
Abstract
Objectives:
The objective of our study was to describe spontaneously reported haemorrhagic adverse events associated with rivaroxaban and dabigatran in Australia.
Methods:
Data were sourced from the Australian Therapeutic Goods Administration (TGA) Database of Adverse Event Notifications between June 2009 and May 2014. Records of haemorrhagic adverse events in which rivaroxaban or dabigatran was considered as a potential cause were analysed.
Results:
There were 240 haemorrhagic adverse events associated with rivaroxaban and 504 associated with dabigatran. Age was specified for 164 (68%) haemorrhages associated with rivaroxaban, of which 101 occurred in people aged ⩾75 years. Age was specified for 437 (87%) haemorrhages associated with dabigatran, of which 300 occurred in people aged ⩾75 years. Time from treatment initiation to haemorrhage was specified for 122 (51%) haemorrhages associated with rivaroxaban, with 69 (57%) haemorrhages occurring within 30 days of rivaroxaban initiation. Time from treatment initiation to haemorrhage was specified for 253 (50%) haemorrhages associated with dabigatran, with 123 (49%) haemorrhages occurring within 30 days of dabigatran initiation. Gastrointestinal (GI) haemorrhages were the most frequent type of haemorrhages associated with both rivaroxaban (n = 105, 44%) and dabigatran (n = 302, 60%). Data were available on the severity of haemorrhage for 101 (42%) haemorrhages associated with rivaroxaban, with haemorrhage leading to death in 17 people. The severity of haemorrhage was specified for 384 (76%) haemorrhages associated with dabigatran, with haemorrhage leading to death in 61 people.
Conclusions:
Our study highlights the need for research on the haemorrhagic complications of anticoagulation in clinical care. A considerable proportion of reported haemorrhagic events occurred within 30 days of rivaroxaban and dabigatran initiation. This highlights the importance of considering bleeding risk at the time of treatment initiation.
Keywords
Introduction
Non-vitamin K oral anticoagulants (NOACs) rivaroxaban and dabigatran are new alternatives to warfarin for the prevention and treatment of venous thromboembolism (VTE), and stroke prevention in non-valvular atrial fibrillation (AF). Rivaroxaban and dabigatran are approved in Australia for patients undergoing elective hip or knee replacement and in patients with AF with at least one additional risk factor for stroke [Australian Government Department of Health 2013]. NOACs have several potential advantages over warfarin including less drug–food and drug–drug interactions [Savelieva et al. 2014]. NOACs have a more predictable dose response than warfarin and standard dosing is possible for patients without drug–drug interactions or renal impairment. This means that regular monitoring of coagulation parameters is generally not performed [Schulman 2014]. These may be contributing factors to the increasing uptake of NOACs. There were 406,640 rivaroxaban- and 173,883 dabigatran-reimbursed prescriptions dispensed in Australia between July 2013 to June 2014 [Australian Government Department of Health: Pharmaceutical Policy Branch 2014].
Australian data on the safety of NOACs are sparse. A study of 244 spontaneous adverse drug-event reports associated with rivaroxaban up until March 2013 found that 30% of reports related to haemorrhage [McDonald et al. 2014]. A corresponding study of 1039 reports associated with dabigatran found 35% of reports related to haemorrhage [McDonald et al. 2015]. Neither study reported how many haemorrhages were fatal. Medical professionals in Australia have called for more local data on NOACs [Pharma in Focus 2014]. The objective of our study was to describe spontaneously reported haemorrhagic adverse events associated with rivaroxaban and dabigatran in Australia.
Methods
Data source
Data were sourced from the Australian Therapeutic Goods Administration (TGA) Database of Adverse Event Notifications (DAEN) between June 2009 and May 2014 [Australian Government Department of Heath: Therapeutic Goods Administration 2013]. Pharmaceutical companies are mandated to report adverse events, while health professionals and consumers are encouraged by recommendation only to report adverse events. The DAEN contains over 260,000 spontaneously reported adverse events since 1971. Adverse events are indexed in DAEN using Medical Dictionary for Regulatory Activities (MedDRA) reaction terms assigned by TGA medical officers. The Monash University Human Research Ethics Committee deemed the study to be exempt from needing ethics approval.
Definition of the cases
The public case report for each haemorrhagic adverse event in which rivaroxaban or dabigatran was considered a potential cause was obtained. Information on each patient’s age, sex, dose, indication, time from treatment initiation to onset of event, and predisposing clinical factors were extracted. Reports were excluded if the report included contradictory data or if the report was a duplicate.
Analysis
The duration of NOAC use prior to the haemorrhagic event was categorised as up to 1 day, 2–6 days, 7–30 days and more than 30 days. MedDRA reaction terms were grouped according to the system organ class. Data were presented as frequencies and proportions. Characteristics of cases were reported separately for those aged <75 years and those aged ⩾75 years. This cut–off was based on the ROCKET–AF trial where the safety and efficacy of rivaroxaban was reported separately for those aged <75 years and those aged ⩾75 years [Halperin et al. 2014]. Haemorrhages in the RE–LY trial of dabigatran in AF have also been reported separately for people aged <75 years and aged ⩾75 years [Clemens et al. 2014]. All analyses were performed using SAS 9.4 (SAS Institute, Cary, NC).
Results
There were 240 haemorrhages associated with rivaroxaban reported to the TGA between June 2009 and May 2014. Haemorrhages were reported by pharmaceutical companies (72%, n = 172), hospitals (13%, n = 30), pharmacists (8%, n = 20), general practitioners (6%, n = 14) and members of the public (1%, n = 3). There were 504 haemorrhages associated with dabigatran. Reporting was by pharmaceutical companies (72%, n = 361), hospitals (12%, n = 61), pharmacists (8%, n = 40), general practitioners (7%, n = 32), members of the public (1%, n = 6) and specialist physicians (<1%, n = 3).
Age was specified for 164 (68%) haemorrhages associated with rivaroxaban, of which 101 occurred in people aged ⩾75 years (Table 1). Age was specified for 437 (87%) haemorrhages associated with dabigatran, of which 300 haemorrhages occurred in people aged ⩾75 years (Table 2). Indication was specified for 144 (60%) haemorrhages associated with rivaroxaban, with AF being reported as the indication in 102 events (45 events among those aged ⩾75 years, 29 events among those aged <75 years, and for 28 events the age was not specified) and VTE prevention or treatment (including hip or knee arthroplasty) in 38 events (14 events among those aged ⩾75 years, 15 events among those aged <75 years, and for 9 events the age was not specified). Indication was specified for 222 (44%) haemorrhages associated with dabigatran, with AF being reported as the indication for 209 events (61 events among those aged <75 years, 134 events among those aged ⩾75 years, and for 14 events age was not specified).
Characteristics of reports of rivaroxaban-associated haemorrhage by age.
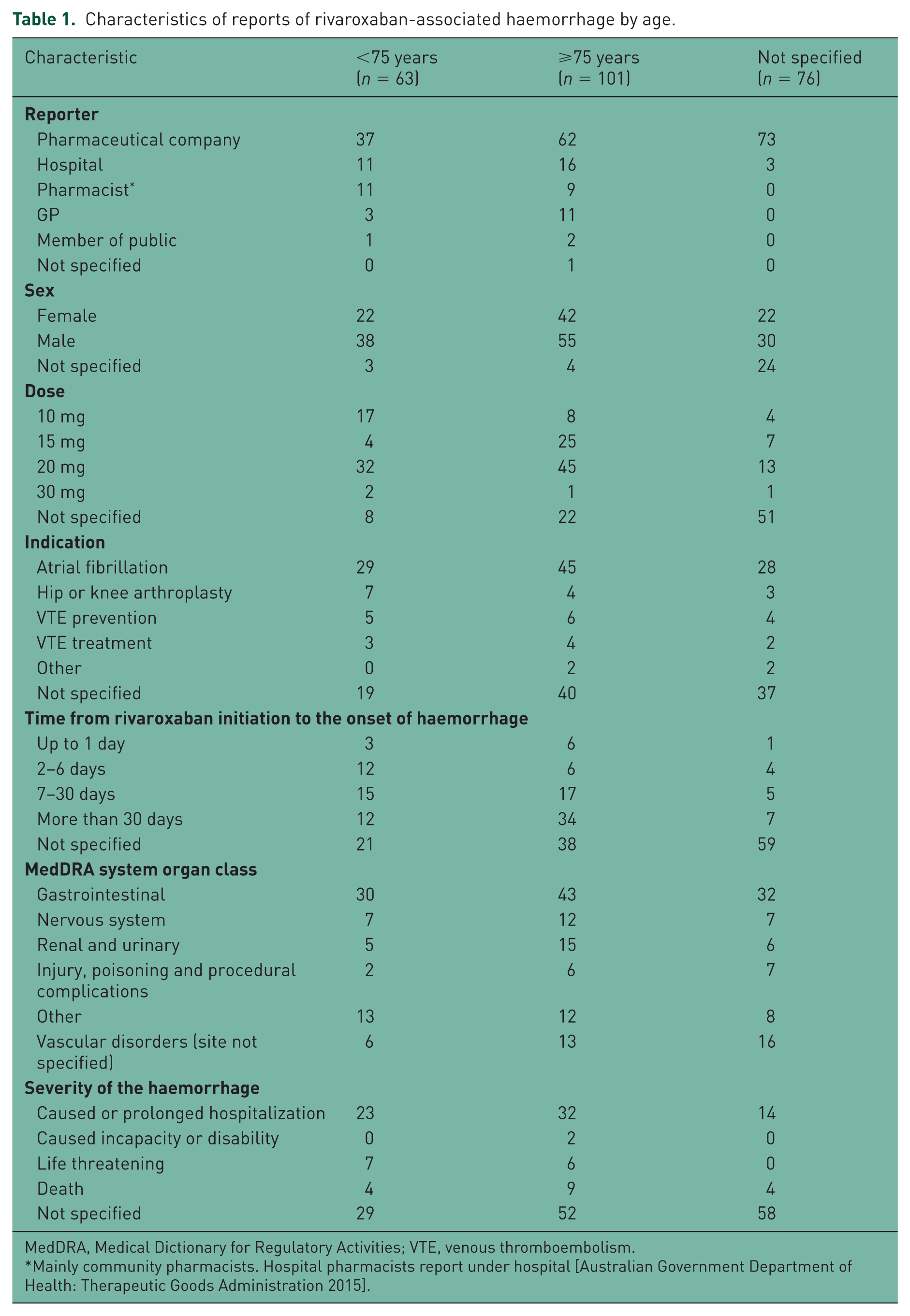
MedDRA, Medical Dictionary for Regulatory Activities; VTE, venous thromboembolism.
Mainly community pharmacists. Hospital pharmacists report under hospital [Australian Government Department of Health: Therapeutic Goods Administration 2015].
Characteristics of reports of dabigatran-associated haemorrhage by age.
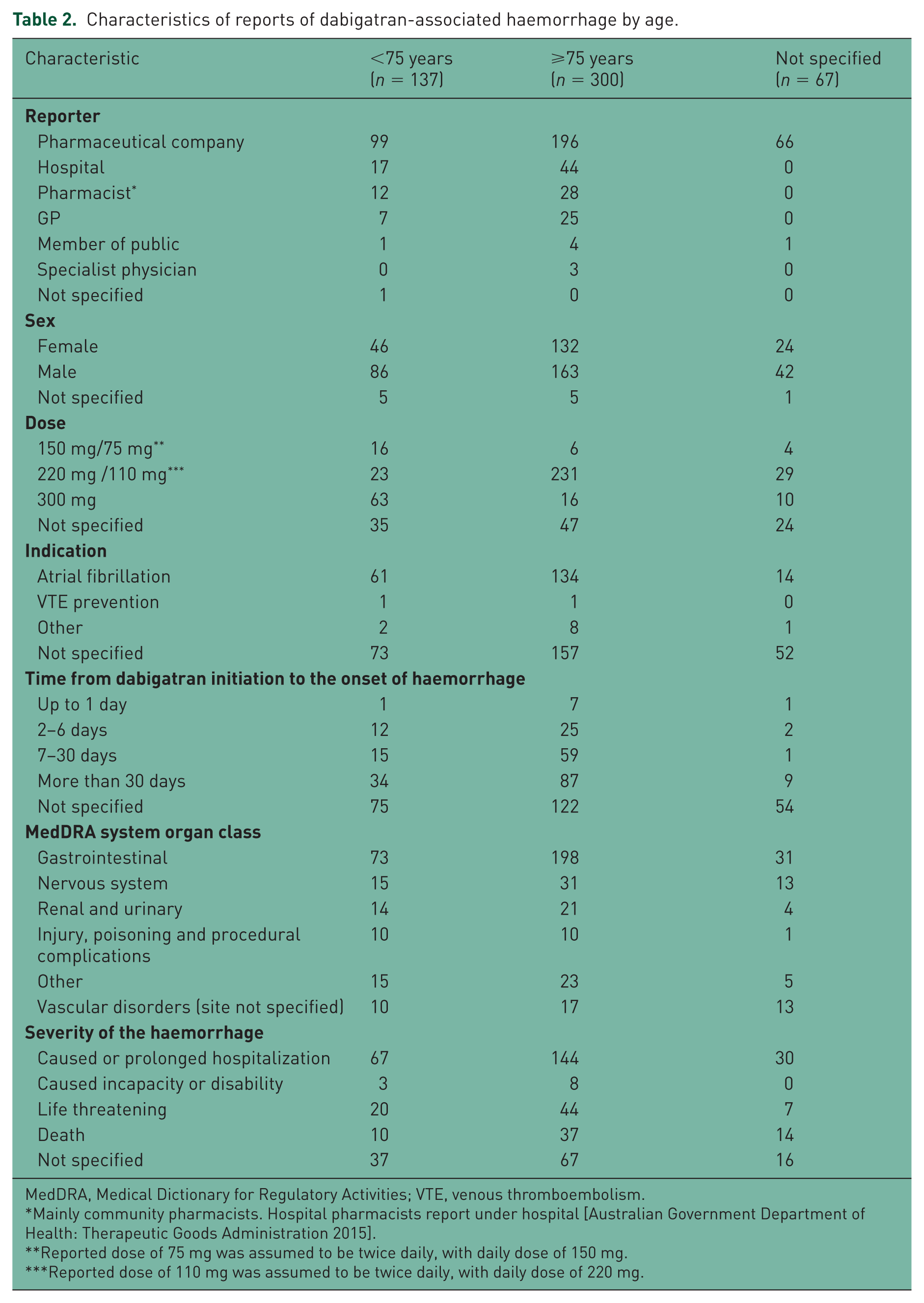
MedDRA, Medical Dictionary for Regulatory Activities; VTE, venous thromboembolism.
Mainly community pharmacists. Hospital pharmacists report under hospital [Australian Government Department of Health: Therapeutic Goods Administration 2015].
Reported dose of 75 mg was assumed to be twice daily, with daily dose of 150 mg.
Reported dose of 110 mg was assumed to be twice daily, with daily dose of 220 mg.
Time from treatment initiation to haemorrhage was specified for 122 (51%) haemorrhages associated with rivaroxaban, with 69 (57%) haemorrhages occurring within 30 days of rivaroxaban initiation (29 events in people aged ⩾75 years, 30 events in people aged <75 years, and for 10 events the age was not specified). Time from treatment initiation to haemorrhage was specified for 253 (50%) haemorrhages associated with dabigatran, with 123 (49%) haemorrhages occurring within 30 days of dabigatran initiation (91 events in people aged ⩾75 years, 28 events in people aged <75 years, and for 4 events the age was not specified).
Gastrointestinal (GI) haemorrhages were the most frequent type of haemorrhage associated with rivaroxaban (n = 105, 44%). Of these, 43 GI haemorrhages occurred in people aged ⩾75 years, 30 in people aged <75 years, and for 32 the age was not specified. GI haemorrhages were also the most frequent type associated with dabigatran (n = 302, 60%). Of these, 198 GI haemorrhages occurred in people aged ⩾75 years, 73 in people aged <75 years, and for 31 the age was not specified.
Data were available on the severity of haemorrhage for 101 (42%) haemorrhages associated with rivaroxaban, with haemorrhage leading to death in 17 people (9 people aged ⩾75 years, 4 people aged <75 years, and for 4 people the age was not specified). The severity of haemorrhage was specified for 384 (76%) haemorrhages associated with dabigatran, with haemorrhage leading to death in 61 people (37 people aged ⩾75 years, 10 people aged <75 years, and for 14 people the age was not specified).
Discussion
The main finding of our study was that there were 240 rivaroxaban haemorrhagic adverse events and 504 dabigatran haemorrhagic adverse events reported to the Australia TGA up until May 2014. A total of 17 of the rivaroxaban-related haemorrhages and 61 of the dabigatran-related haemorrhages were fatal. Our study provided an additional 14 months of adverse event data than the two previous studies published by McDonald and colleagues [McDonald et al. 2014, 2015]. Our study included 240 rivaroxaban-related haemorrhages and 504 dabigatran-related haemorrhages compared with 75 and 367, rivaroxaban and dabigatran haemorrhages, respectively, in the earlier two studies [McDonald et al. 2014, 2015].
Consistent with previous literature we found that GI haemorrhage was the most prevalent type of haemorrhagic event reported for both rivaroxaban and dabigatran. In the ROCKET–AF trial GI haemorrhages were the most frequently reported major haemorrhages in the rivaroxaban arm [Patel et al. 2011]. Similarly, GI haemorrhages were the most frequently reported major haemorrhages reported in the RE–LY trial of dabigatran [Connolly et al. 2009] and in observational studies of dabigatran and rivaroxaban [Beyer–Westendorf et al. 2015, Tamayo et al. 2015]. A meta-analysis of risk for GI bleeding found that NOACs are associated with a modest but significant increase in risk of GI bleeds compared to previous standards of care including low-molecular-weight-heparins, warfarin, or antiplatelets [Holster et al. 2013]. GI bleeding is a particular concern among older people because the 30-day mortality rate associated with GI bleeds increases with age by up to 10% among people aged 75–84 years [Wilcox et al. 2009].
For rivaroxaban, 17 out of 101 haemorrhages for which severity data were available were fatal. This is a higher fatality rate than in the ROCKET–AF trial in which 7% of all major bleeds were fatal [Patel et al. 2011]. However, severity was not reported for 139 haemorrhagic events. It is possible that the severity was less likely to be recorded for less severe haemorrhages and that less severe haemorrhages were less likely to be reported than severe haemorrhages. Assuming that severity was recorded for all fatal haemorrhages, then the rivaroxaban-haemorrhage fatality rate in our study was comparable to the fatality rate in the ROCKET–AF trial. While 61 dabigatran-related haemorrhages were fatal, severity data were only recorded for 384 of 504 reports in our study. In the RE–LY trial 51 of 741 (7%) major bleeds were fatal [Eikelboom et al. 2011].
We found that 29 of 101 people aged ⩾75 had used rivaroxaban for up to 30 days before the haemorrhagic event. A similar trend was observed for dabigatran, where 91 out of 300 events among people aged ⩾75 years occurred within 30 days after treatment initiation. No products are currently licenced by the TGA to reverse the effects of rivaroxaban or dabigatran. However, idarucizumab and andexanet alfa have obtained ‘breakthrough status’ from the FDA, suggesting that a reversal agent might be on the horizon [Sarich et al. 2015].
Strengths and limitations
The strength of our study was that we included all reports of haemorrhage associated with rivaroxaban and dabigatran in Australia up until May 2014. Adverse event reports for all the currently listed indications were collected. We do not know the proportion of pharmaceutical company reports that were from clinical trials and the proportion that came from ‘real world’ practice. However, 40% of all spontaneous adverse event reports (SAERs) received by the TGA are reported by pharmaceutical companies [Australian Government Department of Health: Therapeutic Goods Administration 2015]. Another limitation common to most other analyses of SAERs was that we did not have information on the total number of rivaroxaban or dabigatran users in Australia during the study period. This means that it was not possible to report the proportion of all rivaroxaban or dabigatran users who had a haemorrhagic event. Furthermore, SAERs reporting is voluntary for the patient and health care professionals. It is likely, therefore, haemorrhages reported by pharmaceutical companies are over-represented in our data. Health care professionals may also have been more likely to report serious rather than non-serious bleeding events. This means that SAERs are unlikely to be representative of all haemorrhagic adverse events that occur in clinical practice.
There was a considerable amount of missing data. Although data on renal and hepatic function were recorded for some patients, there were insufficient data to analyse these parameters. Similarly, concomitant medication use was poorly recorded and so we decided not to analyse these data. We did not report proportions for several key parameters by age group because we believed that this would be misleading due to the large amount of missing data. Adverse event-reporting guidelines in Australia request information about any other medications patients are taking.
Conclusion
Our study emphasizes the need for research on the haemorrhagic complications of anticoagulation in clinical care. A considerable proportion of reported haemorrhagic events occurred within 30 days of rivaroxaban and dabigatran initiation. This highlights the importance of considering bleeding risk at the time of treatment initiation.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: JI was supported by a National Health and Medical Research Council Fellowship (grant number 1072137). KM was supported by a Heart Foundation postdoctoral award (grant number 100187).
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.