Rheumatology and British Society of Gastroenterologists. However, even these guidelines have generalized data from studies on the effect of immunosuppressants on infection risk in general or in relation to other viruses. As a result, the highest level of evidence awarded to any guideline was ‘moderate’ and 78.3% (n = 18) of the guidelines were found to be informed by a ‘low’ or ‘very low’ quality of evidence.
This is a fast-moving field with emerging evidence regarding the hospitalization and mortality rate associated with immunosuppressant usage. For example, a prospective case series identified 86 individuals with underlying immune-mediated inflammatory disease who had either confirmed or highly suspected COVID-19 infection. Some 72% were receiving biologics or JAK inhibitors, and of these 16% were hospitalized with one death in the ED department and one developing acute respiratory distress syndrome and remaining on ventilation at the time of publication. The hospitalized patients were older, more likely to be on steroids or conventional DMARDS but less likely to be on a biologic or JAK inhibitors. 41 In addition, the Global Rheumatology Alliance – which is collecting data on COVID-19 cases in rheumatic disease patients worldwide – published its first report on 600 patients with underlying rheumatic disease who developed COVID-19 in May 2020. Some 46% of these patients were hospitalized and 9% died. Steroids >10 mg per day were associated with higher odds of hospitalization (2.05) whereas use of anti-malarials, NSAIDs, and conventional DMARDS either alone or in combination with biologics or JAK inhibitors were not associated with higher risk of hospitalization (OR 0.94, 0.64, 1.23, 0.74). Anti-TNF use was associated with a lower risk of hospitalization (OR 0.4) according to this report. 42 Finally, a UK population-based cohort study linked primary care electronic health records with COVID-19 reported deaths found a slight increase in risk of death in rheumatic diseases with HR of 1.17. This study reported that asthmatics who had required treatment with steroids within the last 12 months had a higher HR for death of 1.24 compared with 1.03 in those without steroids consumption. 43
There are several strengths to this study. We have systematically reviewed the currently available guidelines written in English on the use of immunosuppressive medicines during the coronavirus pandemic. Although we have found a wide range of guidelines available from professional societies and governing bodies internationally, some are lacking in specific detail that would aid clinicians, and we have also demonstrated that at present there is limited evidence to inform these guidelines.
This study has some limitations to note. As we only reviewed guidelines in English language there might be further published guidelines in other languages that were not included. This might explain why our search did not return any European guidelines, especially as given the urgent nature of our subject it is unlikely that English translations would be readily available. This manuscript is a systematic review of guidelines and hence is based on published guidance. We did not include original research papers in this review. In addition, at the time we accomplished this study, there were no published RCTs of immunosuppressive usage in COVID-19 and therefore no high-quality evidence was accessible to inform these guidelines. Consequently, the highest level of evidence awarded to these guidelines was moderate, and this was an inherent limitation imposed to our study. Therefore, our study is limited with regard to recommendation from the findings.
This systematic review has highlighted gaps and uncertainties regarding the use of long-term immunosuppressive medicine during the coronavirus pandemic. Areas where future or currently ongoing research could be directed include:
The relative risk of contracting SARS-CoV-2 in patients taking immunosuppressive medicines;
The clinical course of COVID-19 disease in these patients, including disease severity and mortality as compared with the general population;
The consequences of withholding immunosuppressive therapies at the point of diagnosis with COVID-19 disease, including whether that mitigates disease severity and improves outcomes or results in chronic disease relapse, with consequential morbidity and mortality.
Conclusion
New evidence surrounding COVID-19 is continually emerging and we would anticipate that some of these questions will be answered as the pandemic progresses. Following the publication of robust data and evidence, clinical guidelines on the subject should be reviewed and updated. In the interim, our rapid focused systematic review and critical appraisal of current international guidelines provide a useful resource for all clinicians who are managing patients who routinely use immunosuppressants for the benefit of patients and to help clinicians to make better decisions.
Supplemental Material
sj-doc-1-taw-10.1177_2042098620985687 – Supplemental material for Systematic review of immunosuppressant guidelines in the COVID-19 pandemic
Supplemental material, sj-doc-1-taw-10.1177_2042098620985687 for Systematic review of immunosuppressant guidelines in the COVID-19 pandemic by Fenella Barlow-Pay, Thura Win Htut, Mina Khezrian and Phyo Kyaw Myint in Therapeutic Advances in Drug Safety
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.