
Abstract
Background:
Iron deficiency anaemia in older adults is common, but its management presents unique challenges in diagnosis and management. Little is known about compliance with current best practice guidelines.
Methods:
We undertook an online survey of physician members of the British Geriatrics Society to ascertain how they managed older patients with potential iron deficiency anaemia.
Results:
There were 141 respondents (96% from UK). Almost a third indicated they would accept haemoglobin levels <100 g/dl without further investigation. A quarter said they would only occasionally or never check ferritin levels. Only 30% would sometimes or always use parenteral iron when oral supplements were not tolerated.
Conclusions:
Responses suggest a high level of variation in clinical practice and low adherence to best practice guidelines. Possible explanations include an inadequate evidence base to guide management and a lack of knowledge on the challenges of managing iron deficiency anaemia in this population.
Introduction
Anaemia affects approximately 15% of older adults, with iron deficiency accounting for 15–30% of cases. 1 The World Health Organisation defines anaemia as a haemoglobin level <13 g/dl in adult males and <12 g/dl in nonpregnant females, and currently there are no modified values for the older population. Diagnostic criteria for iron deficiency anaemia vary between published studies, although the serum ferritin is largely regarded as the best noninvasive test.2–4 However, ferritin in the older adult must be interpreted with caution since serum ferritin levels rise with ageing and with chronic diseases found more commonly in older adults. 5
Anaemia is associated with fatigue, impaired functional capacity, increased hospitalisation and mortality. A longitudinal health study for England of adults over 65 years old showed a 56% greater mortality hazard between men with mild anaemia (Hb 120–129 g/l) and an 87% greater mortality hazard for those with severe anaemia (Hb <120 g/l). 6 However, while this highlights the clinical importance of recognising anaemia, a recent systematic review found only three studies providing evidence on the use of oral iron supplements to treat iron deficiency anaemia in older people. The review reported that, whilst haemoglobin levels were raised, there was no evidence for discernible health improvements from oral iron replacement. 7 Furthermore, a review of the evidence for intravenous iron found no precise comparison of the clinical benefit of different iron preparations. 8
Current British Society of Gastroenterology guidelines recommend defining anaemia at any age using the lower range of normal for the laboratory performing the test. 9 They suggest all cases of anaemia should be investigated for iron deficiency, ideally using ferritin. Iron supplementation is recommended in all cases, using parenteral iron for those unable to tolerate oral supplements. No age-based recommendations are made. The guidelines recommend however that ‘special consideration’ be given to those with severe comorbidity. This is limited to advising that decisions on further investigation, particularly invasive tests to determine the underlying cause of iron deficiency, should be taken on a ‘case-by-case basis’. The degree of compliance with guidelines for iron deficiency anaemia in older adults, and the extent to which clinicians alter their management in older people, is unknown. Defining ‘usual care’ is also important for any future trial of iron replacement strategies in this population. Given the lack of evidence and guidelines specific to diagnosing and treating iron deficiency anaemia in older adults, we designed a survey to identify any variations in practice among clinicians involved in treating patients over 65 years old.
Methods
An online survey was designed in Survey Monkey, including questions covering participant job role, perception of threshold for investigation of iron deficiency anaemia and preferences for prescribing (see Appendix for full questionnaire). The survey was made available on the British Geriatrics Society (BGS) website (www.bgs.org.uk) for 2 months from October 2016. A link to the survey was included in a BGS electronic newsletter that was sent via e-mail to all BGS members that are opted in to this form of mailing. Participants had to be practising prescribers with an interest in care of older people. Consent from participants was implied by them proceeding to complete the survey after reading a covering letter. Anonymity of responses was maintained with no identifiable details recorded. Descriptive analysis of frequencies was performed using Survey Monkey’s own software.
Ethics approval was obtained from the College Ethics Review Board at the University of Aberdeen (Ref No CERB/2016/9/1383).
Results
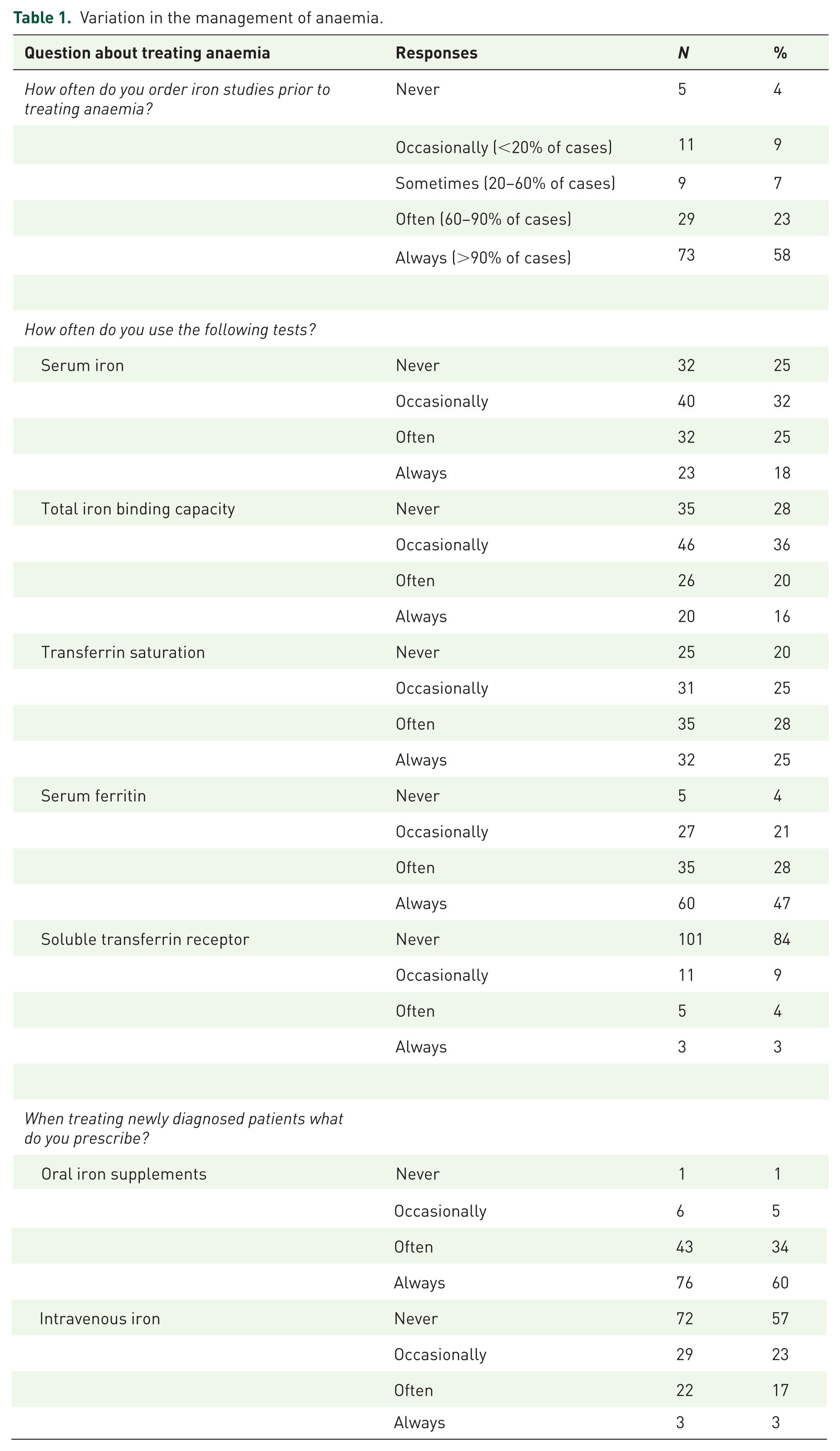
A total of 141 responses were received, comprising 85 consultants, 41 registrars (higher specialty trainees) and nine primary care practitioners (six respondents did not answer this question), with 96% working in the UK (48% England, 43% Scotland, 5% Wales). In response to the question, “what haemoglobin level would you regard as an acceptable lower limit in the absence of ongoing blood loss?”, around one-third of respondents indicated a value of less than 100 g/l for males and females (Figure 1). Of study respondents, only 57% said they would always order iron studies prior to treating for anaemia, with varying preferences for tests and initial treatment (see Table 1).

Perceived acceptable lower limit of haemoglobin.
Variation in the management of anaemia.
Half of respondents said they would often or always give verbal dietary advice to a patient with iron deficiency anaemia, with 11 (9%) often or always providing printed dietary advice and 19 (15%) often or always making a referral to a dietician.
Respondents varied in their approach to a failure of initial treatment either due to adverse effects of medication (Figure 2) or inadequate response (Figure 3). When asked if they would be happy to refer their patients to a hypothetical clinical trial of different management strategies after an inadequate response to oral iron (stop all treatment, continue oral supplementation or prescribe intravenous iron), most (105/119, 88%) replied they would and only 14 (12%) said they would not. The most common reason for declining to consider randomising participants into a future trial was a preference to replace iron in all such patients either orally [n = 11 (79%)] or intravenously [n = 1 (7%)], but two (14%) thought all such patients should discontinue all forms of iron supplementation indefinitely.

Action taken in response to side effects of oral iron.

Actions taken in response to a suboptimal response to treatment.
Discussion
This is the first study to highlight a high degree of variation in clinical practice in managing iron deficiency anaemia in older people, even amongst physicians specialising in the care of older people. The concentration of haemoglobin that physicians considered acceptable, and therefore not requiring investigation or treatment, varied greatly from 80 g/l to 120 g/l. This finding held true for both male and female patients, though most physicians had a higher acceptable minimum level for men. Moreover, physicians varied in how they investigated and treated anaemia, with only 57% stating they would always check haematinics prior to starting treatment, and 25% never or occasionally measuring ferritin levels. Physicians were particularly likely to vary in their ongoing management of iron deficiency anaemia where initial treatment has failed, with some choosing to continue oral supplements for longer, others stopping all treatment due to futility and only 30% sometimes or always opting for parenteral therapy, as recommended by best practice guidelines.
Identifying and minimising unjustified variation in practice has long been identified as integral to a safe and efficient healthcare system. 10 It seems unlikely that the wide range of differing practices identified in this survey would all result in similar patient experience and outcomes, or in the best use of resources. The finding that a high proportion of clinicians do not routinely measure ferritin or define the cause of anaemia is a surprising finding that is difficult to justify. This may reflect a lack of knowledge or over-reliance on mean cell volume to judge iron deficiency. It may reflect misinterpretation of clinical guidelines on investigation, which advise giving special consideration to further investigation of iron deficiency in frail people, but not in testing for iron deficiency itself. Clinicians may be variably aware of the benefits of measuring transferrin saturation, where ferritin is falsely elevated in iron deficiency due to disease. Although an exploration of the factors associated with this variation was outside the scope of this work, a key explanation may lie in the lack of evidence for best practice in this population. Important gaps in the existing literature include evidence for the optimal dosing regimen for oral iron, clarification of the best strategy for those not responding to oral iron, and establishing whether oral or IV iron therapy improves physical function and quality of life compared with no therapy in older patients with non-severe iron deficiency anaemia. 11 Although there is evidence of benefit of IV iron in numerous clinical conditions, trials have recruited mostly younger patients. Arguably, improved quality of life in elders has been found only in the context of heart failure in the FAIR-HF trial, which recruited mostly patients in late middle-age. 12 Some of the observed variation may reflect the heterogeneity and complexity of the case-mix encountered in geriatric medicine and a more holistic and person-centred approach to medicine, such that clinical management is not dictated by laboratory results, but by patient preferences. Nevertheless, misdiagnosis of the underlying type of anaemia may explain the high rates of treatment failure reported with iron supplements. 7
The survey findings should be interpreted with caution due to a number of limitations. Firstly, the population surveyed may not be representative of the general population of physicians as it relied on BGS members voluntarily visiting the website and completing the survey. However, most physicians specialising in the care of older people are members of the BGS and a response number of 141 out of approximately 2500 physician members is typical for this type of survey. Moreover, any selection bias is arguably more likely to reduce variation than to amplify it. Secondly, the survey gathered responses to hypothetical questions, so may not accurately reflect clinical practice in the real world. We mitigated against this by choosing simple questions on common clinical scenarios. Thirdly, since the survey was hosted on a public website, we cannot verify that all respondents were appropriately qualified.
The survey results nevertheless suggest a large proportion of clinicians do not undertake appropriate tests or provide appropriate treatment for iron deficiency anaemia. This highlights a need for greater consistency and better evidence of best practice in the management of iron deficiency anaemia in older people. This will require clearer clinical guidelines and potentially a programme of clinical audit and quality improvement. New research into the most appropriate management strategies in this population and improved education for clinicians on the causes of anaemia in older adults are also needed.
Footnotes
Appendix A: Questionnaire
Management of Iron Deficiency Anaemia in Older Adults
Please briefly explain the reason for your choice:
Comments
Acknowledgements
We would like to thank the British Geriatrics Society for hosting the survey link and formally endorsing the survey through its electronic communications. We gratefully acknowledge the participants of the survey.
Contributors
All authors contributed in design of the survey and interpretation of results. AICD and RLS drafted the paper and all co-authors contributed to writing of the paper.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.