
Abstract
Background:
This study explored the perspectives and experiences from patients and families around how patient/family preferences and priorities are considered in medication-related discussions and decisions within the healthcare system.
Methods:
We conducted a qualitative study using focus groups with residents of Southern Ontario and British Columbia (N = 16). Three focus groups were conducted using a semi-structured focus group guide. The audiotaped focus group discussions were transcribed verbatim. A thematic analysis, using inductive coding, was completed.
Results:
A total of three main themes [and several sub-themes (and sub-sub-themes)] emerged from the data: patient and family expertise [lived experience, information expert, and perceived expert roles (patient/family, healthcare provider)], perceived patient-centredness (relationship qualities of healthcare provider and assumptions about patients), and system (time, coordination and communication, and culture). Stories told by participants helped to clarify the relationships between the themes and sub-themes, leading to, what we understand as shared decision-making around medications and subsequent health outcomes.
Conclusions:
Our findings showed that shared decision-making resulted from both recognition and integration of the personal expertise of the patient and family in medications, and perceived patient-centredness. This is broadly consistent with the current conceptualization of evidence-based medicine. The stories told highlight the complex, dynamic, and nonlinear nature of shared decision-making for medications, and that patient priorities are not as integrated into shared decision-making about medications as we would hope. This suggests the need for developing a systematic process to elicit, record, and integrate patient preferences and priorities about medications to create space for a more patient-centred conversation.
Keywords
Introduction
The current population is aging, and as a result, the majority of patients seen in primary care now have more than one chronic condition, termed multimorbidity. 1 Multimorbidity is associated with polypharmacy, which is most commonly defined as taking five or more long-term medications. 2 In developed countries, polypharmacy is common; it has been estimated that older adults take a median of seven medications.1,3
While polypharmacy can benefit patients with multimorbidity, there are also potential harms, and the balance of benefits and risks may shift with increasing age.4,5 Polypharmacy can increase the complexity of medication regimes, increasing the chance of non-adherence.6,7 Polypharmacy is also associated with an increased risk of other harmful outcomes in older adults such as falls, unnecessary hospitalizations, and mortality.8–11 The evidence for benefit of medications may also shift or can become less clear with increasing age as the evidence itself may be different in older adults, and life expectancy changes may also reduce the potential to benefit. 12 Evidence in older adults may also change from the time a long-term medication is initiated for an individual as new studies emerge. Older age increases vulnerability to the adverse effects of drugs. 12 Polypharmacy is associated with an additional increased likelihood of adverse drug reactions due to the increased chance of medication–medication and medication–disease interactions. 13
Navigating the balance of the benefits versus harms of polypharmacy in older adults is complex as the majority of guidelines available focus solely on single conditions. The application of single disease guidelines in multimorbidity carry substantial risks of treatment harm from the ensuing polypharmacy. 14 Explicit tools and decision aids address some reported barriers to reducing the burden of polypharmacy identified in the literature (i.e. provider knowledge about inappropriate medications). However, despite efforts to address polypharmacy with such tools, the majority of these approaches are drug-based, and usually do not explicitly consider patient preferences or priorities. 15 Polypharmacy may include medications not covered by explicit tools and decision aids as these are not exhaustive and only focus on the most common drug-related problems. As a consequence, in individual patients, patient priorities become particularly important in making decisions, the literature indicates patients themselves use prioritization between treatments as a strategy for minimising their burden of treatment. 16
Shared decision-making is a mechanism that can be used to navigate the complexity of polypharmacy in clinical practice. In shared decision-making, both the health provider and patient discuss the evidence (the potential benefits and risks of each treatment option) and how the options align with patient preferences, values, and context. 17 This type of approach is congruent with one that is person-focussed, whereby an accumulation of knowledge about the patient and their needs can facilitate contextualized care over time. 18 A person-focussed approach improves health outcomes and is a core element of primary care.15,19,20
Studies have argued that current conversations around medications do not support this shared decision-making model, conversations often lack a bidirectional sharing of information.21–24 Further, it has been noted that providers assume they know what their patient’s preferences are in terms of medications. 24 We conducted a recent systematic review that examined processes to record patient priorities and preferences and demonstrated a lack of existing adequate processes to elicit, record, and follow up on patient preferences and priorities. 25 We found only one tool 26 centred on eliciting patient priorities and preferences in the context of multimorbidity, but nothing specifically about multiple medications. 25 One recent study piloted a systematic method to help older adults taking multiple medications incorporate patient priorities into care; and found this feasible; however, the effectiveness on patient outcomes has yet to be examined. 27
Little research has been conducted from the patient perspective in terms of their experience of shared decision-making around multiple medications. A qualitative study explored patient perspectives of older adults involved with decisions around their own medications and found only 1 of the 51 participants mentioned an awareness that priorities and preferences can, or should be, part of the conversion. 22 This study focussed on the patient–doctor relationship in medication decisions; however, decision-making about medication can involve others within the ‘team’ and often occurs in the broader context of the healthcare system.
The purpose of this study was to explore perspectives and experiences of patients and families involved in discussions around polypharmacy. Our ultimate goal was to understand how priorities are, and how they could be, considered in conversations about medications in the planning of patient care from the perspectives of patients and family members.
Research objective
The aim of this study was to explore the perspectives and experiences from patients and families around how patient preferences and priorities are considered in medication-related discussions and decisions within the healthcare system.
Methods
Study design
We chose a qualitative study design, using focus groups to gather data. We chose to use focus groups as we believed the nature of focus group discussion would generate richer participant-driven data over one-on-one interviews with a researcher. Further, we were sensitive to possible perceptions of power imbalance; the facilitators were family physicians and having a group of similar participants helps to remove possible perceptions of unequal power-relations given the ‘status’ of family physicians in patient–doctor relationships. We used a semi-structured discussion guide to prompt group discussion where necessary.
Participants
We recruited participants to represent different broad contexts, community-dwelling older adults, those living independently in care facilities, and those who were in long-term care facilities and not able to express their own priorities and preferences and therefore are reliant on families to fill this function (we chose caregivers of patients with dementia to represent this group). 12
We used a convenience sample, with purposeful selection of participants as described via advertising through the research teams’ community and clinical networks. Selection sought a range of participants in terms of polypharmacy based on number of medications, rather than limiting to particular kinds of medications so as to understand a diversity of experiences. We wanted diversity in terms of experience and not homogeneity. We aimed to capture varied perspectives based on different levels of family involvement, so we also sought participants who were caregivers of patients with dementia as we assumed that the use of multiple medications would be likely in such patients, and that caregivers would be involved in supporting medication management versus the patient alone. Although data saturation was not the end goal because we were interested in higher order themes, it was obtained.
Research team
The research team comprised two family doctors and four other primary researchers. DM has experience in medication research and CR is skilled in group facilitation and clinical communication. The four other researchers (LL, JL, JP, GS) have experience in assisting with polypharmacy research and experience in coding and thematic analysis. JT, a member of the patient advocacy focus group, was involved in a member checking process, detailed below. All team members operated under the belief that patient-centredness and patient engagement in practice and research is critical to advance knowledge and improve care. JT has been involved as a patient advocate as and an advisor within DM’s research program on deprescribing for several years.
Materials
Question guide
We used a semi-structured question guide (Table 1) to prompt discussion where necessary. We followed this structure to allow the research team to explore specific stories in more detail if necessary.
Question guide.
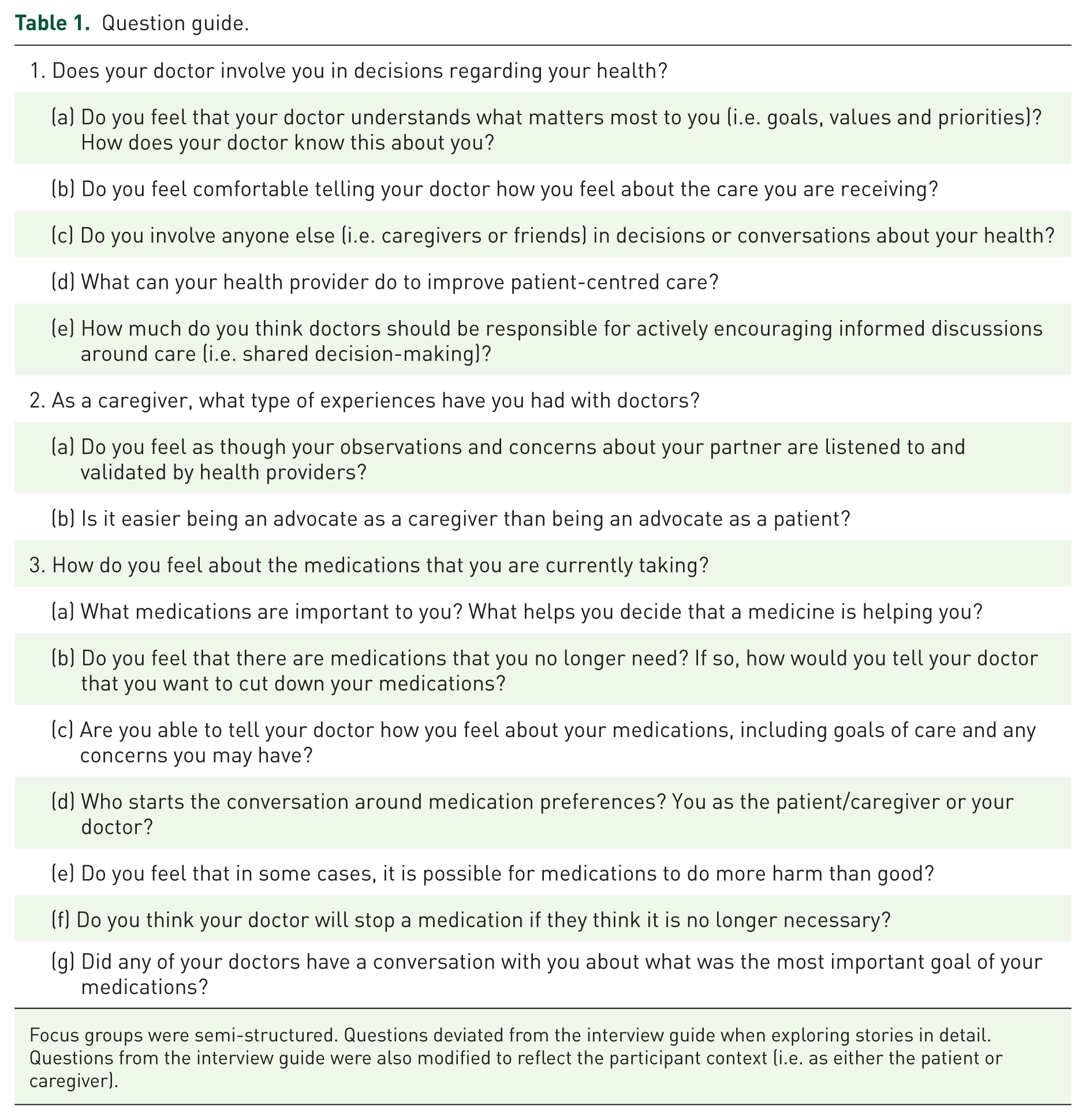
Focus groups were semi-structured. Questions deviated from the interview guide when exploring stories in detail. Questions from the interview guide were also modified to reflect the participant context (i.e. as either the patient or caregiver).
Procedures
After ethics approval (Hamilton Integrated Research Ethics Board #14-830), participants were recruited as described above. After expressing interest in the study, participants were scheduled for a 2-hour focus group over a teleconference phone line or in person. Prior to beginning the focus group session, written or verbal informed consent was obtained. All participants were compensated for their time with a gift voucher. A total of two focus group facilitators were present at each focus group (CR, DM), as well as a note taker (JP). All focus groups were audiotaped for later transcription.
Data analysis
We transcribed audiotapes verbatim, assigning pseudonyms to participants. We conducted a thematic analysis using procedures outlined by Braun and Clarke 28 to identify, analyze, and report patterns in the data (themes). LL and JL read and re-read the transcripts to familiarize themselves with the data. Transcripts were coded inductively; initial codes were identified and patterns which reoccurred were actively sought. We developed potential themes by sorting similar initial codes together. Flexibility was maintained in this step such that themes could be modified and refined until the most reasonable reconstruction of the data was completed. A final thematic map was developed and represents the structure of the data across all focus groups. 28
Consistent with Lincoln and Guba’s 29 recommendations, our coding process sought to ensure trustworthiness of the data. Overall, two coders (LL, JL) independently coded 100% of the data. The coders met after coding each focus group to discuss potential recurring themes. Disagreements were discussed during coding meetings and resolved after revisiting the data. Further, authenticity was maintained by displaying participant’s own words (as direct quotations) within the results section. The overall thematic map was challenged by other team members, who conducted the focus groups and then read and re-read the transcripts independently (CR, DM), resulting in the final thematic map.
We planned a collaborative form of member checking to enhance trustworthiness. 29 A draft of the manuscript and thematic map was sent to some members of the focus groups who gave us email addresses. We asked them to read the manuscript for clarity to confirm their ‘voice’ was accurately represented in the paper and findings. In places where they believed their voice was not represented, or misrepresented, they were asked to clarify this in writing to be considered when we challenged the thematic map for the final time. We have articulated such cases of nonrepresentation or misrepresentation under the heading member checking and incongruence.
Results
A total of 16 participants from Southern Ontario and British Columbia, Canada took part in this study. A total of three focus groups were conducted (focus group 1 and 2 each contained six participants, while focus group 3 contained four participants). One focus group was conducted via teleconference (audio only) and two focus groups were conducted in person. The participants’ age range was 55–90 years; 31% were male and 69% were female.
Participants described two levels of relationships relevant to medications, one with individual providers and the second with the overall healthcare system (i.e. how the individual relationships are contextualized in the overall system). We found that no themes were unique to one focus group.
Thematic map overview
Our thematic map (Figure 1) demonstrates the complexity and relatedness of the themes. It is clear that shared decision-making describes the core feature of the data (the centre). A total of two connected domains, perceived patient-centredness and patient and family expertise, were represented by puzzle pieces. It was apparent from the data that when two these pieces were present together in the discussion, shared decision-making appeared as an integrating process. This emergent process results from both patients/families and their healthcare provider bringing information, knowledge and expertise to the conversation around medications and subsequently enabling providers to support the patients in making decisions that align with their values and preferences. It was also clear from the data that when these pieces were not both present, shared decision-making does not occur.
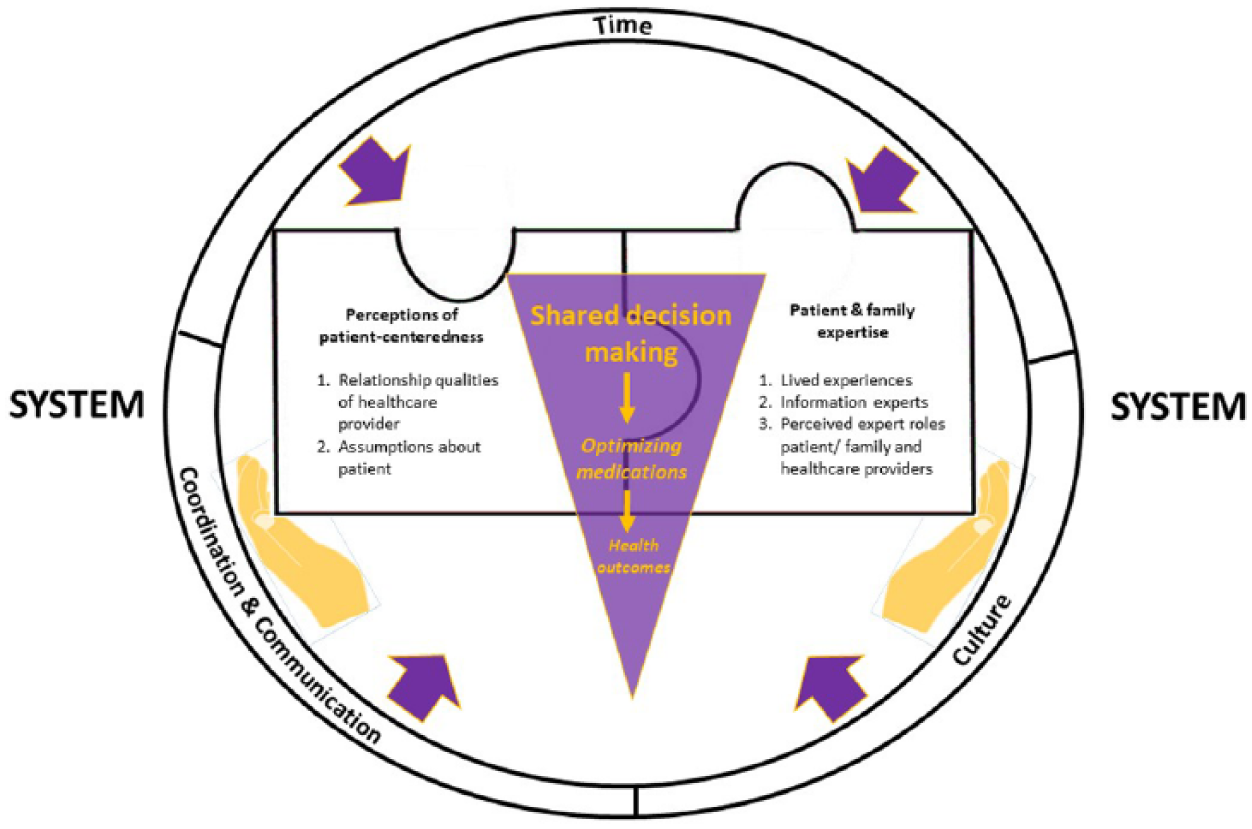
Thematic map: The patient and family voice in medication decisions.
The second layer of the data revolved around the larger system that gives context to shared decision-making. Components of the system, time, coordination and communication, and training, and culture, work as positive or negative forces on the shared decision-making process.
Related to this central feature of shared decision-making, three main themes (with related sub-themes) emerged from the data:
Patient and family expertise [lived experience, information expert, and perceived role as expert (both patient/family, healthcare provider)].
Patient-centredness (relationship qualities and assumptions).
System forces (time, coordination and communication, and culture).
Stories of optimal and suboptimal shared decision-making are detailed below to provide an in-depth understanding of how themes and sub-themes clarify relationships between the themes and sub-themes. Each theme and their sub-themes are delineated below.
Theme 1: Patient and family expertise
There was a clear consensus that patients and their families/caregivers have an expertise about medications and medication effects that is different from healthcare provider expertise, and that this adds to the quality of care if solicited and respected in some manner. In fact, there was almost an aura of pride associated with this expertise as demonstrated in discussions by participants detailing their knowledge about the medications they take. The word ‘advocate’ also appeared in the data several times in the advocacy as well as caregiver focus group, bringing emphasis and a sense of agency (versus a passive presence) to the decision-making for care. This theme was comprised of three domains: lived experiences, information expert, and the perceived role as expert (both patient and family and healthcare provider) which we describe below.
Lived experiences
The experience with chronic diseases, medications and medication regimens, observing the particular effects of drugs on themselves or loved ones, and navigating the healthcare system was a source of expertise believed to be important to care around medications. Participants felt that acquired lived experience of medication effects was important to understanding the patient. Don believed that the harm his wife experienced resulted from doctors not listening to his concerns about the medication his wife was prescribed: ‘that medicine did quite a bit of harm…I think this medicine actually killed my wife…I was told in January that she had dementia and by December she was dead. And September she could not speak anymore because of medication. She could not hold her neck. She could not raise her hands…’ He explained that, ‘the doctors have to realize the caregivers know the best. They are living with the person.’ (caregiver group).
Information experts
The majority of participants described their ability to seek out medication information on their own, evaluate the information in terms of validity or usefulness, and then bring it to their healthcare provider for discussion as a means to aid in the decision-making process. In fact, Sheryl called this type of patient a ‘patient researcher, a patient who is so informed,’ (patient advocate group). In most cases, this was a way for the patient to bring ‘their knowledge’ to the table for conversation. One participant offered a story which emphasized his data gathering skills combined with his desire to continue to be a long-distance runner, ‘So I came back armed with all of my data because at the time I was a competitive distant runner. And I just laid out all the points of why the new drug regime would not work with my running because there were multiple restrictions around food and liquid intake and timing and what have you. And he looked at me, he looked at my data, went okay I agree.’ (Keith, patient advocate group).
It should be noted that information, together with lived experience, was believed to be a strong source of expertise to help with making decisions around medications. For example, Whitney mentioned that ‘if I felt it was not doing the job or having side effects I would call and question it. Because I always read the glossary that comes with my new medications. And if I find that there’s something there that’s not quite right I would question the drug.’ (long-term care group).
Perceived expert roles
Overall, two distinct but related roles were clearly articulated in participant stories: both the patient or family’s perception of their own role as experts in decisions, as well as the patient’s/family’s perception of the role of the healthcare provider in decisions. That is, whether it was perceived that healthcare providers were the sole expert or whether it was perceived that the healthcare providers were a member of the team working alongside the patient.
A participant mentioned that patients/families need to understand that expertise comes from both the patient/family and the healthcare provider, ‘…what I’m finding still is that many patients and family members don’t want to ask questions because physicians, health professionals are trained. They know best…we need to be educating them [the patient/family] that its ok to ask questions…in terms of a refusal, if a specialist or family doctor offers you a drug which you already know is not a good idea… it’s ok to refuse and relook at it later.’ (Leanne, patient advocate group). The notion of becoming a patient expert, and in a sense, a patient advocate, was reflected in the patient advocacy focus group especially.
Some participants also described their perceived position in the patient–clinician dyad related to this. In some cases where a lack of honouring the patient/family expertise in care discussions was described, the word ‘advocate’ appeared. It seemed that a more explicit and present ‘side’ of the conversation (e.g. an advocate) was needed in one-sided discussions to make the patient/family ‘side’ heard. For example, when Keith’s mother was in critical condition in the hospital, the family was not being included in conversations and decisions about her care. Consequently, he decided to fly out to the hospital to advocate on his mother’s behalf.
‘And my sister says but I’m at my wits end, nobody wants to talk to us and now she’s being moved up to another floor for recovery but I’m not getting any sort of answers out of people. I said okay I’m on the first flight tomorrow.’ After arriving, Keith was able to speak with the hospital case worker and said, ‘… ‘we’re dealing with a person and everybody is a person that’s in a bed here in this hospital and we want the best care possible. So who as a family do we get to talk to, to resolve some of the issues because there’s lack of communication at all levels?’ (Keith, patient advocate group).
However, the ‘sides’ of the conversation, in some cases, do not need to be equal, as it is acknowledged by participants that healthcare providers have valuable expertise about care. This was especially noted among long-term care residents. For example, Whitney and Diana mentioned that they would trust the opinion of the healthcare provider simply because they are the specialist.
Theme 2: Perceived patient-centredness
The theme of perceived patient-centredness involved the sub-theme of relationship qualities of healthcare provider critical to developing care based on shared decision-making. Also, assumptions seemed to colour the relationship, either supporting or hindering shared decision-making. It should be noted that the term patient-centred was commonly used by participants.
Relationship qualities of healthcare providers
Several relationship characteristics reflecting patient-centred care were described by participants. Qualities included active listening, frank communication, validation, warm personality, friendly, sense of humour, using gestures which reflect open communication and invitation (i.e. ‘looking right at you’, ‘shakes your hand’, ‘says ‘hi’ and your first name’ [Shania, patient advocate group], asking ‘what do you want to talk about?’ [Leanne, patient advocate group]), these qualities foster trust in the relationship. It should be noted that these qualities were not specific to shared decision-making for medications.
(Provider) assumptions about the patient
This sub-theme represented the ideas or philosophy on the part of the patient/family as well as what they thought the provider’s assumptions about the patient might be, hence ‘provider’ is noted in parentheses. These assumptions revolved around philosophy about medications, providers’ expertise and knowledge about medications, older adults, and roles of the patient/family and the provider in decision-making. For example, Leanne described an assumption a provider had about older adults, she said, ‘[The doctor] said well unfortunately what happens when patients come in my door and go to leave they expect to have a prescription that will deal with whatever symptoms they got’ (patient advocate group). Martina mentioned that although she expected a prescription, she was open to a conversation about why this may not be the best option; thus, assumptions may prevent a conversation about alternative options for medications at the outset (patient advocate group).
Theme 3: System forces and structure
It was clear that shared decision-making for medications did not operate in a vacuum. It was acknowledged by the majority of participants that the system in which the relationship exists functions in the larger healthcare system and that forces such as time, coordination and communication, and culture, facilitate or hinder the relationship, and ultimately shared decision-making. Given that this outer layer of the thematic map included decision-making around medications and those around general care, we have highlighted those findings with respect to medication shared decision-making.
Time
A system with a time-limited medication conversation for care was a common theme among participants. Shania noted that ‘the physician needs time to be the detective and look at the clues and start to sort out well okay this is, it might even be a result of a new medication I’m on,’ (patient advocate group).
Coordination and communication
Patients and caregivers often expressed that a lack of coordination and communication existed among healthcare providers, which often represented fragmented care or multiple individual disease-focussed care that was not well integrated and left patients and caregivers as the primary coordinators of care, which included medication management. A participant (Keith) even mentioned, ‘…so we’re really not doing patient-centred care, we’re doing silo care and that’s the issue.’ (patient advocate group).
Culture
Some participants noted a shift in culture around prescribing. In talking about deciding treatment for glaucoma, Sheryl said, ‘[I] basically told the eye specialist that I was not willing to go on drugs for it and that I would continue to monitor it. And he told me that when he started out as a young doctor, oh I don’t know 20 or 30 years before, he said he would have tried to insist or scare me into taking the medication. But that he wasn’t going to do that, and it was up to me to make that decision.’ (patient advocate group).
The sub-theme of culture was also related to beliefs about quantity versus quality of life and whether or not a medication is necessary to prolong life when it does nothing for quality of life. In fact, Paul changed family doctors and the first question that he asked was ‘what’s your philosophy?’ (caregiver group). This led to a common understanding that he and the doctor shared the same philosophy in terms of taking necessary medication for quality over quantity of life meant that there were no problems with overmedication. There was a firm consensus across groups that medications should be necessary for quality of life, and if there was no benefit, then discontinuing it was desired.
Connection between themes: Lack of shared decision-making
Don’s story illustrates the connection between and among these themes of the data: ‘And I say that my wife suffered unnecessarily. And that as I, as a caregiver could see the decline with that type of medicine. The doctors did not listen and said it was dementia disease. I was very unhappy as [my wife] suffered unnecessarily and I was myself, was very unhappy because I suffer with her. And I said and even after the doctor realized it was the medicine that was all the effect, they didn’t even have the courtesy of admitting…As I say you can see the dates because see my notes are all down on one spreadsheet where I was watching. I had been doing it. I had been highlighting things I was very, very concerned about. I personally want to talk, I talk to the doctors, not working. It’s doing a lot of harm. Just totally ignored me. So, what I’ve done I take, took this yesterday and then I, because I didn’t want it to get, in hindsight also I’m a little bit more educated because I could see as they took away the medicine and then I could rely which medicine was affecting, what it was doing. So, I tried to put it separately so it’s easier. But as I said I wasn’t very happy, but another thing is one of the medicines, this medicine, galantamine, I think that’s a bad medicine. Whatever this thing made my wife suffer. As I say she was basically paralyzed because of medicine. And again, I put that information here. And the specialist, Dr X had said that she should have not been on the medication. He said that medicine doesn’t work at all. When you have specialists saying it doesn’t work and here you have another specialist it doesn’t make sense. And when I came and told the doctor, the doctor, the specialist, actually Dr X told me to take off the medicine and stop right away. At least he, I was happy what he told me so that’s what I wanted.’ (caregiver group).
This story highlights the interaction between patient/family expertise (lived experiences, information expert) and patient-centred relationship qualities [relationship qualities (listening), and assumptions about the disease versus medication side effects] in a way which undermines shared decision-making. This story also highlights the pressures and influences on the ability to engage in shared decision-making within a system that lacks clear communication and coordination.
Member checking and incongruence
We sent the draft paper and our findings with the thematic map to focus group participants from the support group and a participant from the patient advocacy group. It should be noted that two of the four participants we had email addresses for from the support group could not be reached (email bounced back). Overall, one person did not have time to review the paper, and another person did not respond with any comments. JT from the patient advocacy group responded on behalf of the group with feedback on clarity of the manuscript and strengthened the language of the conclusion. She noted no incongruences (i.e. participant voice was accurate in its representation within the results).
Discussion
This study explored the perspectives of patients and families about how patient preferences and priorities are considered in medication-related discussions and decisions within the healthcare system, in particular related to polypharmacy.
The core operating concept that emerged from the data was shared decision-making. Shared decision-making is defined in the literature as a health decision made by both the healthcare provider and patient. It is a decision that involves a discussion of treatment options and the potential benefits and risks of each option, as well as how these options align with patient preferences, values, and context. 17 Our findings showed that shared decision-making for medications resulted from patient perceived integration of patient/family expertise and experience of medicines and patient-centred care. This type of process is unlike reductionist models of evidence-based medicine (EBM) operationalized in guidelines, whereby the focus is to identify clinical problems and subsequently find and implement treatment based on the best available evidence. 30 In a broader model of EBM, a clinician uses their expertise to evaluate information, but the model also works to incorporate the clinical state of patients, patient preferences and values along with research evidence to inform clinical expertise. 31 The process of shared decision-making is critical for this to work effectively. Our findings provide some understanding of the patients and family perspective on this shared decision-making process element of the EBM, an area currently under-studied in the literature. This study builds on the work of Belcher and colleagues, 22 broadening the perspective beyond the patient to include family views and system issues.
Our findings challenge some of the assumptions found within a clinician-only perspective. 32 Specifically, clinicians make assumptions about a patient’s ability and desire to participate in shared decision-making, 32 and often report that their patients want a less active role in healthcare decisions;32,33 whereas our results show that the majority of patients and caregivers wanted an active role in making medication decisions. This is consistent with the literature stating that patients want to be more engaged in healthcare decisions. 34 However, it should be noted too that some patients in our study mentioned wanting a less active, or flexible role in some decisions, termed optional autonomy such that patients should be engaged in decisions to the extent that they wish to do so. 35 The participants in our study described ways in which priorities, preferences and patient expertise may enter conversations about medications.
Despite the benefits of shared decision-making, it has not been widely adopted systematically into routine clinical practice around medications.17,32 Our findings, consistent with other work, suggest that it is not a simple process with a set of linear steps to follow but should be viewed as a continuum, with many possibilities of patient participation along this continuum. 17 Our findings with respect to the system add to the complexity of this process, consistent with research which highlights the fragmented nature of coordination of care in the overall healthcare system. 36
Our results also suggest there is an active process of reflexivity, where individuals think about their perceived position in the patient–provider dyad. Research suggests that a conversation needs to take place in order to address potential power imbalance37,38 yet, to our knowledge, no research to date has unpacked the language commonly used to identify these ‘conversations’. Using language to truly represent partnership, collaboration, and team is one that challenges the notion that medical professionals hold all the power in decisions and may be a key element in facilitating integration of patient expertise and experiences. This may be particularly critical for patients who do not have the high levels of knowledge and education about medications and the healthcare system. Participants in the current study acknowledged the expertise and knowledge of the medical community, and instead of pitting one expertise against another, see integrating the expertise and experience of patients/families with medicines and the expertise and knowledge of clinicians into a process of shared decision-making as the desired way of care.
We suggest that having a systematic process to elicit, record, and integrate patient expertise/experience, preferences and priorities about medications creates an ongoing space for patients or caregivers to participate in shared decision-making. Having such a space may be particularly important for patients who may have a different level of privilege (and power), health literacy or understanding of the healthcare system. This ‘space’ gives permission for bringing one’s expertise to the conversation and may reduce the perceived burden of having to negotiate power or making decisions around medications. Developing a system whereby such priorities and preferences are also followed up during care and medication decisions is critical, considering the complex, iterative and nonlinear nature of shared decision-making about medications. Such a system could consider time and culture factors articulated by participants. Despite efforts to address polypharmacy with explicit, criteria-based tools (some computer-assisted), or implicit, judgment-based tools, 12 the majority of the approaches do not explicitly consider patient preferences or priorities. 25 One exception to date is Naik and colleagues, 27 which demonstrated feasibility, but has yet to demonstrate effectiveness of the process.
Several limitations should be highlighted. We need to acknowledge that this study was from the perspective of the patients and their families. Further, findings with respect to the healthcare provider were those from the perspective of patients and their families. The healthcare provider perspective of shared decision-making in terms of medications is also valuable and critical to the overall understanding of how patient priorities and preferences should be integrated into conversations about medications, especially in terms of the EBM model. It would be naïve to think that understanding can be achieved through one perspective. Research has identified barriers to conversations about medications at the healthcare provider level, 39 however, how to overcome these barriers is not yet realized in a systematic way. Our findings emphasize the need to consider the voice of the patient and their families and flag a clearer avenue to achieve this from the perspective of the patients and their families.
It also should be acknowledged that polypharmacy can occur at any age, although our participants were aged 55–90 years old, our focus was older adults and findings may be not transferable to younger age cohorts with polypharmacy, or those with other types of caregivers (i.e. a young child on multiple medications). Further, research should explore the universality of this model of shared decision-making for medications in other sub-groups of patients who have demographic or medication characteristics which may impact the nature of the conversation. We used a convenience sample and purposeful selection of participants and so our findings may not be transferable to all experiences. We attempted to incorporate collaborative member checking; however, only one participant responded and noted no instances of incongruence; rigor may have been strengthened had we heard from other participants. Further, we did not record medication information and so cannot confirm our sampling resulted in a variety of people; however, our data do suggest we captured a variety of perspectives.
Conclusion
Our findings highlight the importance of the core operating feature of shared decision-making from the perspective of the patient and family members, a viewpoint currently under-studied in the literature. Our findings demonstrate the core elements necessary for shared decision-making to occur, in particular patient expertise and experience with medication use, and a patient-centred relationship. These results support the development of more routine systematic processes to create conversational space, solicit patient expertise and experience, document and follow up on patient and family preferences and priorities for medication use, so these may be effectively incorporated into medication-related decisions.
Footnotes
Acknowledgements
We would like to thank all participants in the study. Without their willingness to share their insights this would not have been possible. We would also like to thank Amen Awan for her work in proof reading the paper and overall work on our research program.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported with funds from the David Braley and Nancy Gordon Chair in Family Medicine.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.