
Abstract
Dear Editor
We previously published a study that examined the risk of Mirena with benign intracranial hypertension (BIH). 1 As part of the analysis we used the United States Food and Drug Administration’s (US FDA) Adverse Events Reporting System (FAERS) database using a disproportionality analysis (DA). 2 DA is a signal detection technique that is used in drug safety research to examine safety signals using adverse drug reaction databases such as FAERS. This technique examines the rate of an adverse event with the drug of interest and compares it with the same event reported with all other drugs. In our previous analysis using the raw US FDA data we computed a reported odds ratio (ROR) of 1.50 [95% confidence interval (CI): 1.10–2.05] 1 for the outcome of BIH. In a separate analysis, 3 I reported an ROR of 3.4 (95% CI: 2.59–4.45) using Open Vigil (2.1), a validated online program that computes effect sizes for DA and provided more recent FAERS data. 2
Neither analyses controlled for reproductive age which has a strong correlation with BIH. 4 Due to this strong correlation an analysis that does not compare the risk of BIH with Mirena to women in the same age group may lead to effect modification. This means that an unstratified analysis by reproductive age can artificially overestimate the risk of BIH with Mirena. Here I demonstrate how this can occur. Using OpenVigil (2.1) I entered the term ‘Mirena’ and ‘BIH’ as the outcome of the interest. The analysis was restricted to unique cases. A total of two analyses were conducted: one without restriction to age and one restricted to women of reproductive age (15–40 years). The results are presented in Table 1. ROR and proportional reporting ratio (PRR) generated by OpenVigil were 3.76 (2.73–5.18) and 3.7 (2.72–5.18), respectively for the age unrestricted analysis. The ROR and PRR are virtually the same due to the rarity of the events.
DA of Mirena and BIH with and without age restriction.
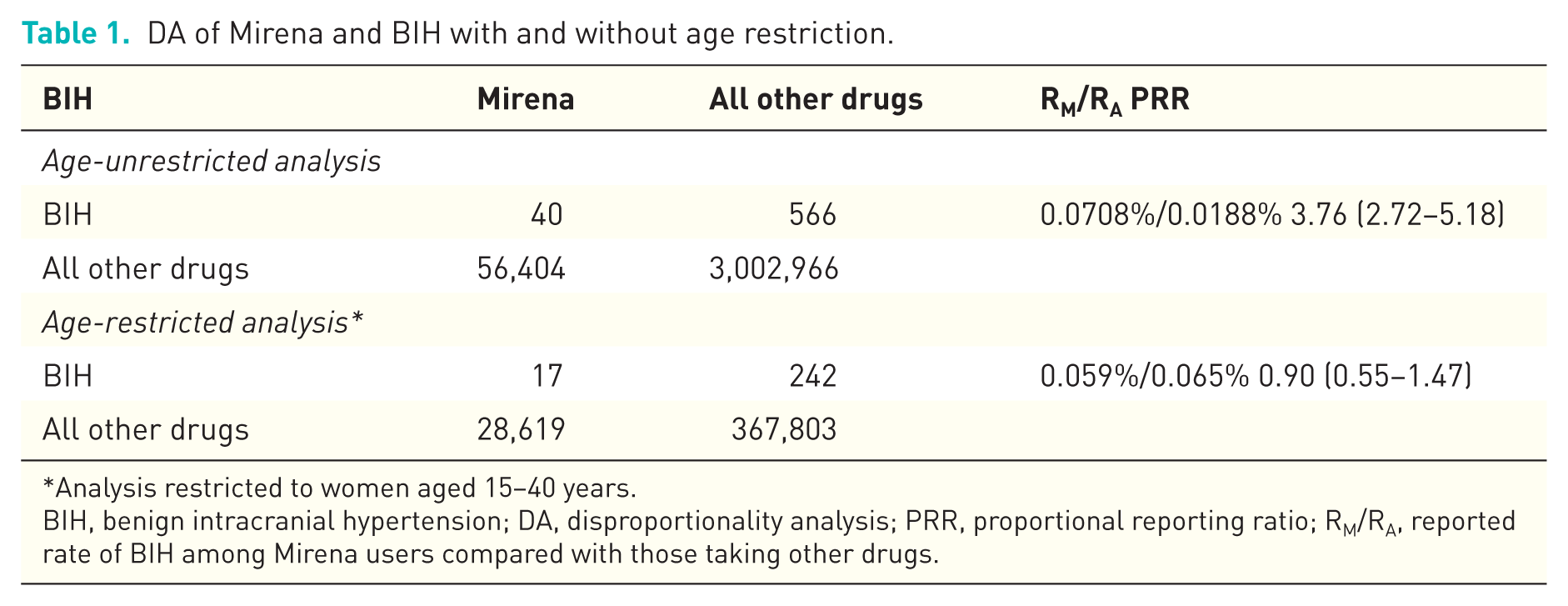
Analysis restricted to women aged 15–40 years.
BIH, benign intracranial hypertension; DA, disproportionality analysis; PRR, proportional reporting ratio; RM/RA, reported rate of BIH among Mirena users compared with those taking other drugs.
Since PRR is a simpler parameter to conceptualize, I only present the PRRs in Table 1. There is a drop in the magnitude of PRR in the age-restricted analysis with a PRR of 0.90 (0.55–1.47) (Table 1). This change may be explained in two ways when computing the PRR (RM/RA, rate in Mirena users compared with the rate in users of all other drugs). First, a smaller number of BIH cases in the age-restricted analysis (a drop in the cases from 40 to 17) which demonstrates possible use of Mirena in older women for conditions other than birth control 5 such as dysmenorrhea or endometriosis. Second, the age-restricted analysis results in a larger rate in the denominator (0.0188% in the age-unrestricted analysis versus 0.065% in the age-restricted analysis). The denominator in the age-restricted analysis represents the reported rate of BIH in women aged 15–40 years not on Mirena. Since this rate is higher than the rate in the age-unrestricted analysis, the excess risk might represent the rate of BIH in women aged 15–40 years in the FAERS database.
Based on the age-restricted analysis a signal is not detected with Mirena with respect to BIH when child bearing age is accounted for. Although in general disproportionality analyses are not restricted by age for many drug safety questions (use of antihypertensive medications or statins mainly uses by older adults) restriction to the appropriate age range where age might be a strong confounder or effect modifier might produce a more unbiased estimate of the signal.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
Etminan has been an expert witness in Mirena litigation in the past but is no longer part of the litigation.