
Abstract
Background:
Review of clinical data on andexanet alfa for the reversal of factor Xa (FXa) inhibitor associated anticoagulation.
Data sources:
In the present review, we identified articles via PubMed using the combined keywords andexanet alfa, apixaban, enoxaparin, edoxaban, and rivaroxaban. Additional online searches via PubMed, Google Scholar, and Lexicomp were conducted for both prescribing and cost information. Portola Pharmaceuticals was contacted for information used for United States Food and Drug Administration approval of andexanet alfa.
Study selection and data extraction:
English-language clinical trials and reviews published between January 2008 and April 2019 were included for review. Bibliographies of selected articles were reviewed manually for relevant publications, focusing on reversal strategies for apixaban, enoxaparin, edoxaban, or rivaroxaban associated anticoagulation using andexanet alfa. Review articles were excluded.
Data synthesis:
The safety and tolerability of andexanet alfa were evaluated in one phase I, two phase II, and one phase III clinical trials. The use of andexanet alfa for reversing FXa inhibitor-associated anticoagulation were evaluated in the phase III ANNEXA-4 study.
Conclusions:
Studies evaluating laboratory parameters for coagulation show that andexanet alfa rapidly neutralizes the anticoagulant effects of apixaban, enoxaparin, edoxaban, and rivaroxaban. Clinical studies show that andexanet alfa improves markers related to coagulation, and reverses major bleeding in healthy volunteers and patients with life-threatening bleeding. Interruption of anticoagulation may result in thromboembolic and ischemic events. The use of andexanet alfa requires close monitoring for signs and symptoms of thromboembolic events, ischemic events, and cardiac arrest. Furthermore, anticoagulation should be resumed following the administration of andexanet alfa as soon as medically appropriate.
Keywords
Introduction
Factor Xa (FXa) inhibitors are approved for the prevention of stroke in patients with atrial fibrillation as well as the treatment and prevention of deep vein thrombosis (DVT) and pulmonary embolism (PE).1–4 A reversal agent for direct thrombin inhibitors was approved in October 2015, 5 but a reversal agent for the FXa inhibitors was lacking. Andexanet alfa was developed as a modified human FXa that is catalytically inactive and can bind up free plasma FXa inhibitors and decrease their activity. The United States Food and Drug Administration (FDA) granted accelerated approval for andexanet alfa on 3 May 2018 for reversal of apixaban and rivaroxaban. Currently, andexanet alfa has been shown to have a reversing effect on FXa inhibitors, although some areas of uncertainty still exist. While reviews of andexanet alfa have been published between 2008 and 2019,6–21 none include full data from the pivotal real-world trial of andexanet alfa. This article will review the data supporting andexanet alfa, encompassing all andexanet alfa clinical trials, including real world clinical use, and discuss implications for the clinical use of andexanet alfa.
Data sources and selection
Pubmed was searched using the keywords andexanet alfa and apixaban, rivaroxaban, edoxaban, betrixaban, or enoxaparin. English language articles assessing safety, pharmacokinetics, or reversing apixaban, rivaroxaban, edoxaban, betrixaban, and enoxaparin-associated anticoagulation, and articles published between 1 January 2008 and 30 April 2019 were included. Additional online searches via PubMed, Google Scholar, and Lexicomp were conducted for both prescribing and cost information. Bibliographies of selected articles were reviewed manually for relevant publications that focused on reversal strategies for apixaban-, rivaroxaban-, betrixaban-, edoxaban-, and enoxaparin-associated anticoagulation using andexanet alfa. Portola Pharmaceuticals was contacted for trial information used to gain FDA approval of andexanet alfa. A total of 84 articles were identified for this review, of which 7 met inclusion criteria and were utilized for this review. Review articles (i.e. nonprimary literature sources), as well as articles comparing all other anticoagulation reversal agents, were excluded.
Pharmacodynamics
Andexanet alfa is a recombinant modified human Xa coagulation factor that specifically binds FXa inhibitors such as rivaroxaban, betrixaban, edoxaban, enoxaparin, and apixaban.22–24 Andexanet alfa neutralizes the effects of FXa inhibitors by acting as a decoy protein; it is not catalytically active but has the ability to bind up FXa inhibitors with high affinity. 25 It can bind and sequester FXa inhibitors in the vasculature, thereby restoring human FXa and reducing the anticoagulant effect of FXa inhibitors. 26 It was also observed to bind and hinder tissue factor pathway inhibitor (TFPI), which is the first line of inhibition of blood coagulation, as well as blocking the early stages of the clotting cascade through binding and inhibiting factors VIIa and Xa.22,27
Pharmacokinetics
In a phase I study, 32 healthy volunteers were randomized in a 6:2 ratio to receive andexanet alfa or placebo in the absence of anticoagulation (Table 1). Plasma concentrations increased proportionally with increasing andexanet alfa doses, while the apparent volume of distribution at steady state decreased with increasing andexanet alfa doses. The mean apparent volume of distribution was approximately equivalent to the blood volume of 5 L. The area under the curve (AUC) increased proportionally with doses above 30 mg. Volume at the max dose and volume at steady state decreased with increases in dosing. Additionally, the mean terminal elimination half-life (4.35–7.5 h) and clearance (3.97–7.16 L/h) were similar with all andexanet alfa doses. Urine pharmacokinetic (PK) parameters for andexanet alfa could not be calculated as andexanet alfa concentrations in urine were below the limit for quantification. Andexanet alfa is not excreted in the urine of healthy patients. However, additional details concerning the metabolism and excretion of andexanet alfa remain unknown.22,28
Included studies.

Dose needed of andexanet alfa is higher to reverse the effects of rivaroxaban 20 mg once daily than that required to reverse apixaban 5 mg twice daily due to the stoichiometric ratio needed for reversal. 25
AUC: area under the curve/exposure, CL: clearance, Cmax: Maximum serum concentration, CV: cardiovascular, FXa: factor Xa, IV: Intravenous, Min: minutes, PD: pharmacodynamic, PK: Pharmacokinetics, t1/2: half-life, Vm: mean volume, Vss: volume at steady state.
Andexanet alfa pharmacokinetics were further evaluated in a phase II study consisting of 54 patients following steady state apixaban dosing of 5 mg twice daily for 6 days. Patients were randomized 2:1 to receive either Andexanet alfa or placebo in one of six cohorts (Table 1). PK parameters found were similar to those of phase I. 28
Factor Xa clinical trial review
Four studies were completed for andexanet alfa: one phase I and two phase II trials were performed in healthy adults, and one phase III trial was performed in patients where major bleeding occurred. Two additional trials are ongoing in patients taking FXa inhibitors, and one trial is expected to begin in 2019 that will be a randomized trial with a control group (Table 1).
Phase I study
Siegal and colleagues performed a phase I study that observed safety (including immunogenicity) and PK of andexanet alfa. It also measured D-dimer, a fibrin degradation product formed during the activation of the coagulation system, as a surrogate marker for thromboembolism. This study enrolled 32 healthy adults with no previous health history or remarkable laboratory findings. Subjects were randomized in a 6:2 ratio to andexanet alfa (n = 24) or placebo (n = 8); andexanet alfa was administered in one of four dosing cohorts (Table 1). Blood and urine samples were collected to assess the plasma concentration of andexanet alfa and the immunogenicity predose, after completion of the bolus, and on days 1, 20, 34, and 48 after dose completion; subjects were followed for 4 weeks. 28
All patients in phase I completed the study. There were dose-dependent increases in D-dimer and prothrombin fragments after andexanet alfa administration. The highest mean D-dimer was seen with the 600 mg dose (1.97 µg/ml). The highest mean levels of prothrombin fragment 1+2 levels occurred with the 300 mg and 600 mg doses (5157 pmol/L, and 7130 pmol/L, respectively); however, there was no evidence of thrombotic events. 28 While D-dimer can be indicative of a thromboembolism, it is not completely definitive; therefore, utilization of this surrogate marker alone to assess efficacy should be done cautiously.30–33
First phase II trial
Siegal and colleagues performed a phase II study to evaluate andexanet alfa’s safety, tolerability, PKs, and pharmacodynamics in patients who were anticoagulated with apixaban. Andexanet alfa was given as either a bolus, a bolus followed by a second bolus, or a bolus followed by a continuous infusion. 28 A total of 54 healthy adults with no remarkable previous health history or remarkable laboratory findings were enrolled and received apixaban 5 mg every 12 h for 6 days. The patients then received either andexanet alfa (n = 36, 9 in each dosing cohort of andexanet alfa) or placebo (n = 18) 3 h after the last dose of apixaban. Andexanet alfa and placebo were administered in six dosing cohorts (Table 1). 28
The outcomes of interest included pharmacodynamics of andexanet alfa [measured by anti-FXa activity, thrombin generation, prothrombin time (PT), activated partial thromboplastin time (aPTT), activating clotting time (ACT)], and unbound apixaban. 28 Prothrombin is a coagulation factor that, once cleaved by FXa, breaks down into thrombin and helps to promote coagulation in the coagulation cascade. 28
Following andexanet alfa administration, FXa inhibitor activity decreased significantly compared with the placebo group and pre-andexanet alfa dose (p < 0.05). The dose with the highest magnitude and duration of FXa inhibition was the seen in cohorts 3–6, which resulted in a reduction of 92.8–95% within 2 min of bolus administration. After andexanet alfa administration, FXa inhibitor activity returned gradually to placebo levels after 1–2.5 h in cohorts 1–3 and 3.3–4.3 h in cohorts 4–6. Administration of andexanet alfa in both cohorts 4 and 6 resulted in a sustained decrease of FXa inhibition. 28
Thrombin generation was restored to baseline (defined as levels prior to patients taking apixaban) within 2 min in a dose-dependent manner. Dosing led to a 67–100% restoration in thrombin generation. There was an insignificant dose-dependent decrease in the mean ACT roughly 2 min after any bolus of andexanet alfa in any of the dosing cohorts. 28
Andexanet alfa reduced the amount of free, unbound apixaban (up to a 90% decrease) in a dose-dependent manner within 2 min of the initial bolus across all dosing cohorts. Apixaban levels were lowered most after the bolus in cohorts 3–6. A sustained decrease in free apixaban occurred in cohort 6. Free apixaban returned to placebo levels within 0.17–3.5 h of bolus administration or bolus plus infusion. 28
Second phase II trial
ANNEXA-A and ANNEXA-R were studies of the safety and efficacy of andexanet alfa for the reversal of anticoagulation with apixaban and rivaroxaban, respectively. A total of 145 healthy volunteers were randomized in a 3:1 ratio for apixaban (ANNEXA-A) or a 2:1 ratio for rivaroxaban (ANNEXA-R). A total of 101 patients (48 in the apixaban study, 53 in the rivaroxaban study) received andexanet alfa, and 44 patients (17 in the apixaban study, 27 in the rivaroxaban study) received placebo. 26
A higher dose of andexanet alfa was used for patients receiving rivaroxaban due to the stoichiometric ratio needed for reversal (Table 1). 26 The primary endpoint for both studies was the percent change in FXa activity before and after andexanet alfa was administered. Efficacy was analyzed in the intent-to-treat population, and in those who had a baseline measurement of anti-FXa activity. 26
FXa inhibitor activity was reduced by 92–94% in the apixaban study, and by 81–103% in the rivaroxaban study, both within 2–5 min of administration of andexanet alfa compared with placebo in both the apixaban and rivaroxaban study (p < 0.001 for both). When administered with a continuous infusion, andexanet alfa reduced the inhibitory effects of FXa inhibi-tors to a greater extent than placebo in both studies (p < 0.001 in ANNEXA-A, and p < 0.001 ANNEXA-R). Thrombin generation increased to above the lower limit of normal (defined by the study as being the mean endogenous thrombin potential at baseline on day 1, plus or minus a standard deviation of 1) within 2–10 min of bolus administration in all the apixaban patients, and in 96% of patients in the rivaroxaban patients (p < 0.001); however, there were no clinical thrombotic events. 26
ANNEXA-4 (phase III study)
The ANNEXA-4 study was designed to evaluate the efficacy and safety of andexanet alfa in patients with acute major bleeding that was potentially life-threatening who were taking a FXa inhibitor. In this study, 352 people were enrolled in the safety arm, and of those, 254 were evaluated for the efficacy of treatment of major bleeding (defined in Table 2). Andexanet alfa was dosed according to the FXa inhibitor (or enoxaparin) that the patient was taking, as well as the timing of their last dose (Table 1). 23
Inclusion criteria for enrollment for acute major bleeding.

Patients were assessed at 4, 8, and 12 h after the end of the infusion; they were also followed for at least 30 days. Blood samples were obtained to measure anti-FXa activity and the free plasma concentration of the FXa inhibitor before and during andexanet alfa treatment, and at 4, 8, and 12 h after the end of administration. 23
The average age of patients enrolled in the study was 77 years; all patients had a history of thrombotic events or cardiovascular disease. Of the 352 patients included, 128 were receiving rivaroxaban (median dose of 20 mg daily), 194 were receiving apixaban (median daily dose was 10 mg), 10 were receiving edoxaban daily (30 mg in 5 patients, and 60 mg in 5 patients), and 20 were receiving enoxaparin at a dose of at least 1 mg per kilogram of body weight. The most common types of major bleeding prior to enrollment occurred in the gastrointestinal tract (26%) and intracranially (64%), which made up 90% of all patients enrolled. 23
Following administration of andexanet alfa, anti-FXa activity was reduced by 92%, 92%, and 75% from median value for apixaban, rivaroxaban, and enoxaparin, respectively, at the end of the bolus administration. In the efficacy group, 249 of the 254 patients could be evaluated for hemostatic efficacy (defined in Table 2), and 204 patients were declared to have excellent or good hemostatic efficacy at 12 h (171 had excellent hemostatic efficacy and 33 had good hemostatic efficacy). Some patients took the last dose of a FXa inhibitor 8 h or more prior to receiving the andexanet alfa infusion. Therefore, hemostatic efficacy was evaluated ⩾20 h from the last dose of a FXa inhibitor. The remaining 50 patients either could not be evaluated (5 patients) or were adjudicated to have poor hemostasis (45 patients). 23
Edoxaban, betrixaban, and enoxaparin
Currently, there are three ongoing trials regarding andexanet alfa’s use in edoxaban, betrixaban, and enoxaparin (Table 1). In one phase II double-blind, placebo-controlled trial, researchers observed the anticoagulation effects, PKs, and safety profile of andexanet alfa in patients taking edoxaban. Edoxaban was given as 60 mg daily for 6 days, and andexanet alfa was given on day 6, 3 h after the last dose of edoxaban. Andexanet alfa was given as either a 600 mg bolus, or a 800 mg bolus followed by 8 mg/min infusion for 1 h. After administration of 600 mg or 800 mg bolus followed by infusion, anti-FXa activity was reduced by 52% and 73%, respectively. Andexanet alfa was well tolerated with no thrombotic events, serious, or severe adverse events. 24
In another ongoing phase II, randomized, double-blind trial, patients took 80 mg of betrixaban daily for 7 days. Andexanet alfa was then administered either as 800 mg bolus 3 h after the last betrixaban dose (cohort 1), or 800 mg bolus 4 h after the last betrixaban dose, followed by a 2 h infusion (cohort 2). Following cohort 1, anti-FXa activity decreased from 29.9 ± 11.6 to 6.5 ± 4.5 ng/ml. Similar results were seen for cohort 2. Andexanet alfa was well tolerated and there were no adverse effects or thrombotic events. 29
In phase III (ANNEXA-4), 20 patients received enoxaparin and 10 received edoxaban. Of the 20 patients who received enoxaparin, 16 decreased their median value for anti-FXa activity from 0.48 international units to 0.15 international units at the end of the andexanet alfa bolus (75% reduction). Edoxaban activity reduction was not reported in the study; however, there is an extension of the study to gain more experience with edoxaban; this extension will be enrolling more patients this year. 23
Safety
In clinical studies, andexanet alfa was associated with mostly mild adverse events. There were no serious or thrombotic events reported. 26 One participant with a history of hives discontinued andexanet alfa administration prematurely due to developing hives, which resolved after a dose of diphenhydramine. 22 In the ANNEXA-A trial, the most frequent adverse events were flushing (4, 8%), and feeling hot (3, 6%). In the ANNEXA-R trial, the most frequent adverse events were flushing (2/53, 4%), and urticaria (1, 2%). Andexanet alfa has little immunogenicity after a single intravenous dose. Antibodies to factor X or FXa did not develop in any participants (measured through day 43), and neutralizing antibodies against andexanet alfa were not detected. Non-neutralizing antibodies were detected in 1 participant (2%) that received placebo and in 17 participants (17%) who received andexanet alfa (2 of these participants had non-neutralizing antibodies before andexanet alfa administration). Antibodies appeared within 15–30 days after andexanet alfa administration, and the titers generally remained low, at or below 1:640 in 18 participants, except for 1 participant who had a titer of 1:2560. Transient elevations in D-Dimer and prothrombin were noted, and generally returned to normal range within 24–72 h. 26
Safety data in the ANNEXA-4 trial included 352 patients, of whom 34 (9.7%) experienced one or more of the following thrombotic events within a 30-day follow-up period: ischemic stroke or stroke of uncertain classification (14, 41%), DVT (13, 38%), myocardial infarction (7, 21%), PE (5, 15%), and transient ischemic attack (1, 3%). Of the thrombotic events, 11 occurred within 5 days, 11 occurred between 6 and 14 days, and 12 occurred between 15 and 30 days after andexanet alfa therapy. Notably, all of the thrombotic events occurred before restarting anticoagulation. 23 It is likely that thrombosis could have resulted from a lack of anticoagulation rather than a rebound phenomenon. 34 Furthermore, andexanet alfa may block TFPI, which could lead to thrombosis.22,27 There were 49 deaths (14%) prior to the 30-day follow up visit, with 71% of those deaths due to a cardiovascular cause, 24% due to a noncardiovascular cause, and 4% due to an uncertain cause. 23 There were two patients in the ANNEXA-4 trial that experienced infusion reactions that were characterized as nonsevere. Furthermore, no antibodies to FXa or factor X, and no neutralizing antibodies to andexanet alfa developed. 23
The ANDEXXA package insert includes a pooled safety analysis of clinical trials in which 223 healthy volunteers received FXa inhibitors followed by treatment with andexanet alfa. The frequency of adverse reactions was similar in the andexanet-alfa-treated group (120, 54%) and the placebo-treated group (54, 57%). Infusion-related reactions occurred more frequently in the andexanet-alfa-treated group at (39, 18%) compared with the placebo group. The most common adverse reactions were urinary tract infection (>5%), pneumonia (>5%), and infusion-related reactions (>3%). 22
The package insert for ANDEXXA recommends monitoring patients for signs and symptoms of arterial and venous thromboembolic events, ischemic events, and cardiac arrest. Anticoagulation therapy should be resumed as soon as medically appropriate following treatment with andexanet alfa to reduce thromboembolic risk. Furthermore, the safety of andexanet alfa has not been evaluated in patients who experienced thromboembolic events or disseminated intravascular coagulation within 2 weeks prior to the life-threatening bleeding event requiring treatment. Safety has not been evaluated in patients who received prothrombin complex concentrates, recombinant factor VIIa, or whole blood products within 7 days prior to the bleeding event. 22
FDA indications, administration, storage, and stability
Andexanet alfa was granted FDA-accelerated approval on 3 May 2018, for patients receiving rivaroxaban and apixaban, when reversal of anticoagulation is needed due to life-threatening or uncontrolled bleeding.22,35
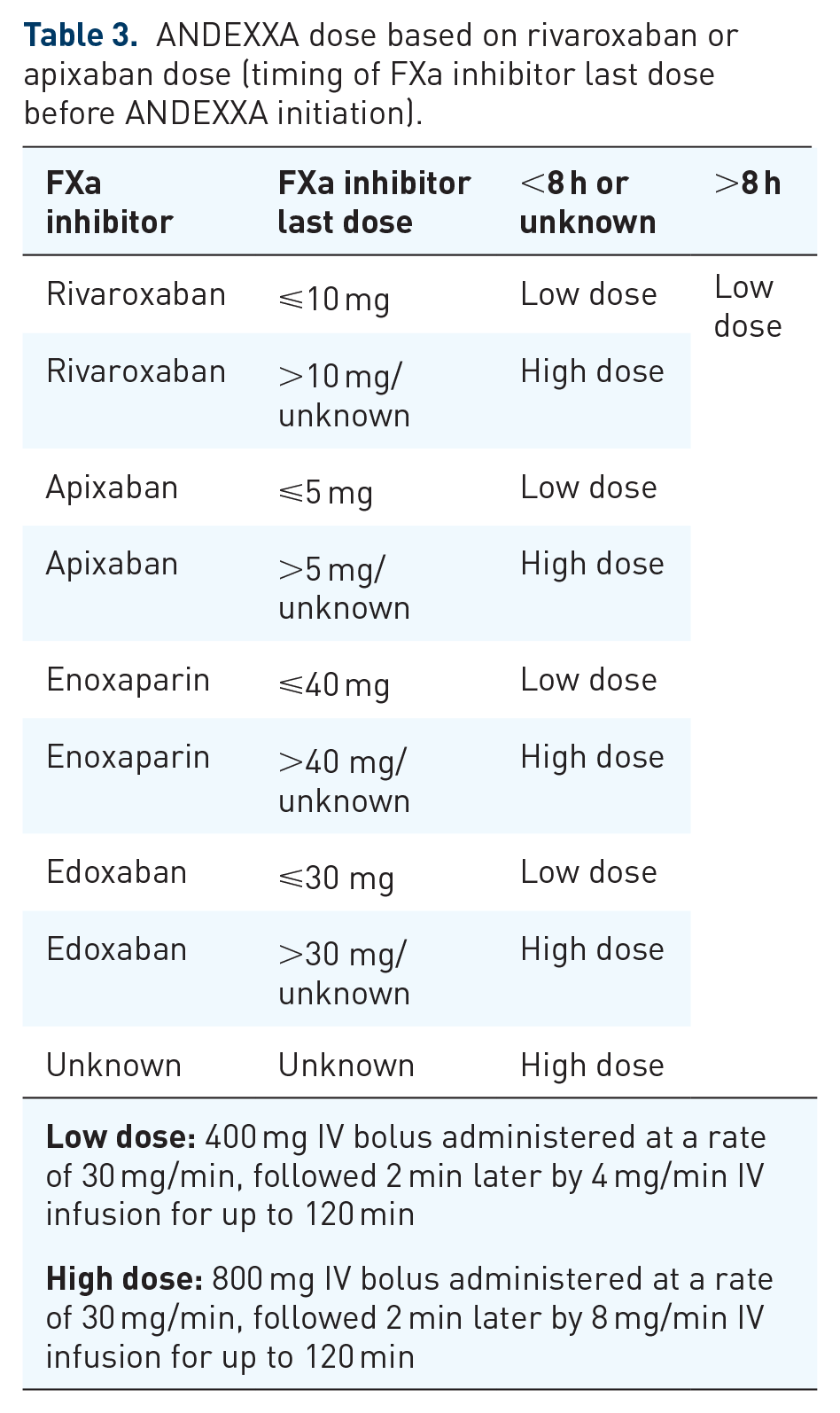
The recommended dose of andexanet alfa is based on the specific FXa inhibitor, dose of the inhibitor, and time since the patient took the last dose (Table 3). 22
ANDEXXA dose based on rivaroxaban or apixaban dose (timing of FXa inhibitor last dose before ANDEXXA initiation).
The drug is available in a single-use 100 mg vial at a concentration of 10 mg/ml. The product must be reconstituted before administration. The reconstituted product is stable at room temperature for up to 8 h (in the vial or in an IV bag), or for 24 h (vial) or 16 h (IV bag) at 2–8°C. 22
Andexanet alfa is recommended to be administered intravenously with a 0.2 or 0.22-micron in-line polyethersulfone or equivalent low protein-binding filter. The initial bolus should be started at 30 mg/min, and within 2 min following administering the bolus, the continuous IV infusion should be administered for up to 120 min. 22
Cost
The wholesale acquisition cost of one 100 mg vial of andexanet alfa is US $3300 in the United States. 36 Low dose therapy requires nine vials of andexanet alfa which costs $29,700. High dose therapy requires 18 vials of andexanet alfa which costs $59,400. An alternative reversal agent is a prothrombin complex concentrate product (Kcentra), which may be used off-label for the treatment of life-threatening hemorrhaging associated with nonvitamin K antagonists including apixaban and rivaroxaban at a dose of 50 units/kg with an additional 25 units/kg if clinically necessary, which costs $2.77 per unit. A single dose of 50 units/kg in a 70 kg patient cost $9695. Before any direct cost comparisons can be made, formal pharmacoeconomic analyses are needed to determine the true cost-effectiveness of these therapies.37,38
Areas of uncertainty
The role of andexanet alfa in patients who have been anticoagulated with edoxaban remains unclear. In the ANNEXA-4 study, 10 patients taking edoxaban did not have any FXa activity reduction reported; however, an extension of this study is continuing to enrol more patients this year in order to gain more experience with andexanet alfa use in edoxaban-related bleeding.
Additionally, the ANNEXA-4 study excluded patients who were scheduled for surgery within 12 h after presentation of a major bleed (with the exception of a minimally invasive surgery or procedure), as well as patients who received one of the following agents within 7 days before screening: vitamin K antagonist, dabigatran, prothrombin complex concentrate, or whole blood or plasma. 23 As surgical patients were not well studied in trials, it remains uncertain when andexanet alfa plays a role in surgery. Furthermore, severely bleeding patients were excluded from these studies, and the use of andexanet alfa in this population is still speculative.
Another important consideration is that andexanet alfa in the ANNEXA-4 trial was used mostly in patients with intracranial hemorrhages or gastrointestinal tract bleeds (totaling 90% of all patients studied). The inclusion criteria for enrollment for acute major bleeding is outlined in Table 2; however, additional criteria for an intracranial hemorrhage is that patients must have undergone a head computed tomography (CT) or magnetic resonance imaging (MRI) scan demonstrating the intracranial bleed. Any patients with an intracranial hemorrhage were excluded if they had a Glasgow coma score of 7 or less, or estimated intracerebral hematoma volume of more than 60 ml as assessed by CT or MRI scan. Further data will be needed to confirm whether the safety and efficacy profile is maintained for major bleeding at other critical sites.
The rebound levels of FXa inhibitors that were demonstrated in studies could lead to concern of returned risk of bleeding in patients; in studies, patients did not have a return in bleeding with rebound levels of FXa inhibitors. Furthermore, the studies of the PKs of andexanet alfa have demonstrated that there is a sustained reduction in FXa inhibitor activity during infusion. This also remains an area of uncertainty, as is to how to address rebound levels of FXa inhibitors.
Lastly, while andexanet can reverse the effects of unfractionated heparin, given the significant difference in cost relatative to protamine sulfate, its use in this setting is likely limited. Protamine sulfate incompletely reverses low molecular weight heparins (LMWHs), but andexanet appears to have some effects to reverse the anticoagulant effects of LMWHs; however, reversal of LMWHs was evaluated in a limited number of patients, and likely requires additional study to fully assess the safety and efficacy profile of andexanet before it is widely utilized.
Guideline updates
Andexanet alfa has recently gained FDA approval for the reversal of anticoagulation in patients treated with apixaban or rivaroxaban experiencing life-threatening or uncontrolled bleeding, and is not yet included in the national guidelines.
Off-label use
Andexanet alfa could be considered for use for enoxaparin-related major bleeding, as it has been shown in trials to reverse the effects of enoxaparin.
Conclusion
The ability to safely and reliably reverse the anticoagulant effect of apixaban, rivaroxaban, and enoxaparin with andexanet alfa is an important advancement in antithrombotic pharmacotherapy. Current clinical data supports andexanet alfa’s ability to reverse the anticoagulant effects of apixaban, rivaroxaban, and enoxaparin, but has also been associated with adverse thrombotic events in some patients. The results of the extended phase III ANNEXA-4 trial for the purposes of gaining more experience with edoxaban will further clarify the clinical benefits of andexanet alfa in patients requiring urgent reversal of edoxaban activity.