
Abstract
Prescribing of medicines for older people who live in nursing homes is a very common intervention. Undoubtedly, medicines have contributed to longevity and improved health outcomes in the population, but they are not without their side effects and can give rise to adverse events. The nursing home population is particularly at risk as residents have multiple comorbidities and receive multiple medications. Moreover, the quality of prescribing has been criticised with long-standing concerns about inappropriate prescribing, particularly overuse of medications which are not clinically indicated or which are no longer required. It has been suggested that pharmacists could use their skills to improve prescribing in the nursing home population and this review paper outlines the evidence for this type of intervention. The studies which have been included were rigorously designed and conducted. A number of interventions consisted of medication reviews, which often focused on specific drugs, notably antipsychotics, hypnotics and anxiolytics. In some cases, the pharmacist was solely responsible for the delivery of the intervention while in others a multidisciplinary approach was taken involving other key healthcare professionals. A number of outcome measures were employed to assess the impact of the intervention, ranging from a change in the number of inappropriate medications to differences in hospitalizations or health-related quality of life. Owing to the variation across studies, it is difficult to be definitive about the impact of pharmacy interventions in this setting. In an older, frail population such as nursing home residents, consideration needs to be given to appropriate and relevant outcome measures including a reduction in inappropriate prescribing, optimization of prescribing, reduced costs and improved health-related quality of life. Pharmacists and other healthcare professionals should continue to strive to meet these challenges in this particular demographic.
Introduction
A recent commentary highlighted the importance of medication use in a population which uses more medicines compared with other groups, that is, older people. Avorn stated ‘The use of medications in older patients is arguably the single most important health care intervention in the industrialised world’ [Avorn, 2010]. However, this same commentary proceeds to highlight some of the deficits in prescribing in older people such as under-representation of older people in trials, poorly organized care and medical education lacking instruction on prescribing in this population [Avorn, 2010].
One group of older people, those who are residents in care homes (the collective term used to describe nursing and residential homes), require particular consideration. Care homes include nursing homes which provide 24-hour nursing care, residential homes which provide personal care only and mixed care homes, which offer both residential and nursing care [Barber et al. 2009]. These residents typically receive between 8 and 10 medications [Patterson et al. 2010; Barber et al. 2009] and may have at least four active medical diagnoses [Patterson et al. 2010], all of which require careful monitoring and optimization as and when required. However, the care home sector has also been the subject of intense scrutiny and criticism in relation to several aspects of the quality of care, and prescribing is no exception. There has been a legacy of overuse of inappropriate medication and underuse of medication required for the treatment and/or management of a range of medical conditions.
One approach to tackle this problem has been the implementation of interventions focusing on prescribing, which are undertaken by pharmacists. This paper provides an overview of the evidence of the effectiveness for these types of interventions and seeks to provide an objective overview of the quality of the evidence and a critique of the approaches taken with each study. To begin with, the main problems which have arisen with prescribing in this setting are reviewed, followed by a consideration of policy and practice approaches which have been used to improve prescribing. The latter sections of the paper provide examples of key studies which have evaluated interventions performed by pharmacists (often in conjunction with other healthcare professionals), and provide a critical appraisal of the effectiveness and value of such interventions. The terms ‘care home’ and ‘nursing home’ are often used interchangeably in the literature. Much of the early literature which raised concerns about prescribing in this setting emanated from nursing homes in the United States (US), and a number of studies which examined pharmacist interventions were conducted in nursing homes. Therefore, the term ‘nursing home’ will be used preferentially in this paper.
A comprehensive search of the literature was undertaken using MEDLINE, Web of Science, Embase, CINAHL, International Pharmaceutical Abstracts, Internet searches and hand-searching of journals. Key search terms (and combinations thereof) were prescribing, nursing homes, residential homes, care homes, pharmacist, pharmacy, intervention and outcomes.
Prescribing in nursing homes: a legacy of poor practice
Prescribing is one of the most common medical interventions experienced by older people resident in nursing homes [Thomson et al. 2009; Hughes and Lapane, 2005]; residents are often the frailest old and take up to four times as many medications than their age-matched community-dwelling nonfrail older counterparts [Walley and Scott, 1995]. Owing to multiple medical conditions and polypharmacy (broadly defined as multiple medications), in addition to age-related changes in pharmacokinetics and pharmacodynamics, nursing-home residents are at high risk of adverse drug events [Alldred et al. 2007; Hughes et al. 2007]. Prescribing for this vulnerable population has been widely recognized as being poor in quality, particularly with respect to overuse of inappropriate drugs and underuse of beneficial therapies [Hughes and Goldie, 2009], and in addition to inappropriate dosages and drug interactions. There is also evidence that nursing home residents are poorly monitored with respect to chronic conditions [Fahey et al. 2003].
One particular group of medications that has attracted much attention in this setting are the psychoactive drugs, i.e. hypnotics, anxiolytics and antipsychotics. In the late 1970s and early 1980s, the prevalence of hypnotic use had been reported to be between 23% and 34% in the nursing home environment [Morgan et al. 1982; Kalchthaler et al. 1977; Ingman et al. 1975]. which was up to five times the prevalence of use seen in patients living in their own homes [Stewart et al. 1989]. A major investigation conducted by the Institute of Medicine on behalf of the US Congress suggested that these types of medications were being used as ‘chemical restraints’ to sedate and subdue residents [Institute of Medicine, 1986]. This use represented extreme violation of a resident’s individual rights as well as overt usage of medication which was not clinically indicated. In the report issued by the Institute of Medicine entitled ‘Improving the Quality of Care in Nursing Homes’, the following comment encapsulated the long-standing criticisms which had been levelled at these institutions: ‘Understaffed facilities may make excessive use of antipsychotic drugs to substitute for inadequate numbers of nursing staff’ [Institute of Medicine, 1986].
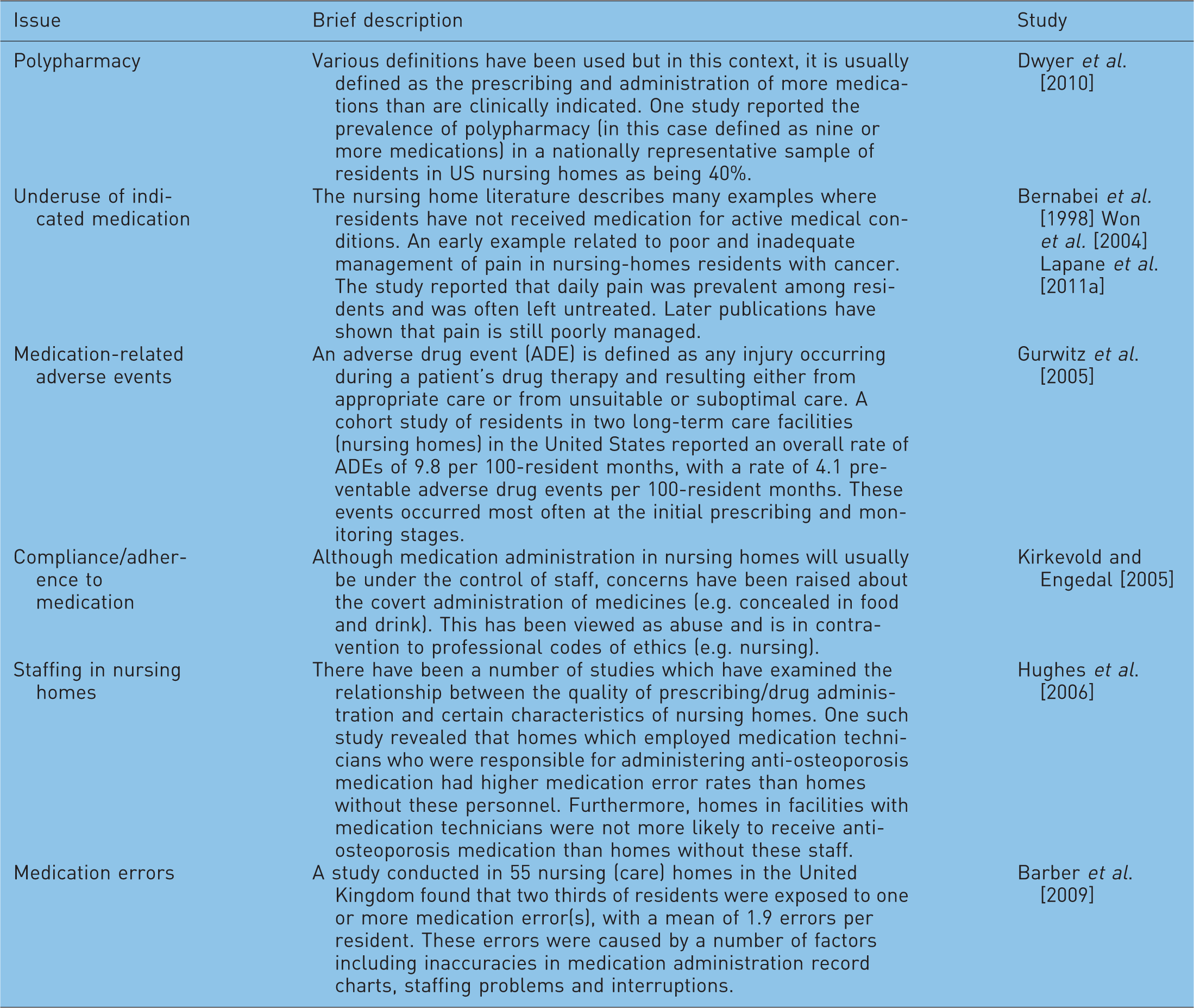
Key issues pertaining to prescribing in nursing homes.
Approaches to improving prescribing in nursing homes
The US has probably led the way in terms of attempting to address prescribing issues in nursing homes. This may be attributed to the long-standing concerns about poor quality care in the nursing home setting which led to the major investigation and report by the Institute of Medicine in 1986 [Institute of Medicine, 1986]. As a result of this report, a wide-ranging and unique piece of legislation was implemented to improve care in US nursing homes.
The Nursing Home Reform Amendment which was embedded in the Omnibus Budget Reconciliation Act of 1987 (hereafter known as OBRA 87) was implemented in October 1990 [Stoudemire and Smith, 1996; Elon and Pawlson, 1992]. OBRA 87 and its attendant regulations applied to all residents of Medicare/Medicaid (the main US government health programmes) certified facilities regardless of residents’ actual source of payment [Eichmann et al. 1992]. There are specific regulations relating to medication and prescribing, with a key requirement that each resident’s drug regimen must be free from unnecessary medicines [Tessier, 1993]. This is defined as:
medicine that is used in excessive dose; medicine that is used for excessive duration; medicine that is used without adequate monitoring; medicine that is used without adequate indications for its use.
In the context of psychoactive prescribing, the relevant regulation states that: ‘The resident has the right to be free from any psychoactive drug administered for purposes of discipline or convenience and not required to treat the resident's medical symptoms’ [Health Care Financing Administration, 1995].
There is also guidance provided as to which indications psychoactive medications can and cannot be prescribed. For example, antipsychotic agents can be used if the resident suffers from schizophrenia provided that this is clinically justified and documented, but cannot be used simply to control wandering and uncooperativeness [Health Care Financing Administration, 1995].
Adherence to the legislation is monitored by drug regimen review which is usually undertaken by pharmacists, commonly known as consultant pharmacists in the US nursing home context. These reviews are carried out monthly and should include at least an evaluation of the appropriateness of, and response to, each patient's drug therapy. The pharmacist must report any irregularities to the attending doctor and director of nursing [Hughes et al. 1999]. State surveyors (inspectors) conduct the annual nursing home assessments guided by ‘F-tags’ which denote specific topic areas for assessment. The results of the inspections are available to consumers on the Nursing Home Compare Website (www.medicare.gov/NHCompare) which allows prospective residents and/or their families to view certain indices of care in a selected nursing home compared with state and national average figures. As such, facilities have strong motivation to change practice to be in accordance with the guidance set forth in the F-tags. Indeed, recently this approach has targeted a specific area: pain management. As of 31 March 2009, F-tag 309 states that ‘each resident must receive and the facility must provide the necessary care and services to attain or maintain the highest practicable physical, mental, and psychosocial well-being, in accordance with the comprehensive assessment and plan of care’ [Centers for Medicare and Medicaid, 2009: Appendix PP, p. 9] and each ‘facility must ensure that each resident obtains optimal improvement or doesn’t deteriorate within the limits of a resident’s right to refuse treatment, and within the limits of recognized pathology and the normal aging process’ [Centers for Medicare and Medicaid, 2009: Appendix PP, p. 11]. The impact of this directed F-tag on prescribing and care quality remains to be seen.
This legislative approach has generated much interest beyond the US, but has never been replicated in any other country to the same extent. However, there has been interest in the role of pharmacists in the nursing home setting. Although the US legislation has been successful in preventing or reducing poor practice such as marked reductions in the prescribing of the psychoactive drugs [Hughes et al. 2000; Garrard et al. 1995; Rovner et al. 1992], it has been less successful at promoting best practice [Hughes and Lapane, 2005]. There has not been a diffusion effect in terms of encouraging prescribing for conditions which are undertreated. The limitations of the legislation have been recognized and there have been calls in the US for more proactive pharmacist involvement rather than drug regimen review, which by its definition, is retrospective in nature [Office of the Inspector General, 1997]. This may be achieved through different models of pharmacist intervention as outlined in the following section.
Pharmacy interventions: from evidence to practice
Pharmacists have been viewed as experts in pharmacotherapy and these skills could be exploited in the nursing home setting. The US experience of using consultant pharmacists to carry out medication review represents one practice model that has been in place for some time. Indeed, this role is mandatory in all US nursing homes which receive funding from major federal government health programmes [Levenson and Saffel, 2007]. Other countries have not followed this mandatory approach. Rather, a number of studies have been performed which have attempted to assess the effectiveness of pharmacist input into prescribing in nursing home residents. As with any intervention, the gold standard for assessment is a randomized controlled trial (RCT). However, sometimes ethical issues prevent the implementation of such a study design in a nursing home setting. The studies described in the following represent those which have been rigorously designed and rigorously undertaken. Unless otherwise indicated, the studies are RCTs.
One of the first RCTs to be conducted on pharmacist intervention was performed in Sweden by Schmidt and colleagues in 33 nursing homes [Schmidt et al. 1998a, 1998b]. This study was multidisciplinary in nature involving other key healthcare professionals such as doctors, nurses and nursing assistants. The intervention consisted of case conferences involving this team, and the focus was on the prescribing of psychoactive medications such as antipsychotics, hypnotics and anxiolytics. Prescribing data were extracted from each resident’s prescriptions, and regular meetings were held to discuss drug use with the aim of minimizing inappropriate prescribing. For those homes which received this intervention, the average numbers of psychoactive medication and therapeutic duplication did not change over time. However, there was a reduction in the prescribing of antipsychotics, hypnotics and antidepressants in the intervention sites, and staff’s knowledge on appropriate therapy improved. In the control homes, there was an increase in psychoactive medication and therapeutic duplication. The investigators recognised that the multidisciplinary nature of the intervention was key in the success of this intervention [Schmidt et al.1998a, 1998b].
Medication review as performed by pharmacists has been central to a number of intervention studies. Medication review has been defined as a review performed by a healthcare professional, taking into consideration a patient’s health status and medications, with access to full medical and care records, in conjunction with a consultation with the patient and their carer [Alldred et al. 2007]. Furniss and colleagues conducted a RCT in 14 nursing homes in England, which utilized pharmacist medication review only as a means to improve prescribing, reduce healthcare costs (e.g. general practitioner visits, hospital inpatient and outpatient appointments) and accidents and deaths [Furniss et al. 2000]. The findings from this study were equivocal. There was a decrease in the number and costs of medicines, but this was not significant, and there were no changes in other outcomes.
A number of studies have been conducted in Australia which again has involved pharmacists either as the main professional delivering the intervention, or as part of a multidisciplinary team. Roberts and colleagues implemented a programme which focussed on establishing professional relationships between pharmacists and nursing home staff, educating nurses on common issues in geriatric pharmacotherapy, and medication reviews prepared by the pharmacists [Roberts et al. 2001]. These reviews were considered by a geriatrician. There was a reduction in the number of prescribed and administered drugs, some reductions in prescribing costs, but no significant difference in survival between the two groups (intervention and control).
Three studies have been conducted by Crotty and colleagues, again in the Australian setting. In one study conducted in 20 nursing homes [Crotty et al. 2004c], the pharmacist delivered the intervention which was educational in nature. Pharmacists visited doctors and provided educational sessions (two by 30 minutes) on falls and stroke prevention. In the case of falls, guidelines were presented on prevention strategies in addition to information on risks of psychotropic medication. Stroke prevention focused on the use of aspirin, warfarin and antihypertensive medication. Although doctors expressed great interest in the intervention, it failed to have any effect on the main outcomes in terms of prescribing or falls rate. This lack of effect was attributed to the timeframe for the study (7 months) which may have been too short to see an effect, attrition of staff, and the fact that not all GPs who provided care to residents in the participating homes took part in the study (hence diluting the overall effect).
The second study [Crotty et al. 2004c] involved a multidisciplinary approach, using case conferences, which reviewed the quality of prescribing based on the Medication Appropriateness Index (MAI). The team which reviewed the medication in addition to a pharmacist included a GP, geriatrician, nursing home staff and a representative from the local Alzheimer’s Association. Secondary outcomes included monthly drug costs and behaviour problems as measured by a validated scale. There was an improvement in the MAI, but no changes in behaviour or cost.
The final study [Crotty et al. 2004b] extended some of their previous approaches to transitions between hospital and nursing home. It has been recognized that this transition is often problematic due to inadequate information and poor communication between the two sectors that can result in medication errors [Murray and Laditka, 2010; Boockvar et al. 2004]. This study [Crotty et al. 2004b] again utilized a multidisciplinary approach, centred around case conferences involving a pharmacist who specifically dealt with the transition, a family doctor, a community pharmacist and a nurse from the nursing homes. The pharmacist who coordinated the transition did so through compiling transfer summaries. These were provided to the doctor, nursing home staff and community pharmacist and provided details on changes to medication or aspects of medication which would require monitoring. The community pharmacist conducted a medication review, and a case conference involving the key personnel described above was co-ordinated by the pharmacist overseeing the transition. The primary outcome was based on a change in the MAI (as per Crotty et al. [2004a]), with secondary outcomes focused on hospital usage, adverse drug events, mobility, behaviour, confusion and pain. More appropriate prescribing was seen at follow-up based on MAI scores, and a significant improvement in pain and hospital usage in those residents receiving the intervention.
A more recent UK study was conducted [Zermansky et al. 2006] in 65 nursing homes (described as care homes in the English context), with approximately 330 residents in the intervention and control groups, respectively. This was a pharmacist-led intervention which consisted of medication review, which entailed consideration of the GP’s records and consultation with the resident and carer. Outcomes were a change in the number of repeat medication, number of falls, deaths, hospital admissions, GP consultations, Barthel index score (a measure of activities of daily living) and the Mini Mental State Examination. Significant differences between intervention and control were reported for a change in the number of medication and the number of falls, but other outcomes remained unaffected.
Ironically, in the US, which has led the way in terms of pharmacist intervention, albeit through legislation, few intervention studies have been undertaken to evaluate the benefits of pharmacist input. As described above, it has been recognized that OBRA has had limited success in promoting appropriate prescribing as its focus has been on prevention of inappropriate drug use [Hughes and Lapane, 2005]. Therefore, one professional organization which looks after the interests of consultant pharmacists in the US, the American Society of Consultant Pharmacists (ASCP), developed a more holistic model of care that has become known as the Fleetwood model. This model of care went beyond retrospective medication review. This approach encompasses prospective review, direct communication with the prescriber, and formalized pharmaceutical care planning in patients at highest risk for medication-related problems and was formally evaluated in a demonstration project conducted in North Carolina [Lapane et al. 2011b]. Although the study was originally designed as a RCT, implementing such a design would have been unethical because to do so would have required that newly trained Fleetwood pharmacists (who serviced both intervention and comparison homes) would have to withhold their skills from residents in homes randomized to receive the intervention. Instead 12 nursing homes serviced in one part of the state received the intervention while usual care continued in the comparison group located in a different region (and thus pharmacists did not service both intervention and comparison homes). The outcomes which were measured were use of potentially inappropriate medications, potential adverse drug events and mortality. Residents receiving the intervention had similar hospitalization rates, hospitalizations owing to potential adverse drug events and mortality rates as those in the control homes. A decline in the use of potentially inappropriate medications was observed earlier in the intervention homes relative to the control homes, but differences did not reach statistical significance [Lapane et al. 2011b].
This model of care had been developed specifically for the US nursing home setting, and in order for it to be of relevance beyond the US, it was recognized that adaptations would be required. This was undertaken by Patterson and colleagues with a view to evaluating the adapted model in nursing homes within the UK (Northern Ireland) [Patterson et al. 2007]. A qualitative study involving those who provide care to older people (pharmacists, GPs, nursing home managers and advocates for older people) assessed the suitability of the US Fleetwood model for implementation in the UK setting. There was general concern about psychoactive prescribing, and it was recognized that in order for the Fleetwood model to work beyond the US, pharmacists would need access to records (medical and medication), prescribers and residents. This led to the implementation of an adapted version of the Fleetwood model which focused on psychoactive medication (antipsychotics, hypnotics and anxiolytics) and an evaluation of its effects [Patterson et al. 2010]. Nursing homes in Northern Ireland were randomized to receive the intervention (n = 11) or usual care (the control sites, n = 11). Specially trained pharmacists visited intervention homes on a monthly basis for 12 months, reviewed prescribing and applied an evidence-based algorithm to assess the appropriate of psychoactive medication use. This information was fed back to prescribers (GPs). The primary outcome for the study was the proportion of residents prescribed one or more inappropriate psychoactive medication, with the secondary outcome being a change in the rate of falls. Marked reductions were seen in inappropriate psychoactive prescribing in those residents who received the intervention, but there was no effect on falls. This was attributed to inadequate statistical power to detect a reduction in falls, and the relatively poor quality of falls’ data (self-report from nursing homes) [Patterson et al. 2010]. An upcoming publication which has assessed economic outcomes from this study suggests that the intervention is cost effective [Patterson et al. 2011].
The most recent intervention used an information technology approach to identify nursing home residents at risk of falls and delirium and to implement monitoring plans with a view to reducing hospitalizations potentially due to adverse drugs events and mortality [Lapane et al. 2011c]. This was a cluster RCT with 12 homes in the intervention arm and 11 homes in the control arm. Software (Geriatric Risk Assessment Med Guide-GRAM®) which correlates medication effects with physical, functional and cognitive decline was integrated into pharmacy software to allow identification and monitoring to take place. Reports were produced by the software which identified resident-specific medications that could potentially cause, aggravate or contribute to delirium and fall risk. The reports were used by a nurse in the admission assessment to identify problems for which the resident’s medication regimen put him or her at greatest risk and by pharmacists when they were reviewing residents’ medication. Monitoring plans were put in place for such residents. Nursing staff and the pharmacists in the intervention homes were trained in how to use the reports and reminded about the medications that can contribute to falls and delirium. Although the homes using the GRAM® software experienced rates of falls, potential delirium and mortality less than the nursing homes receiving usual care, the hospitalization rates were higher in the intervention homes. None of these differences reached statistical significance. Newly admitted residents in the intervention homes (vs. usual care homes) experienced a significant reduction in the rate of potential delirium onset. This study provides evidence of the need for prospective intervention on admission to nursing home [Lapane et al. 2011c].
Assessing the outcomes of pharmacist intervention
The studies summarized above represent those of high quality which have attempted to evaluate, in a rigorous way, the impact of pharmacist interventions in nursing homes. The studies have some commonalities. The process of medication review was central to many of the studies, psychoactive medication was often the focus for pharmacist input (reflecting the legacy of concern with regards to these drugs), and a number of studies attempted to involve other key health professionals such as the nursing home staff and GPs. However, what is also noteworthy is the range of outcome measures which have been used across all studies. In some, the outcome measure was based on the number of drugs, while other studies selected more clinically relevant outcomes such as adverse drugs events, hospitalizations or falls. This spectrum of outcome measurement represents one of the great difficulties in conducting work on improving prescribing, particularly in this population and measuring some of these outcomes.
Outcomes research has traditionally categorized outcomes as clinical, economic and humanistic (health-related quality of life). Whether changes in prescribing, e.g. a reduction in the number of drugs, is translated into better outcomes (based on the categorization above) is debatable. Studies that have used quality-of-life measures as outcomes following the implementation of new models of care, or medication review, have found little change [Pacini et al. 2007; Bernsten et al. 2001]. In considering such measures applied in a nursing home population, an improvement in health-related quality of life may be unrealistic; a reduction in the decline of a quality-of-life measure may be the most that could be expected. Studies that have used a health-related quality-of-life measure in older people have found that it is not sensitive to changes in inappropriate prescribing [Franic and Jiang, 2006]. Whether a reduction in inappropriate prescribing is enough to prevent hospitalization of a frail older person with multiple comorbidities is also uncertain, and clearly, some of the studies above suggested that it is not sufficient.
Conclusion
Prescribing dominates medical management of older people and this is brought into sharp relief in the nursing home setting. Surprisingly, there is an inverse relation between the severity and extent of problem prescribing in nursing homes and the number of intervention studies to learn how to improve prescribing. This may be in part owing to the difficulty in conducting these studies because of issues relating to gaining access to nursing homes, obtaining informed consent from vulnerable residents and engaging staff in the research process. Such studies are often challenged by insufficient resources to conduct the trial for an extended period or to implement laborious, but accurate assessment of adverse drug events. In the absence of such resources, acceptance that reduction in the use of inappropriate medications is a clinically relevant outcome which long term would benefit residents should be considered. Conversely, there is also the neglected problem of under-use of potentially beneficial medications. This means being able to strike a balance between ‘many drugs’ (which are appropriate) and ‘too many drugs’ (which are inappropriate) [Aronson, 2004]. Such undertreatment is an important outcome with clinical relevance that is not often studied [Aronson, 2004; Gurwitz, 2004], particular in the nursing home population.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that they have no conflict of interest.