
Abstract
Background:
Atypical antipsychotics (AAP) have been associated with reduced duration of delirium in the intensive care setting. However, long-term use of these drugs is associated with significant adverse events, including increased all-cause mortality in the elderly. Inappropriate continuation of AAPs after discharge from the intensive care unit (ICU) is worrisome and needs to be addressed.
The aim of this work was to assess the prevalence of continuation of AAPs after hospital discharge and evaluate the associated risk factors.
Method:
This was a single-center retrospective chart analysis in the setting of adult ICUs at a tertiary care academic medical center. It involved all adult patients admitted to the ICU and initiated on AAPs from January 2012 to December 2014. The measurements were: (1) prevalence of ICU-initiated AAP continuation following hospital discharge, (2) risk factors associated with continuation of AAPs following hospital discharge, and (3) risk of continuation of AAPs in patients ⩾65 years of age.
Results:
A total of 55% of ICU patients initiated on AAPs were discharged from the hospital with a prescription for continued AAP therapy. Male sex and discharge location were highly associated with continuation upon discharge. Older patients (⩾65 years of age) were not at a higher risk of being continued on these drugs after discharge.
Conclusion:
Male sex and discharge to a healthcare facility were associated with a higher rate of continuation. Research into practical methods to reduce their continuation upon discharge should be performed to mitigate the long-term risks of AAP administration.
Introduction
Inappropriate continuation of drugs initiated in an intensive care unit (ICU) is common, particularly in the elderly population. 1 The transition of care from the ICU to other locations puts patients at a high risk for medication errors, 2 and improper medication reconciliation at discharge is a likely contributor. The medications most commonly associated with inappropriate continuation are inhaled bronchodilators and proton pump inhibitors. 3 However, with the increase in use of atypical antipsychotics (AAPs) for the treatment of ICU delirium, continuation of these drugs after hospital discharge is on the rise. 4
ICU delirium, a syndrome of disrupted cognition, inattention, and altered mental status, is a common occurrence in critical ill patients with a prevalence approaching 80%. 5 ICU delirium has been associated with increased mortality, increased ICU and hospital length of stay, reduced ventilator-free days, and increased overall hospital costs.6–10 The onset and duration of delirium is also predictive of long-term cognitive decline. 11 The most recent guidelines from the Society of Critical Care Medicine endorse routine monitoring for delirium in all adult ICU patients and recommend, albeit with a level C evidence, the use of AAPs in reducing the duration of ICU delirium. 12 The use of AAPs, however, is associated with short-term risks of QTc interval prolongation and extrapyramidal side effects (including malignant neuroleptic syndrome) as well as long-term risks of weight gain, hyperlipidemia, new onset diabetes mellitus, increased mortality in patients age 65 years and older, and higher rates of long-term institutional care.1,13–16
In this clinical retrospective investigation, we sought to quantify the number of ICU-admitted patients initiated on an AAP and the prevalence of AAP continuation on discharge. We hypothesized that patients discharged to advanced care facilities would be more likely to be continued on an AAP prescription. Secondarily, we sought to determine the independent risk factors for continuation of AAP upon discharge to home or advanced care facilities.
Methods
Study design
After review and approval from the institutional review board (study no. 00000628, approval: July 11, 2014), a retrospective analysis of electronic medical records (EMRs; Cerner Corporation, North Kansas City, MO, USA) was performed for all patients admitted to the adult ICUs at Penn State Health Milton S. Hershey Medical Center, a tertiary care academic medical center between January 2012 and December 2014. The study team consisted of intensivists, pharmacists, a statistician and trainee physicians. The inclusion criteria were as follows: age greater than 18 years, admission to one of the four adult ICUs (surgical, neuroscience, medical, and heart and vascular), and documented AAP administration in the ICU. Patients who were taking AAPs prior to admission were excluded from the analysis. No daily detection of delirium was ongoing during the study period.
Data collection
Admission and discharge medication reconciliation as well as AAP initiation data were extracted from the hospital pharmacy database. Physician documentation of delirium was determined using the hospital billing database. Individual review of patient charts was conducted for any discrepancies that were noted. Collected variables included age, sex, ICU type, ICU length of stay (LOS), hospital LOS, AAP regimen, discharge disposition (home, expired, advanced care), and presence or absence of delirium in the patient’s electronic medical record. AAP included in the analysis were aripiprazole, olanzapine, quetiapine, risperidone, and ziprasidone. Patient EMRs, as well as external pharmacy fillings, were reviewed to evaluate whether the patients were using AAPs prior to admission. The EMRs of patients who survived to discharge were then reviewed to determine if the AAP was continued or discontinued upon discharge from the hospital.
Outcomes
The primary outcome was the discharge location of patients continued on AAP upon hospital discharge in patients initiated on AAP. Discharge locations were to home or an advanced care facility (skilled nursing facility, long-term care facility or nursing home). Secondary outcomes included continuation of AAPs in patients ⩾65 years of age compared with <65 years old and sex differences in AAP continuation. We analyzed other factors associated with AAP continuation, including hospital and ICU LOS, ICU location (surgical, trauma, neuroscience, medical, cardiovascular), and the presence or absence of physician documentation of ICU delirium during the ICU LOS.
Statistical analysis
All variables were summarized, and the distributions of continuous variables were assessed using histograms and normal probability plots. We then used a Chi-square test to look for statistical associations between age ⩾ 65, sex, ICU type, discharge location, and prescribed AAP. We subsequently used a two-sample t test to examine the difference in mean age between the patients continued versus discontinued on AAPs. A Wilcoxon rank sum test was performed to evaluate the difference in median hospital or ICU LOS between the same groups. Finally, we included all of these variables in a multivariable model with continued AAP after discharge as the outcome variable. From this model, we generated adjusted odds ratios (ORs) for all of the recorded predictors. We tested for interactions between all predictors in the model, but none were significant. Multicollinearity of the predictors was tested using variance inflation factor statistics. The Pearson, deviance, and Hosmer–Lemeshow goodness-of-fit tests were used to test the fit of the adjusted multivariable model. All analyses were performed using SAS Software, version 9.4 (SAS Institute, Cary, NC, USA) and significance was set at p < 0.05.
Results
Between January 2012 and December 2014, 12,984 patients were admitted to the four adult ICUs, of which 346 (2.66%) were newly initiated on an AAP during their ICU stay. Of the 346 adult patients started on AAPs, 32 died prior to discharge from the hospital (Figure 1).
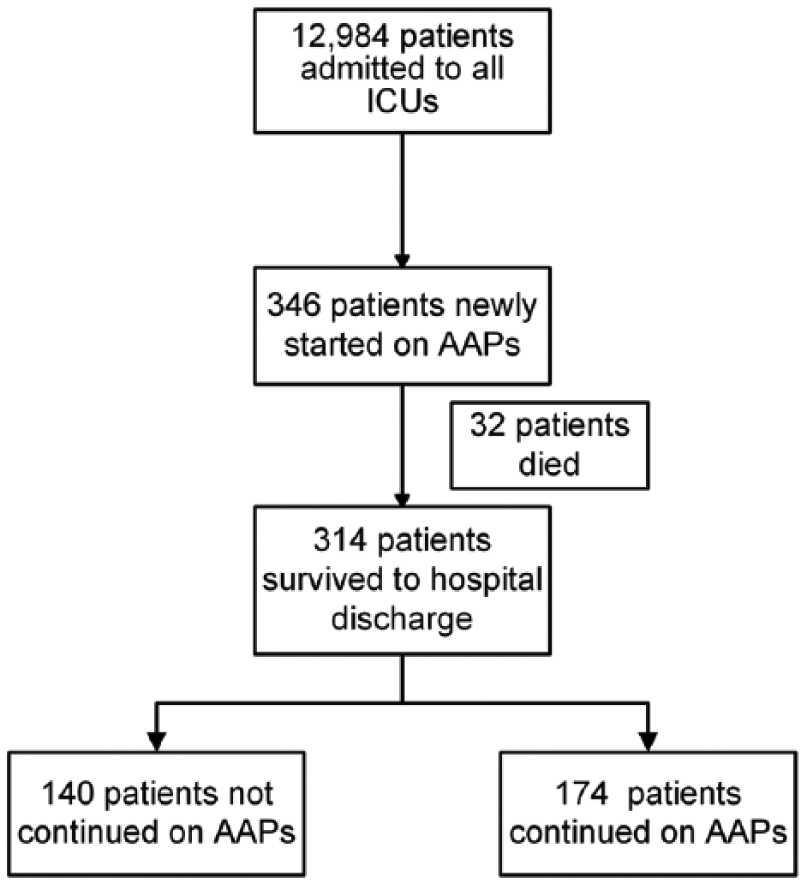
Flowchart of the study.
A total of 346 and 314 patients were analyzed for initiation and discharge-related variables, respectively. Over 66% of patients newly initiated on AAPs were male and the surgical ICU (SICU) had the most number of patients initiated on AAPs (Table 1). A total of 55% of patients remained on AAPs following hospital discharge. Quetiapine was the most commonly prescribed drug at initiation (n = 238, 69%) as well as discharge (n = 115, 66%). Physician documentation of delirium or encephalopathy was present for 102 (32.5%) patients who were newly initiated on AAPs.
Demographics of patients initiated on AAP during their ICU stay.

AAP, atypical antipsychotic; HVICU, heart and vascular intensive care unit; ICU, intensive care unit; MICU, medical intensive care unit; NCCU, neuro critical care unit; SICU, surgical intensive care unit.
Among all patients newly initiated on AAPs during their ICU stay, the comparison between patients who were continued or discontinued on AAP upon discharge is presented in Table 2. Regarding our primary predictor, we have shown that discharge location was found to be strongly associated with a higher rate of continuation of AAPs after discharge [60.3% versus 38.6%; OR = 3.11; confidence interval (CI): 1.67–3.77; p < 0.001]. Analysis of other predictors demonstrated that more men were continued on AAPs after discharge compared with women (59.7% versus 47.2%; OR = 1.69; CI: 1.03–2.77; p = 0.036) and that a shorter hospital LOS (OR = 0.68; CI: 0.51–0.92; p = 0.013) and longer ICU LOS (OR = 1.43; CI: 1.03–1.99; p = 0.031) were significantly associated with continuation of AAPs after discharge. We found no association of higher AAP continuation after discharge in patients ⩾65 years of age (p = 0.334; Figure 2). Continuation of AAPs after discharge was not significantly associated with age, initiating ICU, and AAP drug used (Table 2).
Characteristics and comparison of patients who were continued on AAP on discharge.

Mean ± SD for age, median (IQR) for hospital and ICU LOS, and N (%) for all other variables; ORs and p-values are from a multivariable logistic regression model with continued AAPs on discharge as the outcome including all factors in the table; OR for age is per 5 years while the ORs for hospital and ICU LOS is per 7 days.
AAP, atypical antipsychotic; CI, confidence interval; HVICU, heart and vascular intensive care unit; ICU, intensive care unit; IQR, interquartile range; LOS, length of stay; MICU, medical intensive care unit; NCCU, neuro critical care unit; OR, odds ratio; SD, standard deviation; SICU, surgical intensive care unit.

AAP continuation after discharge in patients ⩾65 years of age.
Discussion
In this study, we have demonstrated that continuation of AAPs is higher in patients that have been discharged to advanced care facilities (nursing home, long-term care facilities, skilled nursing facilities). In addition, we have shown that male sex is a significant risk factor for the continuation of AAPs upon discharge from hospital.
We believe that higher AAP continuation in patients discharged to advanced care facilities is important and is likely occurring because of persistent delirium, oversight or possibly the clinician’s fear of delirium relapse. 13 Due to inadequate documentation of delirium, likely common in large institutions, we were unable to determine the exact reason. The fear of relapse could certainly be of concern, since the delirium-provoking circumstances may still exist. Another reason could be that the providers are more comfortable continuing AAPs for patients discharged to healthcare facilities (compared with nonhealthcare facilities), as they will be receiving continued medical care. There are two studies that have also found similar association between discharge to a location other than home and continuation of AAPs.14,17
In our study, men were more likely to be continued on AAPs upon discharge (70.7% versus 59.3%, p = 0.034), correlating with previously published observations that ICU delirium is more common in men. 18 Previous studies have found that male patients were more likely to be newly started on antipsychotics but did not find such an association with continuation upon discharge. 17 It is unclear why this association exists in our investigation, although we argue that perceived higher rates of positive delirium symptoms (agitation, aggression, restlessness) in men may result in higher rates of initiation and continuation of AAP. We believe that further research into the sex differences of delirium are needed to better understand this relationship.
Despite no significant differences in the initiation or discharge continuation for ⩽65-year-old versus >65-year-old ICU patients, it remains worrisome that 43% of patients who were continued on AAPs after discharge were aged 65 years and older, given the increased risks in this population. It has been previously shown that there is a higher risk of initiation of AAP patients aged over 65 years and we have confirmed that this risk continues upon discharge. 17 In our study, we were unable to determine if this was an appropriate or inappropriate continuation of the AAP. Given increasing recognition of the long-term mortality risk of AAPs, this previously unpublished observation should provide impetus to improve our methodology in medicine reconciliation prior to discharge. We must ensure that the benefits of AAP continuation far outweigh the risks prior to discharge of this at-risk population.
One of the unexpected findings in our study was the association of a shorter hospital LOS with continuation of AAPs after discharge. It is possible that patients with resolution of symptoms of delirium with the use of AAP were discharged sooner and also were more likely to be continued on AAPs upon discharge.
In the four adult ICUs included in our study, 2.7% (346/12,984) of patients were started on an AAP during their ICU stay. More than 50% of the patients initiated on AAPs in the ICU had these medications continued following discharge from the hospital. This rate is consistent with current national trends as demonstrated by various studies which looked at such relationships.13,17,19 Although a higher continuation rate in surgical ICUs has been described, 19 we did not find any difference between the subspecialty ICUs in which AAPs were initiated and their continuation following hospital discharge. We did however, find a high variability in prescribing practices of AAPs among the ICUs with the initiation rate as high as 50% in the surgical ICU. The high incidence of delirium observed in postoperative patients 20 could be partly responsible for this observation. Finally, the lack of a standardized protocol for the treatment of delirium at our institution could be another reason why we observed significant differences in the prescribing practices between the ICUs.
Our retrospective analysis has limitations. This was a single-center retrospective analysis at a tertiary care academic institution, and it is not clear if the findings are generalizable across all settings. Another limitation to our study was the inability to accurately assess the indications for initiation of AAPs for all patients due to inconsistent delirium screening and physician documentation. There was significant prescriber variability in different ICUs with the heart and vascular ICU being managed exclusively by intensivists and mid-level providers while the surgical ICU, medical ICU and neuro critical care unit had a mix of house staff and mid-level providers along with intensivists. This type of variability is however, not uncommon in large academic institutions. In addition, we are unable to conclude definitively that continuation of these medications was inappropriate for all these patients, due to incomplete documentation of indications for medications at discharge.
Conclusion
In conclusion, over half of the patients initiated on AAPs in ICUs in our study were prescribed these medications at hospital discharge. We have demonstrated higher rates of AAP continuation in patients being discharged to advanced care, male patients and no difference in age >65 years compared with patients ⩽65 years. We recommend that further research in methods to reduce AAPs in patients discharged to healthcare facilities should be undertaken. We are concerned that many of these patients are discharged without adequate oversight or follow up of their symptoms of ICU delirium. Given the advent of EMRs, we believe that a discharge checklist for potentially problematic medications such as AAPs could be developed to reduce the risk of inappropriate continuation on discharge. Further research should be performed to assess the factors related to these observations to provide better management of ICU delirium, reduce post-discharge adverse events and improve post-ICU care in at-risk populations.