
Abstract
Background:
To determine the prevalence and nature of potential drug–drug interactions (DDIs) with direct oral anticoagulants (DOACs) in elderly hospitalized patients.
Methods:
This was a retrospective observational study. Inclusion criteria were: aged over 65 years; taking apixaban, rivaroxaban or dabigatran; and admitted to the Repatriation General Hospital between April 2014 and July 2015. A list of clinically relevant ‘perpetrator’ drugs was compiled from product information, the Australian Medicines Handbook, the Australian National Prescribing Service resources, and local health network guidelines. The prevalence and nature of potential DDIs with DOACs was determined by comparing inpatient drug charts with the list of perpetrator drugs.
Results:
There were 122 patients in the study with a mean age of 82 years. Most patients had nonvalvular atrial fibrillation and were taking DOACs to prevent thrombotic stroke (83%). Overall, 45 patients (37%) had a total of 54 potential DDIs. Thirty-five patients had potential pharmacodynamic DDIs with antidepressants, nonsteroidal anti-inflammatory drugs and antiplatelets (35/122, 29%). Nineteen patients had potential pharmacokinetic DDIs (19/122, 16%). Of these, 68% (13/19) were taking drugs that increase DOAC plasma concentrations (amiodarone, erythromycin, diltiazem or verapamil) and 32% (6/19) were taking drugs that decrease DOAC plasma concentrations (carbamazepine, primidone or phenytoin). There were no cases of patients taking contraindicated interacting drugs.
Discussion:
Potential DDIs with DOACs in elderly hospital inpatients are relatively common, particularly interactions that may increase the risk of bleeding. The risk–benefit ratio of DOACs in elderly patients on polypharmacy should always be carefully considered.
Keywords
Introduction
The rapid increase in direct oral anticoagulant (DOAC) use has raised concern in clinical practice about safety in patients who were not well represented in the randomized controlled trials (RCTs). In particular, the risk of bleeding in patients with chronic kidney disease, those with multiple comorbidities, the elderly, the frail, and in patients taking polypharmacy (defined as at least five concomitant drugs). 1 Polypharmacy is a well known risk factor for adverse drug reactions (ADRs) that result from drug–drug interactions (DDIs). 2 There are two major types of DDIs. Pharmacokinetic DDIs (PK-DDIs) occur when the concentration of the ‘victim’ drug is altered by the introduction of a ‘perpetrator’, altering how much and for how long the victim is present at the active site, and pharmacodynamic DDIs (PD-DDIs) occur when interacting drugs have either additive or opposing pharmacological effects. 3 Drug interactions with DOACs may arise via pharmacokinetic or pharmacodynamic mechanisms. The pharmacokinetics of DOACs is dependent to varying degrees on gastrointestinal and hepatic P-glycoprotein (P-gp) and cytochrome P4503A (CYP3A), the activities of which can be altered significantly by commonly used drugs. 4 The pharmacodynamics of DOACs can be enhanced by several drug classes, including other anticoagulants, antiplatelets, nonsteroidal anti-inflammatory drugs (NSAIDs) and the selective serotonin and selective noradrenaline reuptake inhibitors (SSRIs/SNRIs).5–7 Table 1 summarizes the important pharmacological properties of the DOACs currently available in Australia.
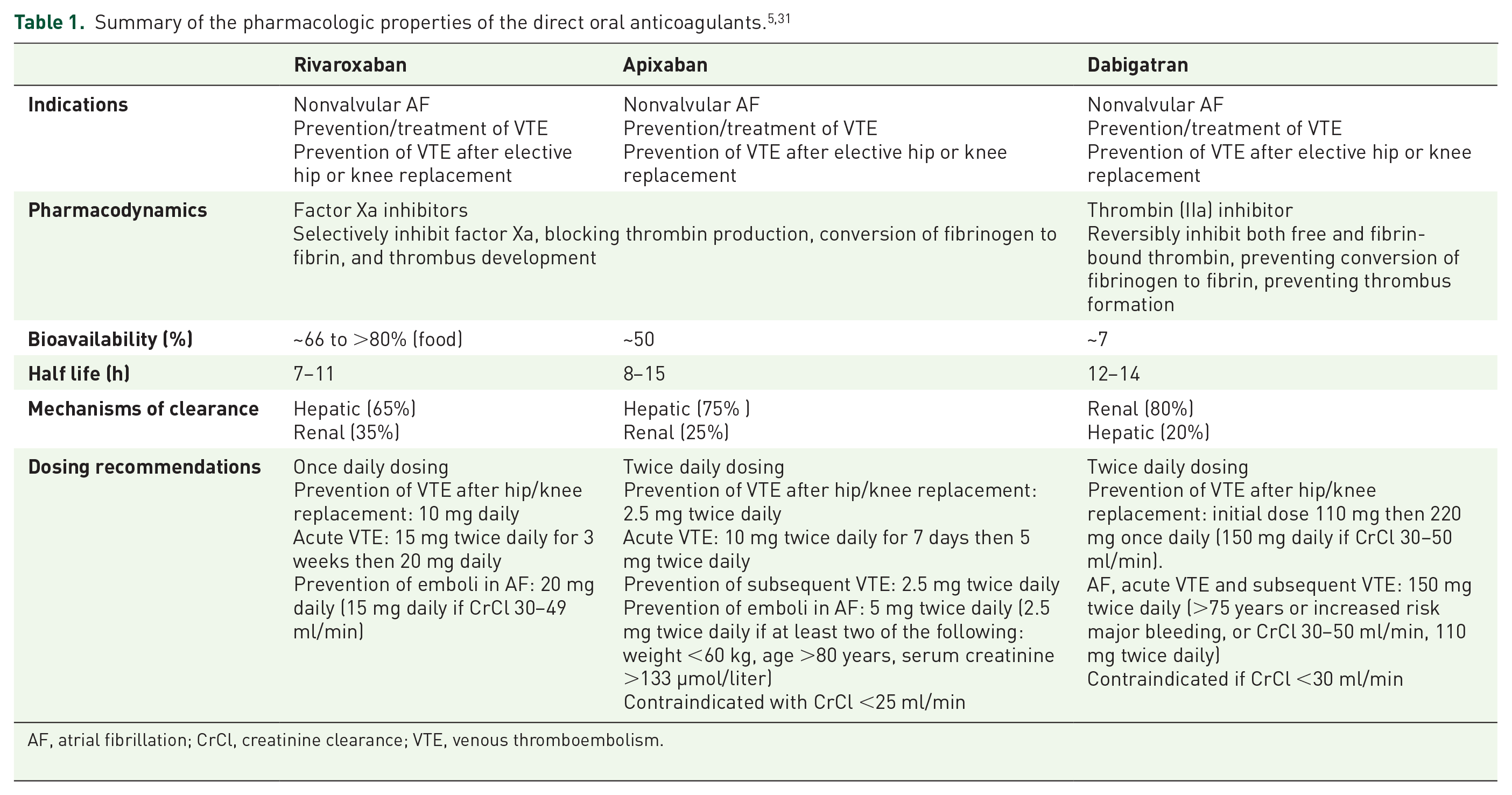
AF, atrial fibrillation; CrCl, creatinine clearance; VTE, venous thromboembolism.
Despite numerous phase I studies characterizing the changes in DOAC pharmacokinetics with P-gp or CYP3A inhibitors and inducers, as described in the product information for each drug, the clinical significance of many DDIs with DOACs is still unclear. Two post hoc analyses of RCTs with apixaban (ARISTOTLE) and rivaroxaban (ROCKET-AF) reported no significant impact of interacting drugs on bleeding risk or thrombosis, but in these analyses strong P-gp or CYP3A inhibitors and inducers were excluded, and the impact of PD-DDIs was not assessed.4,5 In contrast, other post hoc analyses of concomitant antiplatelet use in DOAC RCTs showed increased risks of major bleeding, with hazard ratios (HRs) of 1.60 [95% confidence interval (CI) 1.42–1.82] for single antiplatelet use and 2.31 (95% CI 1.79–2.98) for dual antiplatelet use in RE-LY (dabigatran), and a HR of 1.32 (95% CI 1.21–1.43) for aspirin use in ROCKET-AF (rivaroxaban).8,9 Several recent studies of DOACs in ‘real-world’ clinical settings have shown similar efficacy and safety to the RCTs, but these were not designed to investigate interacting drugs.10–15 Some data are available on clinical outcomes of specific PK-DDIs with DOACs but the evidence is conflicting. For example, amiodarone has been associated with increased odds of bleeding in patients taking rivaroxaban, 16 and patients who had major bleeds on rivaroxaban appeared twice as likely to be taking a P-gp inhibitor with or without a CYP3A inhibitor. 17 This contrasts two post hoc analyses of the ROCKET-AF and ARISTOTLE trials that found no significant difference for any bleeding outcome in patients taking rivaroxaban or apixaban with amiodarone respectively.18,19 To add to the debate over clinical relevance, there are several case reports about bleeding on DOACs following the commencement of drugs that inhibit P-gp or CYP3A, including amiodarone,20–22 and there are also case reports of decreased efficacy on CYP3A inducers such as phenytoin.23–27
A surrogate marker to identify safety concerns with DDIs in clinical practice is the reporting of ‘potential DDIs’. This is the review of medication regimens to search for theoretical DDIs, based only on knowledge of underlying mechanisms, or known DDIs, based on previously established clinical importance. After collating this literature on DOACs, between 40% and 88% of patients in various clinical settings (general medical units, orthopaedic surgery units, primary care, tertiary care etc.) have at least one potential DDI with DOACs.28–34 For example, one study showed that nearly 80% of hospitalized patients on dabigatran had potential PK-DDIs, 32 whereas another showed that concomitant use of dabigatran with P-gp inhibitors occurred in 45% of patients. 33 Likewise, in a study of rivaroxaban after major orthopaedic surgery, there was a high prevalence of potential PD-DDIs, particularly with NSAIDs (52% of patients), although concomitant use of CYP3A or P-gp inhibitors or inducers was very low (<5% of patients). 34 Despite these data, the proportion of potential DDIs that cause actual DDIs and harm to patients on DOACs is unknown.
Increasing adult age is associated with polypharmacy due to comorbidities and an increased prevalence of ADRs caused by DDIs. 35 Elderly patients may also have several DDIs considered clinically irrelevant individually but when taken together can result in serious ADRs. Given the widespread use of DOACs in the elderly, and increasing efforts to capture ‘real-world’ data about their safety, the aim of this study was to determine the prevalence and nature of potential DDIs with DOACs in hospitalized patients aged over 65 years.
Methods
This was a retrospective observational study of patient characteristics, clinical information, and drug charts in an electronic health record (the Enterprise Patient Information System, EPAS). Ethics approval was granted by the Southern Adelaide Clinical Human Research Ethics Committee (application number 324.15). All inpatients at the Repatriation General Hospital (RGH) in Adelaide who were prescribed a DOAC (apixaban, rivaroxaban or dabigatran) from April 2014 to July 2015 and were over 65 years of age were included. EPAS was searched to retrieve data on serum creatinine, height, weight, age, comorbidities and medications. Creatinine clearance was estimated using the optimized Cockcroft-Gault equation. 36 Data were collated and entered in an Excel spreadsheet.
A list of drugs with the potential to cause clinically relevant DDIs with DOACs in Australia was compiled from various prescribing information resources (Table 2). The resources used were the Australian product information for each DOAC from the manufacturer;6,7,37 the Australian Medicines Handbook, which is the national drug formulary of Australia updated annually; 38 the National Prescribing Service online resources, an Australian Government funded organization that provides evidence-based information to healthcare professionals and consumers; 39 and the South Australian health guidelines on DAOC use, which were compiled by a senior clinical pharmacist in collaboration with medical consultants from relevant clinical units. Commercial DDI compendia were searched to check for any missed interacting drugs, but, because of the disparity between these compendia, 40 they were not used as primary resources to generate the list. Drugs that cause at least fivefold increase in DOAC area under the plasma concentration–time curves (AUCs) are typically strong inhibitors of P-gp or CYP3A, and these drugs are all contraindicated interacting medications. Drugs that cause at least twofold but up to fivefold increases in DOAC AUC are typically moderate inhibitors of P-gp or CYP3A. Many of these drugs are not contraindicated, but prescribing advice is to use with caution. Drugs that are inducers of P-gp or CYP3A have highly variable effects on drug exposure due to time dependence and differences in study designs used for characterization, and no work has yet catalogued inducers according to changes in DAOC AUC. Interestingly, drug information resources are inconsistent with prescribing advice for DOACs in the presence of these inducers, with some resources stating that inducers are contraindicated, 38 whereas others advise caution with an assessment of overall thrombotic risk. 39 Medications that interact with DOACs through pharmacodynamic mechanisms are also considered to be used with caution, the exception being other anticoagulants which are contraindicated. When considering drug classes [e.g. human immunodeficiency virus (HIV) protease inhibitors, NSAIDs, SSRIs/SNRIs, anticoagulants, antiplatelets and proton pump inhibitors (PPIs)], all drugs in the class were considered equal as potential perpetrators of DDIs with DOACs.
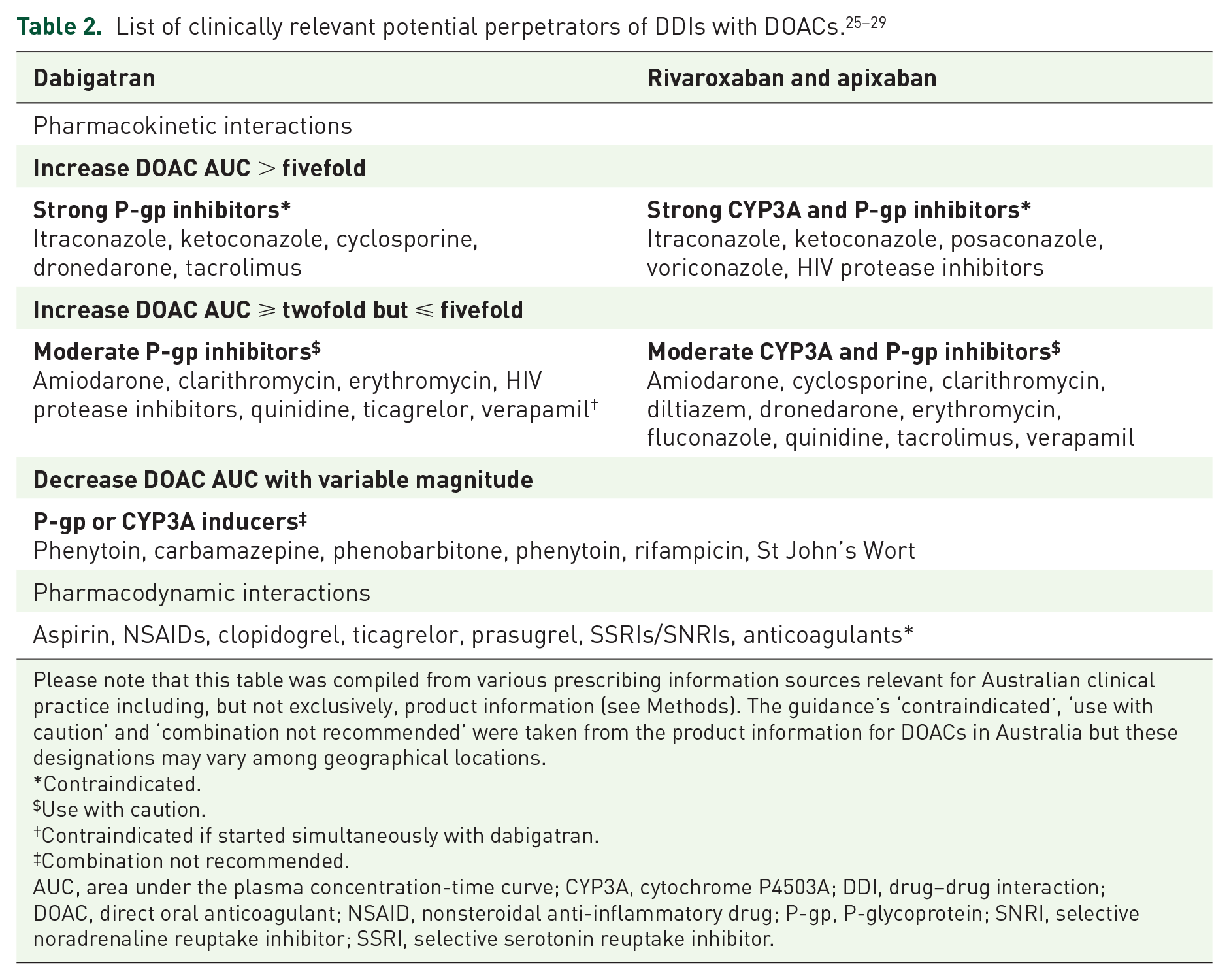
Please note that this table was compiled from various prescribing information sources relevant for Australian clinical practice including, but not exclusively, product information (see Methods). The guidance’s ‘contraindicated’, ‘use with caution’ and ‘combination not recommended’ were taken from the product information for DOACs in Australia but these designations may vary among geographical locations.
Contraindicated.
Use with caution.
Contraindicated if started simultaneously with dabigatran.
Combination not recommended.
AUC, area under the plasma concentration-time curve; CYP3A, cytochrome P4503A; DDI, drug–drug interaction; DOAC, direct oral anticoagulant; NSAID, nonsteroidal anti-inflammatory drug; P-gp, P-glycoprotein; SNRI, selective noradrenaline reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
Drugs that were prescribed, dispensed and administered during the hospital admissions of patients taking DOACs were included in the analysis, except for stat (one-off) doses. Thus, potential interacting drugs had to be administered to patients on multiple occasions. These drugs were cross checked with the drugs in Table 2 to identify potential DDIs with DOACs and then categorized by the type and mechanism of the interaction. To compare the prevalence of potential DDIs with previous studies, two separate overall analyses were conducted, one including PPIs (omeprazole, esomeprazole, pantoprazole, lansoprazole and rabeprazole) and one excluding PPIs (i.e. only the drugs listed in Table 2). The rationale for this is that PPIs were previously considered as perpetrators of PK-DDIs with dabigatran. 5 Data were analysed by simple statistics and expressed as percentages.
Results
Twenty-five individual drugs and five drug classes (HIV protease inhibitors, NSAIDs, SSRIs/SNRIs, antiplatelets and anticoagulants) were identified as potential perpetrators of DDIs with DOACs that are relevant for Australian clinical practice. Table 2 shows the list of interacting drugs, DDI type and mechanism, and the estimated changes in DAOC exposure for PK-DDIs.
The characteristics of patients in the study are summarized in Table 3. There were 122 patients with a mean age of 82 years (48.4% men and 51.6% women). Forty-nine (40%) patients were taking rivaroxaban, 50 (41%) were taking apixaban and 23 (19%) were taking dabigatran. Most patients had nonvalvular atrial fibrillation and were on DOACs to prevent thrombotic stroke (83%). The mean creatinine clearance was 44 ml/min and the mean CHADSVasc score was 4.83, which translates to a thrombotic stroke risk of 5–6% per year.
Patient characteristics.
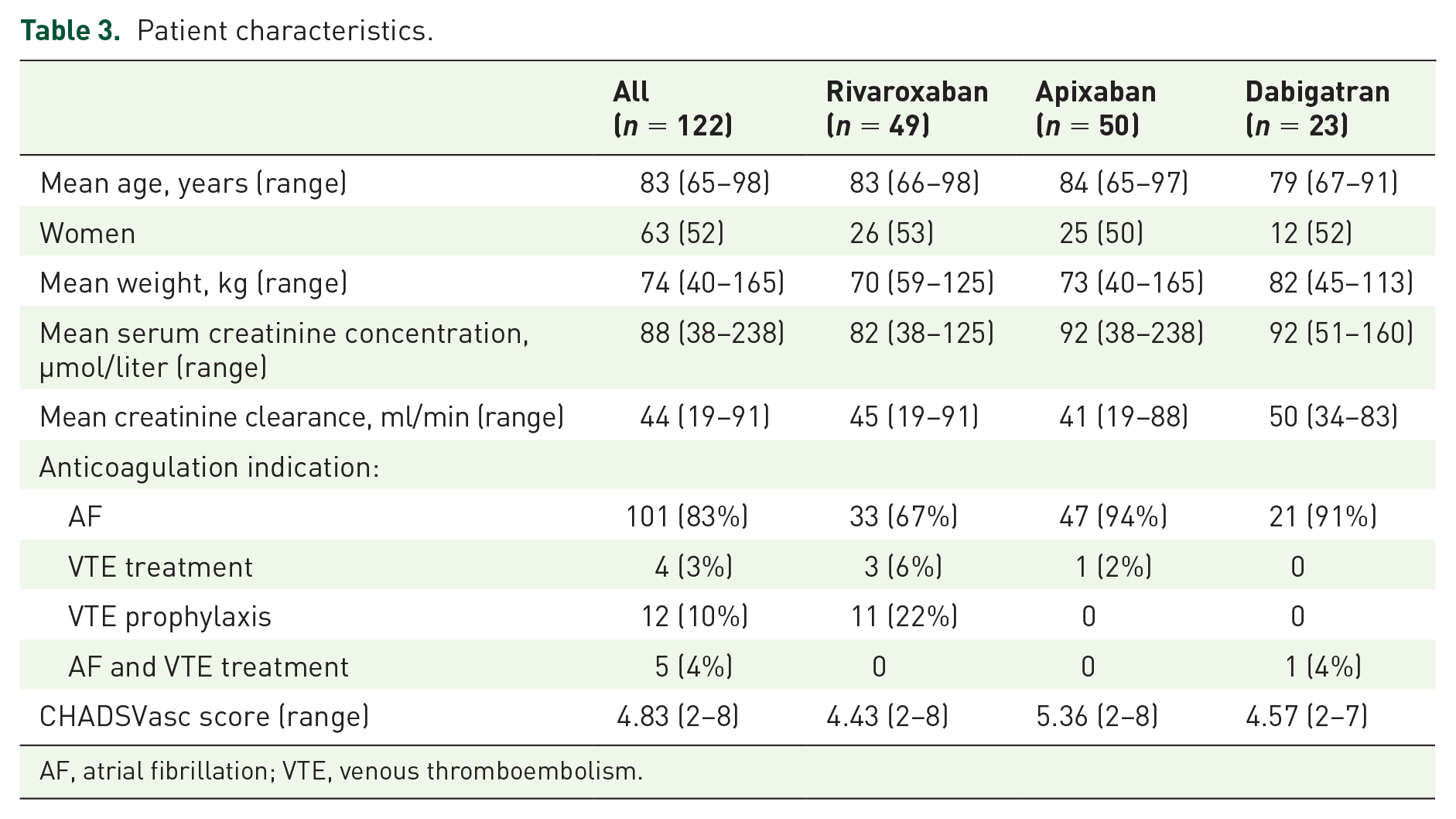
AF, atrial fibrillation; VTE, venous thromboembolism.
Overall, 45 patients (37%) had a total of 54 potential interactions. Thirty-five of the 122 patients had potential PD-DDIs (29%) and 19 patients had potential PK-DDIs (16%). Of the patients who had potential pharmacodynamic interactions, 80% (28/35) were taking SSRIs/SNRIs (desvenlafaxine, paroxetine, sertraline, citalopram, venlafaxine, escitalopram, duloxetine or fluoxetine), 8.6% (3/35) were taking NSAIDs (ibuprofen or meloxicam) and 11% (4/35) were taking aspirin [Figure 1(a)]. Of the patients who had potential pharmacokinetic interactions, 68% (13/19) were taking medications that increase DOAC plasma concentrations (amiodarone, erythromycin, diltiazem or verapamil) and 32% (6/19) were taking medications that decrease DOAC plasma concentrations (carbamazepine, primidone or phenytoin) [Figure 1(b)]. There were no cases of patients taking contraindicated interacting drugs. The rank order of prevalence of potential DDIs was rivaroxaban (88%) > dabigatran (52%) > apixaban 30%. When PPIs were included in the analysis, 18 patients had potential interactions with dabigatran (18/23, 78% of patients on dabigatran), to give an overall prevalence of patients with potential DDIs with DOACs of 42%.
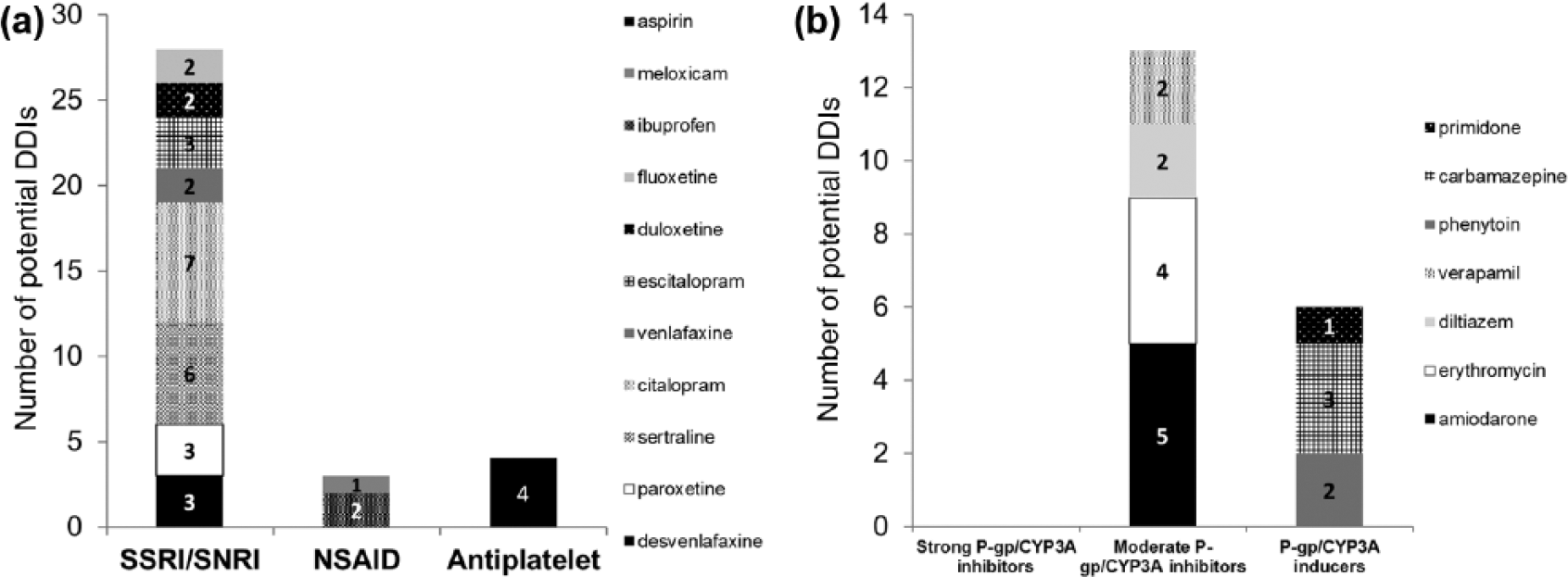
Potential pharmacodynamic drug–drug interactions (DDIs) (a) and pharmacokinetic DDIs (b) with direct oral anticoagulants (DOACs). CYP3A, cytochrome P4503A; NSAID, nonsteroidal anti-inflammatory drug; P-gp, P-glycoprotein; SNRI, selective noradrenaline reuptake inhibitor; SSRI, selective serotonin reuptake inhibitor.
There were eight patients in the study who had more than one potential interaction with a DOAC (6.6%). Four of these patients had the combination of a PD-DDI and a PK-DDI with an inhibitor of P-gp or CYP3A. One patient was taking rivaroxaban with ibuprofen (NSAID) and citalopram (SSRI), one was taking apixaban with amiodarone (P-gp/CYP3A inhibitor) and phenytoin (P-gp/CYP3A inducer) and two patients had combinations of potential PD-DDIs and PK-DDIs, with apixaban–duloxetine (SNRI) and carbamazepine (P-gp/CYP3A inducer) in one, and ibuprofen and phenytoin in the other.
Discussion
This is the first study to investigate potential DDIs with DOACs exclusively in elderly hospitalized patients. The mean age was high (>82 years) and well above the exclusion cutoff of 65 years. Thirty-seven percent of patients had potential interactions, which is just below the lower limit of the range collated from other studies with DOACs in clinical settings (40–88%).28–34 Twice as many patients had potential PD-DDIs with DOACs compared with PK-DDIs, driven predominantly by concomitant use of SSRIs/SNRIs [Figure 1(a, b)].
The lower prevalence of patients with potential DDIs with DOACs in our study compared with previous work could be for several reasons. First, prescribers may be becoming more familiar with DOAC interactions as clinical experience with their use increases. Second, there may be heightened awareness of DDIs in the study population, the elderly, who are well known to have increased susceptibility to ADRs. Third, apixaban, rivaroxaban and dabigatran were studied here, whereas most of the comparator studies included only dabigatran.28–34 The prevalence difference could be explained because PPIs were classified as interacting drugs in several of the previous dabigatran studies, in which up to 64% of patients were taking dabigatran and PPIs together. 32 The rationale for this classification is that the bioavailability of dabigatran is dependent on an acidic gastric environment, and pantoprazole decreased dabigatran absorption by 30% in a phase I healthy volunteer study and by an average of 12.5% in RE-LY. 7 We also found very high concurrent use of dabigatran and PPIs (78% of patients). Indeed, when PPIs were included as perpetrators, this increased the overall prevalence of patients with potential interactions to 42%, consistent with the range of previous work (40–88%).28–34 However, the consensus now is that interactions between dabigatran and PPIs are not clinically important. 5 Therefore, PPIs were excluded from the list of clinically relevant perpetrators (Table 2) and the final prevalence calculations. Fourth, other variations in perpetrator lists could result in prevalence differences, a known problem when comparing commercial DDI compendia. 40 Fifth, the clinical setting and the types of cases can influence DDI risk. For example, acute medical units have a high patient turnover and wide patient demographic, and studies there would capture more patients taking contraindicated interacting drugs such as azole antifungals and HIV protease inhibitors. Finally, the availability of clinical pharmacology or clinical pharmacy support could also influence the likelihood of interacting drugs being coprescribed. This study was conducted at the RGH where clinical pharmacists attend all ward rounds and for each patient determine the medication history and conduct a full medication review.
There were fewer patients in the study with potential PK-DDIs compared with potential PD-DDIs, 16% versus 29% respectively. This was also reported in patients taking rivaroxaban after major orthopaedic surgery, when NSAIDs were coprescribed in 54% but the prevalence of potential PK-DDIs was only 4.6%. 34 Other studies have shown similar frequencies of PD-DDIs, particularly due to coprescription of aspirin (47–60%).30,33,41 The comparably low prevalence of PD-DDIs in our study (29%) was largely due to minimal antiplatelet use (3.3%), possibly because prescribers were reluctant to use an antiplatelet and anticoagulant combination in elderly inpatients. Interestingly, potential interactions between DOACs and SSRIs/SNRIs were common, occurring in about a quarter of inpatients (28/122). Many prescribers may not be aware of the bleeding risks of SSRIs/SNRIs, especially when used in combination with antiplatelets or anticoagulants.42–45 One cohort study found that in patients with atrial fibrillation taking warfarin, bleeding rates were higher during periods of SSRI use compared with periods when they were not taken (2.32 per 100 person-years versus 1.35 per 100 person-years, p ⩽ 0.001). 44 There are also some data about the risks of bleeding with coadministration of DOACs and SSRI/SNRIs. An analysis of the RE-LY trial showed an increased risk of bleeding when SSRIs were used in combination with dabigatran, but detail about the magnitude of this risk has not been published. 7 The product information for apixaban suggests using the combination of apixaban and SSRIs/SNRIs with caution, presumably based on first principles since a reference to primary literature is not given. 6 Taken together, these data represent relatively weak clinical evidence to support the SSRI/SNRI-DOAC interactions and further work is required to address the question of clinical significance in sufficient detail. Therefore, it is important to note that the high prevalence of DOAC and SSRI/SNRI combinations reported here in the elderly (28/122) represents potential rather than actual DDIs, and that withholding therapies based on this finding alone may be inappropriate.
No patients in the study took contraindicated interacting medications with DOACs. This is pleasing considering that Candel and colleagues 28 and Trujillano and colleagues 31 found 8.6% and 8.2% of patients in their respective studies took contraindicated drugs. Importantly, there were eight patients in the study who had greater than one potential DDI. How such interactions play out in clinical practice is complex and difficult to predict. The most concerning drug combinations give an increased risk of bleeding: concurrent PD-DDI and PK-DDI involving a P-gp or CYP3A inhibitor, since increases in DAOC concentration could augment already enhanced pharmacodynamics (this occurred in four patients); and concurrent use of multiple drugs with additive pharmacodynamic properties, for example one patient was on rivaroxaban, ibuprofen and citalopram.
This study was not designed to measure clinical events. It is therefore not possible to determine the proportion of potential DDIs with DOACs that subsequently contributed to any patient harm. This is a universal limitation of studies reporting potential DDIs. However, an important attribute of this work is the quick and cheap identification of prescribing patterns that could negatively impact drug safety. Indeed, our results were used to educate local prescribers, highlighting the high mean age of patients taking DOACs at the hospital and the frequently seen DOAC and SSRI/SNRI combinations.
In conclusion, potential DDIs with DOACs in elderly hospitalized patients are relatively common, occurring in about one third of patients. Most of these potential interactions may increase the risk of bleeding, either by additive pharmacological effects, by increasing DOAC exposure, or by a combination of both. The risk–benefit ratio of DOACs in elderly patients on polypharmacy should always be carefully considered.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.