
Abstract
Epidermal necrolysis, whether involving limited, that is, Stevens–Johnson syndrome (SJS), or large, that is, toxic epidermal necrolysis (TEN), areas of the skin surface, is associated with high mortality. A specific prognosis score (SCORTEN) accurately predicts mortality. Management of SJS and TEN mainly relies on supportive care but several treatments have been proposed, particularly corticosteroids and intravenous immunoglobulins (IVIG), to block the progression of the disease. The aim of this study was a pooled analysis of published series addressing the question of treatment efficacy by comparing the mortality observed to the mortality predicted by the SCORTEN score. A literature search was carried out through PubMed from January 2001 to December 2009. It found 47 original series including at least 10 patients. Among these, 13 containing a clear description of treatment(s) and an evaluation of SCORTEN score were analyzed allowing the calculation of a mortality ratio (MR) for each series and a pooled MR with 95% confidence interval (CI) for each treatment. The analyzed series comprised a total of 439 patients. Supportive care was used only in 199 patients with a pooled MR of 0.89 (CI 0.67–1.16, p = 0.43), corticosteroids were administered to 78 patients with a pooled MR of 0.92 (CI 0.53–1.48, p = 0.84), and IVIG in 162 with a pooled MR of 0.82 (CI 0.58–1.12, p = 0.23). In conclusion, even though this analysis had some limitations, it strongly suggested that neither corticosteroids nor IVIG provide any important reduction in the risk of dying from SJS and TEN.
Keywords
Introduction
Epidermal necrolysis is an acute life-threatening mucocutaneous reaction characterized by extensive necrosis and detachment of the epithelium of the skin (epidermis) and many mucous membranes. Most often resulting from hypersensitivity to drugs, it includes Stevens–Johnson syndrome (SJS), toxic epidermal necrolysis (TEN), and overlap SJS/TEN, based on the extent of skin area involved [Mockenhaupt, 2009]. Necrosis of the epithelium is likely initiated by drug-specific cytotoxic T cells and nonspecific cytotoxic cells that kill epithelial cells directly [Nassif et al. 2004], and also indirectly through the release of soluble death mediators, the principal being granulysin [Chung et al. 2008]. To some extent the process is close to what happens during the acute rejection of a skin graft. Epidermal necrolysis is occasionally observed in a context of acute graft-versus-host disease after bone marrow transplantation [Friedman et al. 1984]. As an immunological mechanism had been suspected long before recent evidence, ‘specific’ therapeutic interventions proposed over years included corticosteroids, immunosuppressive drugs, and agents expected to block soluble death mediators or their receptors. Among the latter, thalidomide was used because of its antitumor necrosis factor alpha activity [Wolkenstein et al. 1998], and high-dose intravenous human immunoglobulins (IVIG) because of their Fas-ligand blocking activity [Viard et al. 1998].
With the exception of thalidomide that proved detrimental, none of the proposed treatments was evaluated in a randomized controlled trial (RCT). The main reasons are the extreme rarity of the disease, with an incidence estimated to be around two cases per million inhabitants per year [Rzany et al. 1996].
The present consensus is that to date there is no validated treatment capable of stopping progression of the disease, and that the main focus of management should be on supportive measures in specialized centers [Endorf et al. 2008]. Even in the best centers, the mortality of SJS and TEN is high, with an overall death rate averaging 20–25% [Schneck et al. 2008], ranging from 10% in SJS to more than 40% in TEN, according to classification by extent of detachment that is widely accepted nowadays [Bastuji-Garin et al. 1993].
The SCORTEN is a prognosis score elaborated specifically for SJS and TEN [Bastuji-Garin et al. 2000], and subsequently used and validated by many teams. It is calculated on arrival at a specialized unit and provides an accurate estimation of the risk of death [Guégan et al. 2006; Palmieri et al. 2002]. This score was elaborated and validated in two cohorts of patients only treated by usual supportive care.
The rarity of SJS/TEN and the dispersion of patients in a variety of hospital wards make it very difficult to carry out RCTs. Large RCTs are only feasible within the organization of a global network of reference centers each treating more than 12 patients a year. While waiting for such an opportunity, several teams have used the SCORTEN as an ‘internal control’ and compared the mortality rates observed when using a therapeutic intervention to those predicted by the SCORTEN.
The aim of the present study was to provide an overall evaluation of all published studies on SJS and TEN that used the SCORTEN score as a marker of the possible efficacy of a treatment.
Material and methods
Systematic literature review
The objective was to find all published series of SJS/TEN that included at least 10 patients, described modalities of treatment, and used the SCORTEN score to compare observed versus predicted mortality (a priori criteria defined before the literature search).
All articles published between January 2001 (SCORTEN was published in 2000) and December 2009 were searched in PubMed with no limitation on language. Search terms included SJS or TEN AND with successively each of the following: prognosis, mortality, treatment, corticosteroids, intravenous immunoglobulins, cyclosporine, plasmapheresis, SCORTEN, that is a total of 16 queries.
These queries obtained a total of 2151 references. We also reviewed the reference lists of articles with information on the topic, but no additional pertinent studies were retrieved. After depletion of duplicates and references with titles indicating a single case report or a review, we read all English language abstracts and selected 47 original series (46 in English, one in French), including at least 10 patients. Full texts of these publications, not blinded for author names, were analyzed in detail by the two authors to result in the pooled analyses of all 13 series that fulfilled the predefined criteria. The others were not included because SCORTEN had not been used (n = 29), the treatment was not specified (n = 3), several treatments had been used without evaluation in subgroups (n = 1), or because the study focused on long-term follow up and not on the effect of early treatment (n = 1).
No series fulfilling our criteria mentioned a treatment other than supportive only, corticosteroids, or IVIG. Published series where plasmapheresis or cyclosporine had been used in more than 10 cases did not refer to SCORTEN. Four of the 13 papers analyzed included a historical comparison of two treatment modalities: supportive only versus IVIG [Imahara et al. 2006; Brown et al. 2004], corticosteroids versus IVIG [Kim et al. 2005], and corticosteroids alone versus corticosteroids + IVIG [Yang et al. 2009].
The nature of the supportive care and doses of corticosteroids or IVIG were sometimes not detailed. We therefore grouped all cases treated with symptomatic measures only (group 1), corticosteroids only whatever the dose (group 2), or IVIG only whatever the dose (group 3). With regard to the series by Yang and colleagues, only the 45 cases treated with corticosteroids only were included in group 2, the 20 cases treated with both corticosteroids and high-dose IVIG were not included [Yang et al. 2009].
Analyses
In each series, the number of deaths observed (O) among patients was compared with the number of deaths predicted (E) by the initial SCORTEN score using the mortality ratio (MR = ΣO/ΣE) with 95% confidence interval (CI). The 95% CI was calculated as for the standardized MR [Breslow and Day, 1987]. When MR and 95% CI were provided in the original publication, recalculation always provided the same figure. The between-study heterogeneity of MR was graphically assessed in each group (1, 2, and 3). Furthermore, when individual patient values were available, we tested whether SCORTEN varied across studies within the same therapeutic group using the nonparametric Kruskal–Wallis test with Dunn’s posttest for multiple comparisons. The pooled estimates of MR and 95% CI were calculated in each group by summing the numbers of observed and predicted deaths. When heterogeneity was suspected, analyses were also performed after exclusion of the series that appeared to be the source of heterogeneity. The chi-square test was used to assess whether the MR was different from 1 [Samuels et al. 1991].
Results
The series analyzed included 439 cases of patients hospitalized for treatment of SJS, overlap SJS/TEN, or TEN between 1980 and 2007 in 13 different centers (seven dermatology/intensive care units and six burn units). A total of 199 patients (45%) had been treated by supportive care only, while 78 (18%) had also received systemic corticosteroids, and 162 (37%) had been given high-dose IVIGs.
Characteristics of all series included in the study.
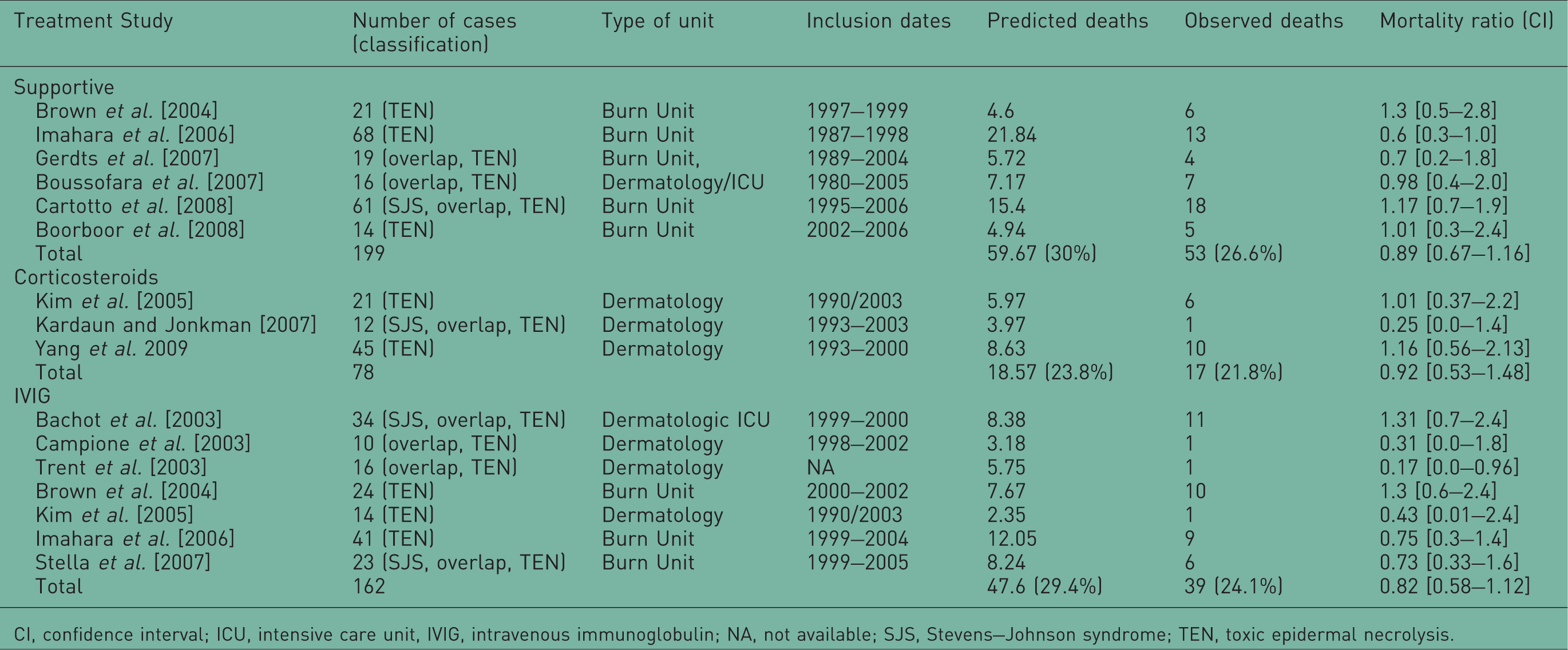
CI, confidence interval; ICU, intensive care unit, IVIG, intravenous immunoglobulin; NA, not available; SJS, Stevens–Johnson syndrome; TEN, toxic epidermal necrolysis.
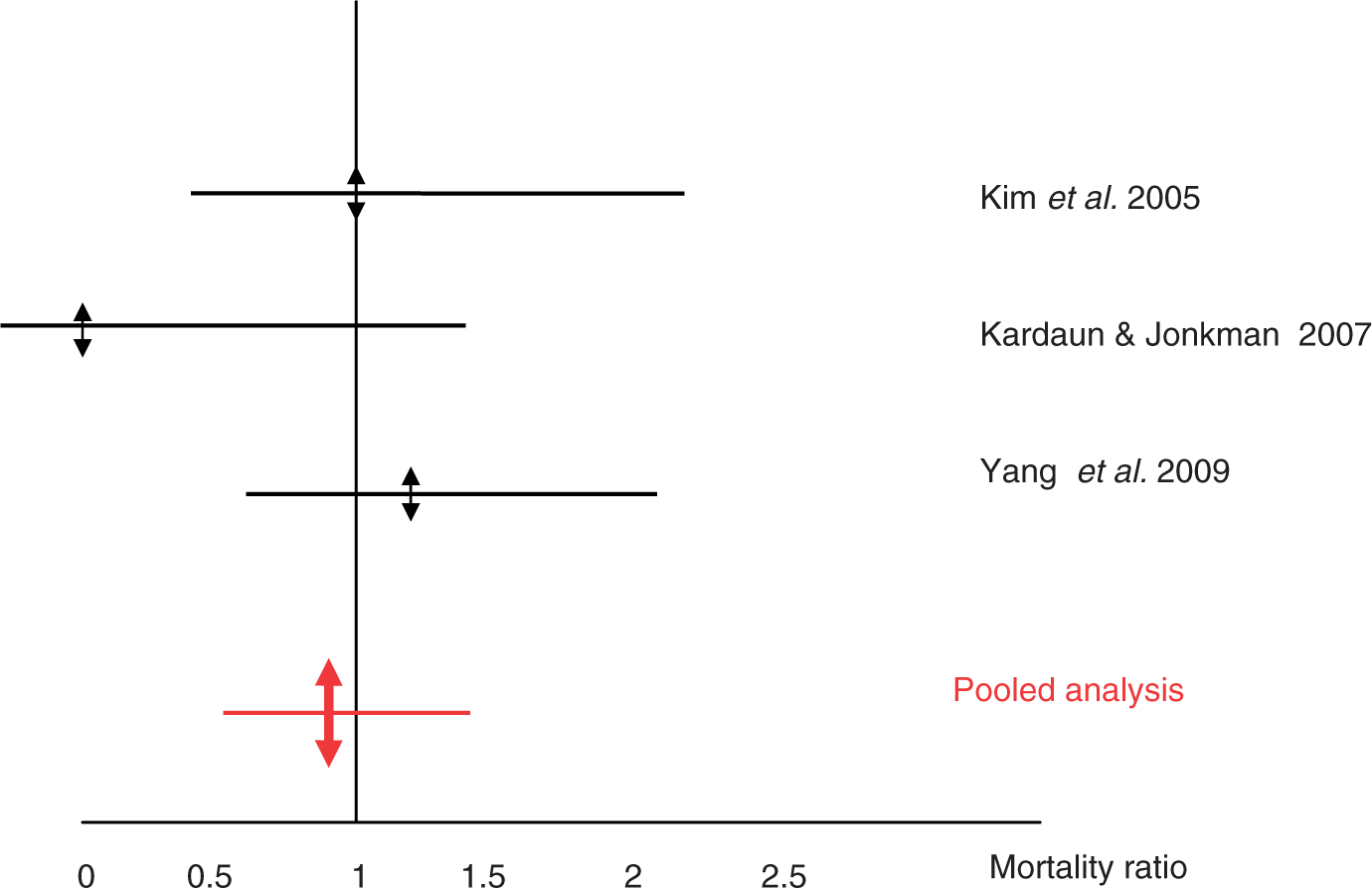
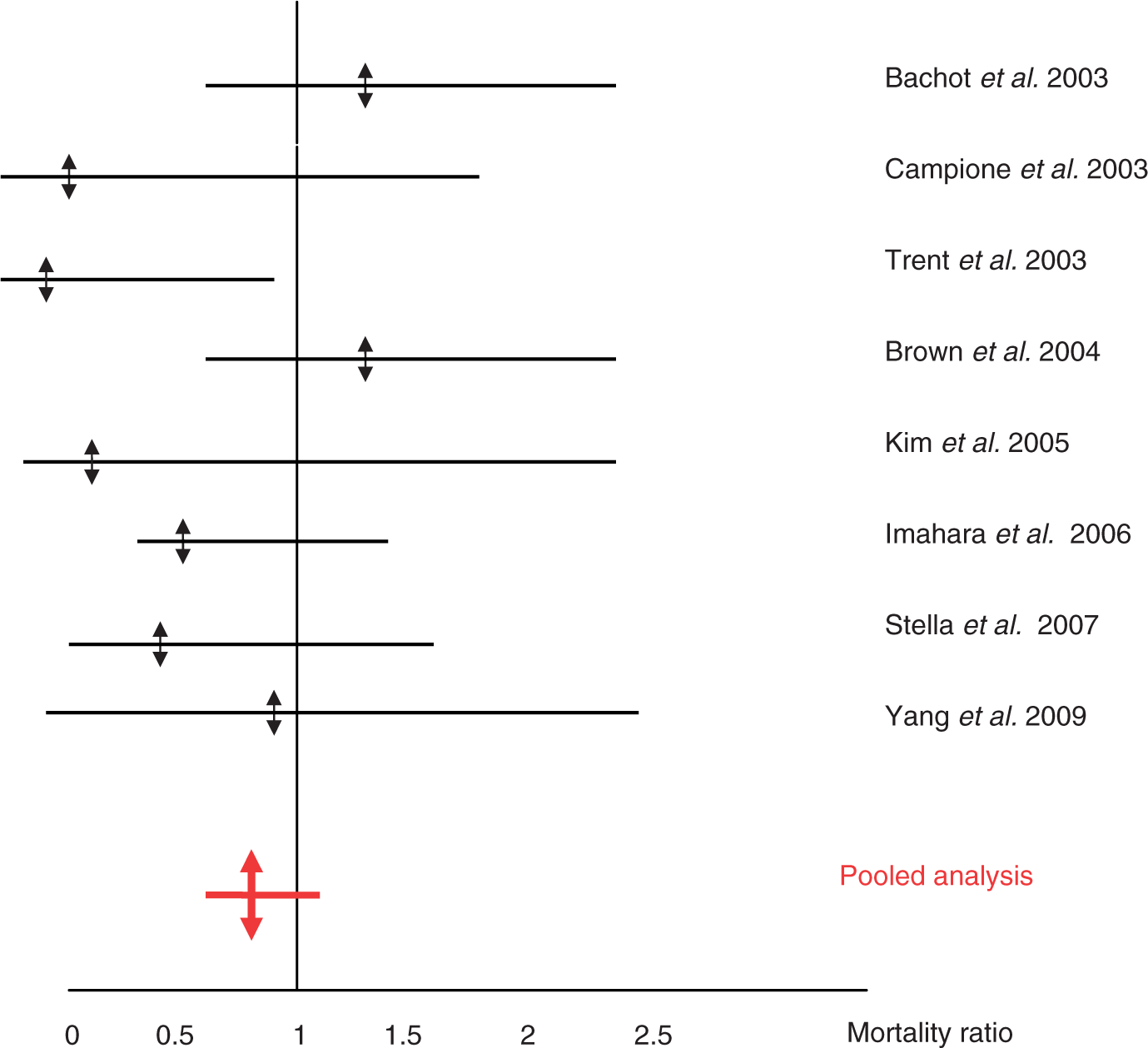
Figures 1–4 are graphical presentation of MRs and 95% CI. The large overlaps of MR within each therapeutic group do not suggest a problematic hetererogeneity between the included series. In two series, however, there is a borderline significant decrease in MR: 0.17 [0.0–0.96] in a series of 16 patients treated with IVIG [Trent et al. 2003], and 0.6 [0.3–1.0] in a series of 68 patients treated with supportive care [Imahara et al. 2006]. In both corticosteroid and IVIGs groups, SCORTEN score did not statistically differ across the series (p = 0.57 and p = 0.12, respectively), while a significant difference was observed for the conservative series (p = 0.03). The posttest indicated that the SCORTEN score observed in the study by Boussofara and colleagues was higher that observed in the series by Brown and colleagues (3.25 ± 1.39 versus 2.14 ± 1.28; p < 0.05) [Boussofara et al. 2007; Brown et al. 2004]. The MRs were, respectively, 0.89 [0.67–1.16], p = 0.43 in the group with supportive care only, 0.92 [0.53–1.48], p = 0.84, in the group receiving corticosteroids, and 0.82 [0.58–1.12], p = 0.24, in the group receiving IVIGs. The exclusion of the study by Boussofara and colleagues did not change the MR of the group with supportive care only (MR = 0.88 [0.64–1.17], p = 0.42).
Graphical presentation of mortality ratios in series with supportive treatment alone. Graphical presentation of mortality ratios in series with corticosteroid treatment. Graphical presentation of mortality ratios in series using intravenous immunoglobulins. Comparison of pooled mortality ratios by treatments.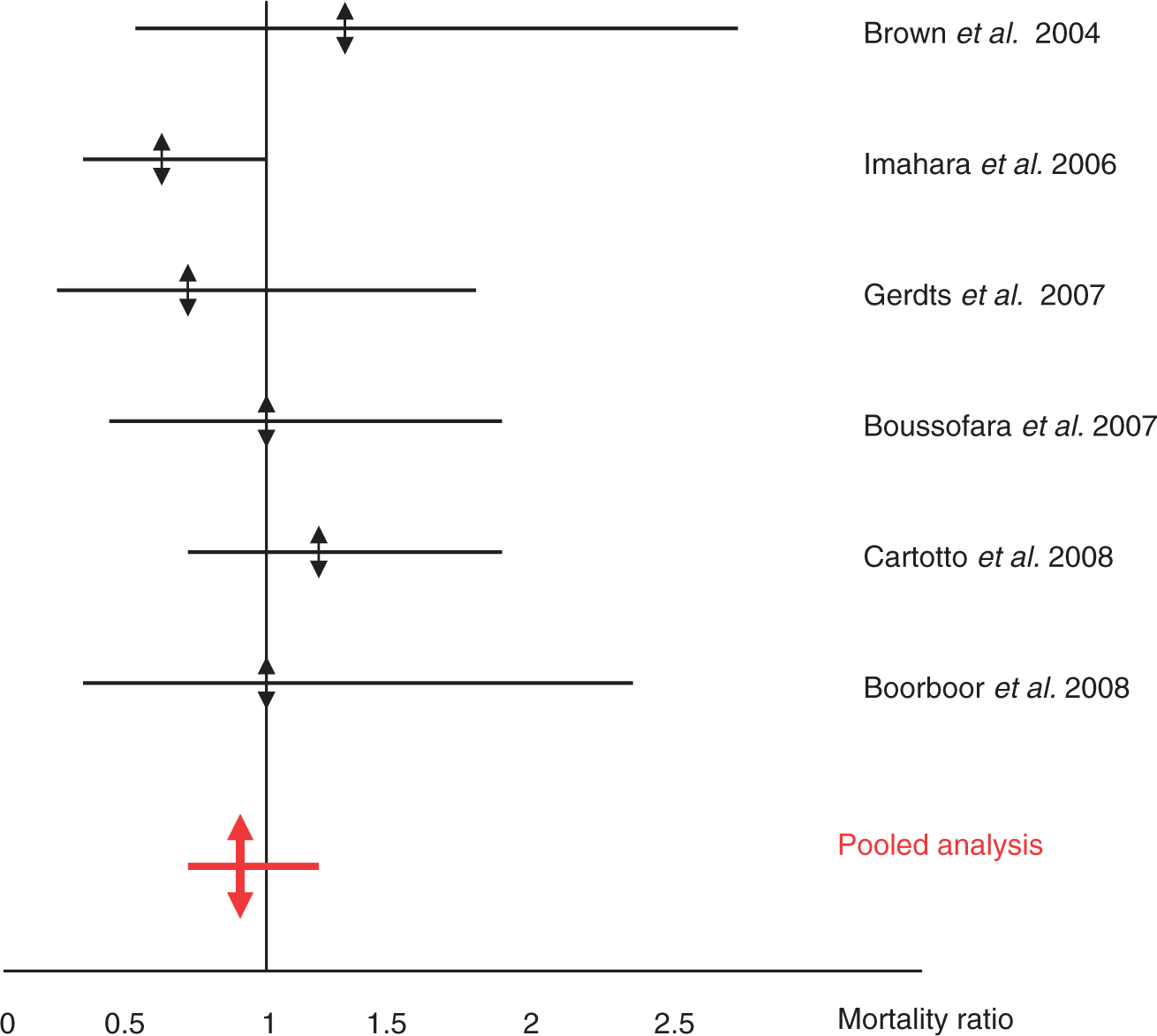
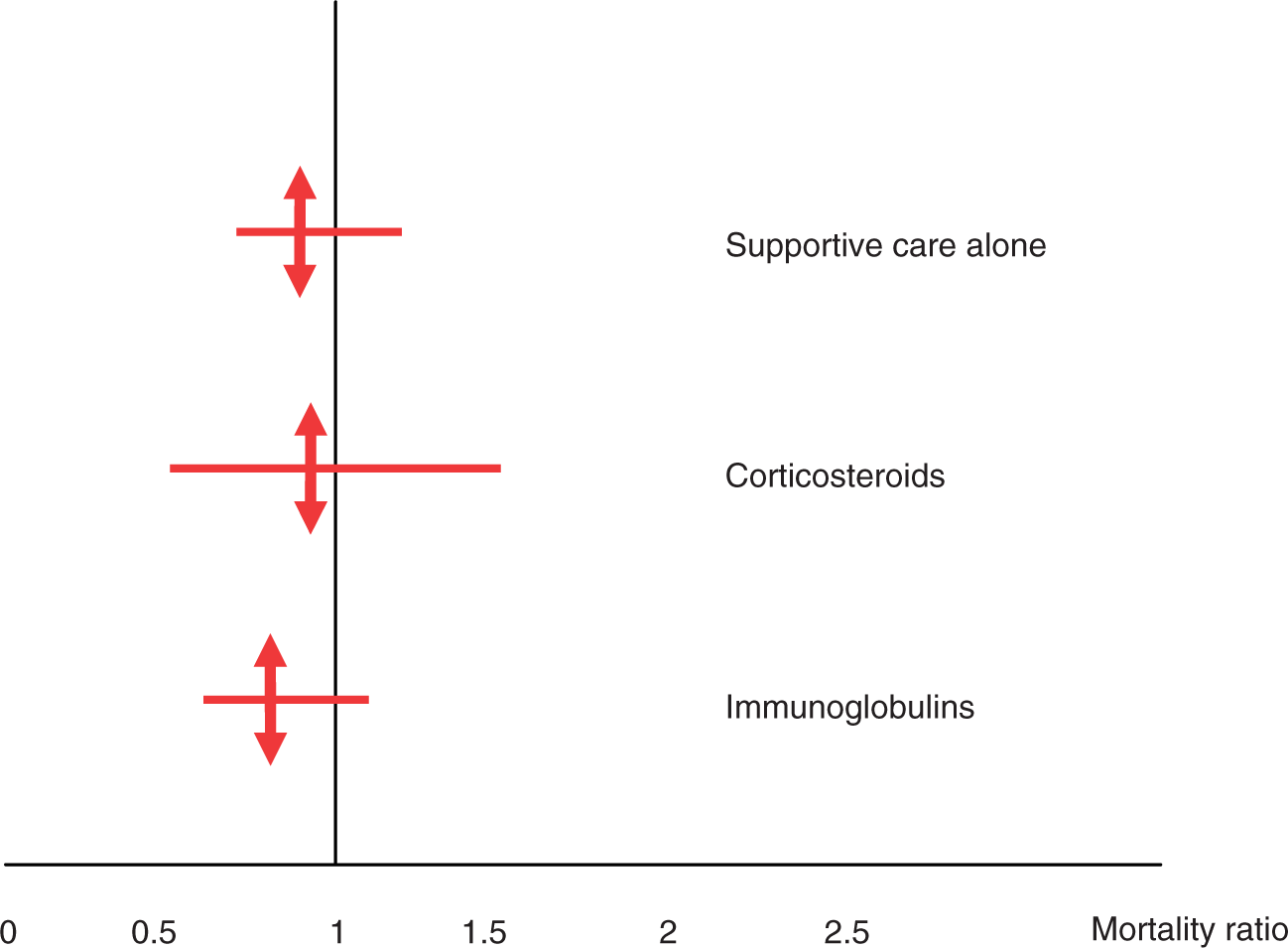
Graphical presentation also shows the overlaps between the CIs of the three overall MRs (Figure 4).
Discussion
This study is the first pooled analysis of treatments of SJS/TEN using SCORTEN as a kind of internal control allowing the comparison of observed versus predicted mortality. Since SCORTEN has been shown to be an accurate tool for measuring the severity of SJS/TEN and predicting final mortality when performed on patient admission [Cartotto et al. 2008; Guégan et al. 2006; Palmieri et al. 2002], we based our study on the hypothesis that any effective treatment would reduce the MR calculated as the observed/predicted MR.
To minimize the risk of publication bias (small series being more likely to be accepted with ‘positive’ results), we had decided arbitrarily to include only series reporting at least 10 cases. We are confident that our literature search did not miss such series in the time period selected, because all the included series were found several times (median four times, range 3–12) with various combinations of the selected keywords.
Our work did not avoid all limitations. First, the arbitrary limit of 10 cases led to a huge disparity in the size of included studies. Second, the supportive treatment was not always well described and likely differed between centers. Third, doses of corticosteroids or IVIG also varied with studies. Series also differed by distribution of cases by severity. Some included only TEN, and others both SJS and TEN. Definitions used for separating SJS from TEN were not always provided and overestimation of the extent of skin detachment was a frequent problem that may result in upgrading the SCORTEN score by 1 point. Unfortunately, there was no way to check the hypothesis concerning a bias that, if present, would more likely affect less experienced centers, that is, smaller series. We did not try to classify the 13 included series according to their strengths and weaknesses but only looked at statistical heterogeneity regarding the MRs.
We included all cases in the spectrum of SJS and TEN (SJS, overlap, and TEN), principally because the SCORTEN had been constructed and validated in such a population [Guégan et al. 2006; Bastuji-Garin et al. 2000], and also because the death rate from SJS is actually much higher [Schneck et al. 2008] than that often quoted when papers still confounded SJS and erythema multiforme major.
Overall the numbers of observed deaths were slightly inferior to those predicted by the SCORTEN score in all groups without any significant difference related to treatment group. The MR was slightly lower in series using IVIG. This was not significant and may result from remaining publication bias for small series, and also from improvement in supporting measures with time, the IVIG series being the more recent. If really related to some efficacy of IVIG, the reduction in mortality compared with supportive care would be about 10% (e.g. reduction from 29% to 24%).
In our opinion, the present results are more credible than the many prior reviews that compiled series of patients treated with IVIG without any internal control, and often added publications that partly included the same cases. Such duplication of cases is very unlikely in the selected series because all were published by a single center without any overlap in authors’ names.
The present results slightly differ from those of the EuroSCAR cohort study by showing no trend towards a benefit from corticosteroids [Schneck et al. 2008]; however, they do agree that no treatment is obviously effective. We consider, therefore, that our results reinforce the current consensus that no ‘specific’ treatment of SJS/TEN can be considered of established value and that the priority should be to remain on supportive measures [Endorf et al. 2008]. We will certainly not conclude with the usual suggestion that a RCT should be conducted, in fact, a RCT comparing IVIG with supportive care with the aim of demonstrating a 10% reduction in mortality would need to include 355 patients per arm (for a type I error of 0.05 and a type II of 0.20). Such a study is obviously not feasible given the rarity of the disease, the dispersion of patients in many centers, and likely disparity in the quality of supportive care.
Rather, we suggest that SCORTEN could be used as an internal control for evaluating the possible benefit of a treatment in open prospective trials. A clinically meaningful (i.e. important) reduction in mortality could be initially detected in a series of 30–50 patients and confirmed in a larger one.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
J.-C. Roujeau has contributed his expertise to a variety of pharmaceutical companies concerning the causality of severe cutaneous adverse reactions. He received financial support for two therapeutic studies on SJS/TEN (from Laphal for a RCT of thalidomide 15 years ago and from Novartis for a pilot trial of cyclosporine 2005–2007).