
Abstract
Objective:
A reliable database on the causes and contributing factors of medication errors can inform strategies for their prevention. To form a single database from multiple databases requires a process of integration that both maximizes the utility of the new data and minimizes the loss of information. Unfortunately, the terminologies used by different studies and databases may limit integration; therefore, terminologies must be standardized prior to integration.
Methods:
The National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) Taxonomy of Medication Errors was applied to standardize the different terminologies in 11 studies that reported the causes or contributing factors of medication errors.
Results:
After standardization, 57% of the reported causes and contributing factors were integrated to form a database while 43% were not integrated because the terminologies could not be standardized or were not similar to the taxonomy.
Conclusions:
This study highlights the challenges to standardizing and integrating databases and the importance of adopting and applying a standardized terminology to record medical errors.
Introduction
Medication errors are the most common type of medical errors and one of the leading causes of iatrogenic injuries [Michaels et al. 2010; Institute of Medicine, 2000]. Around 106 medication errors are believed to occur every 1000 patient days [Kane-Gill et al. 2006]. In 2009, the World Health Organization Patient Safety identified adverse drug events (ADEs) as one of the top six priority areas for patient safety research in countries in transition as well as developed countries [World Health Organization, 2009].
Information on ADEs arising from medication errors plays an important role in understanding the causes and contributing factors to those events and their mitigation [Shah et al. 2004]. A database on ADEs can identify dominant causes and contributing factors to medication errors which will aid resource-limited organizations in prioritizing their interventions.
Critical steps in this process are the coding of ADEs arising from medication errors using a valid taxonomy and the aggregation of coded ADEs into a usable database. This process is typically undertaken by a single institution or a large network of institutions using a common database. However, there is a range of medication error ADE databases used by institutions and networks within and between regions. At this broader level, researchers, policy makers and clinicians, may seek to synthesize a single ADE database by aggregating data from a range of databases. Developing a database using information from different studies and databases is challenging because studies may utilize different terminologies [Runciman et al. 2009]. For example, studies may utilize different terms to describe a ‘potential adverse event’, including ‘near miss’ and ‘close call’. Another example would be ‘adverse event’, ‘adverse reaction’ and ‘complication of care’ [Weingart, 2005]. The similar terms may be interpreted as such and grouped together or interpreted as being different and separated in a database.
The World Health Organization acknowledged that different terminologies cause difficulties in integrating information from different studies and databases [Runciman et al. 2009]. To overcome the difficulty, a standard terminology was developed to enable different organizations to utilize a similar terminology when reporting medical errors [Runciman et al. 2009]. Although a standard terminology may be very useful to aggregate new data, it is not known whether a standard terminology can be used to integrate existing information coded using different terminologies. In order for such integration to occur, the different terminologies will first have to be translated into a single terminology by using a standard terminology. If this is possible, greater value will be derived from existing databases and studies that use different terminologies. In this study, we aimed to:
standardize the different terminologies used to report the causes and contributing factors of medication errors using a single terminology; integrate and report the common causes and contributing factors of medication errors to form a database; examine whether the integration process affected how medication errors were understood.
To achieve the objectives, the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) Taxonomy of Medication Errors was selected [NCC MERP, 1998]. This taxonomy was selected as the ‘standard terminology’ because the taxonomy contained sections on the causes and contributing factors of medication errors. The section on the causes of medication errors includes communication, name confusion, labelling, human factors and packaging/design as major categories. The major categories are divided into subcategories, with each subcategory providing a more specific description compared with the major category. The section on contributing factors of medication errors lists a variety of systems-related contributing factors, including lighting, noise, staffing, policies and procedures, and frequent interruptions and distractions.
Methods
To compile the reported causes and contributing factors of medication errors, a literature search was performed by the first author using the following databases: Embase (1980–2010), Medline (1950–2010) and Web of Science (1900–2010). The keywords used were ‘medication error’, ‘cause’ and ‘factor’. For the first phase, the title and abstract of retrieved articles were read to determine whether the studies reported the causes or contributing factors of medication errors. Articles not in English were rejected. Only articles that reported the causes or contributing factors of medication errors for a particular domain were selected for the second phase. Articles that reported the causes or contributing factors of medication errors specifically for a particular procedure were not selected for the second phase. For example, articles that discussed the causes or contributing factors in an intensive care unit were selected while articles that discussed the causes or contributing factors of medication errors during medication administration were not selected for the second phase. The reason articles about particular procedures were excluded was because such articles may utilize procedure-specific terminologies. In addition, the objective of this study was to determine the possibility of using a medication error taxonomy to integrate causes and contributing factors of medication errors reported by studies in different domains, such as intensive care and general care units. In the second phase, the full articles of selected articles were reviewed by the first author and the reported causes or contributing factors of medication errors were compiled. Only the top five causes or contributing factors of medication errors from each article were considered.
For the third phase, the reported causes or contributing factors were integrated to form a database by the first author. The reported causes or contributing factors were standardized into a single terminology based on the NCC MERP Taxonomy of Medication Errors. To standardize the terminology, each reported cause or contributing factor was examined to determine whether a corresponding category existed in the taxonomy. If a corresponding category existed, the reported cause or contributing factor was replaced by the corresponding category. The corresponding category was then selected for integration process. Each reported cause or contributing factor was examined to see whether a similar category existed in the taxonomy. If a similar category existed, the reported cause or contributing factor was then selected for integration. The reported causes or contributing factors that did not have corresponding categories in the taxonomy or were not similar to categories in the taxonomy were not integrated. Information selected for integration were then grouped based on the NCC MERP Taxonomy of Medication Errors to form a database on causes and contributing factors of medication errors. The database was then analysed to determine the frequency of the causes and contributing factors.
Results
The causes and contributing factors of medication errors as reported by different studies.

The causes and contributing factors of medication errors reported by different studies (after standardization process).

Italic, standardized according to the NCC MERP Taxonomy of Medication Errors, integrated;
The reported causes and contributing factors that were standardized (n = 31) or were similar to the categories in the taxonomy (n = 12) were integrated for analysis. The total number of causes and contributing factors integrated was 43 (57%). Thirty two (43%) reported causes and contributing factors were not integrated because their terminology cannot be standardized by using the taxonomy or their categories were not similar to the taxonomy.
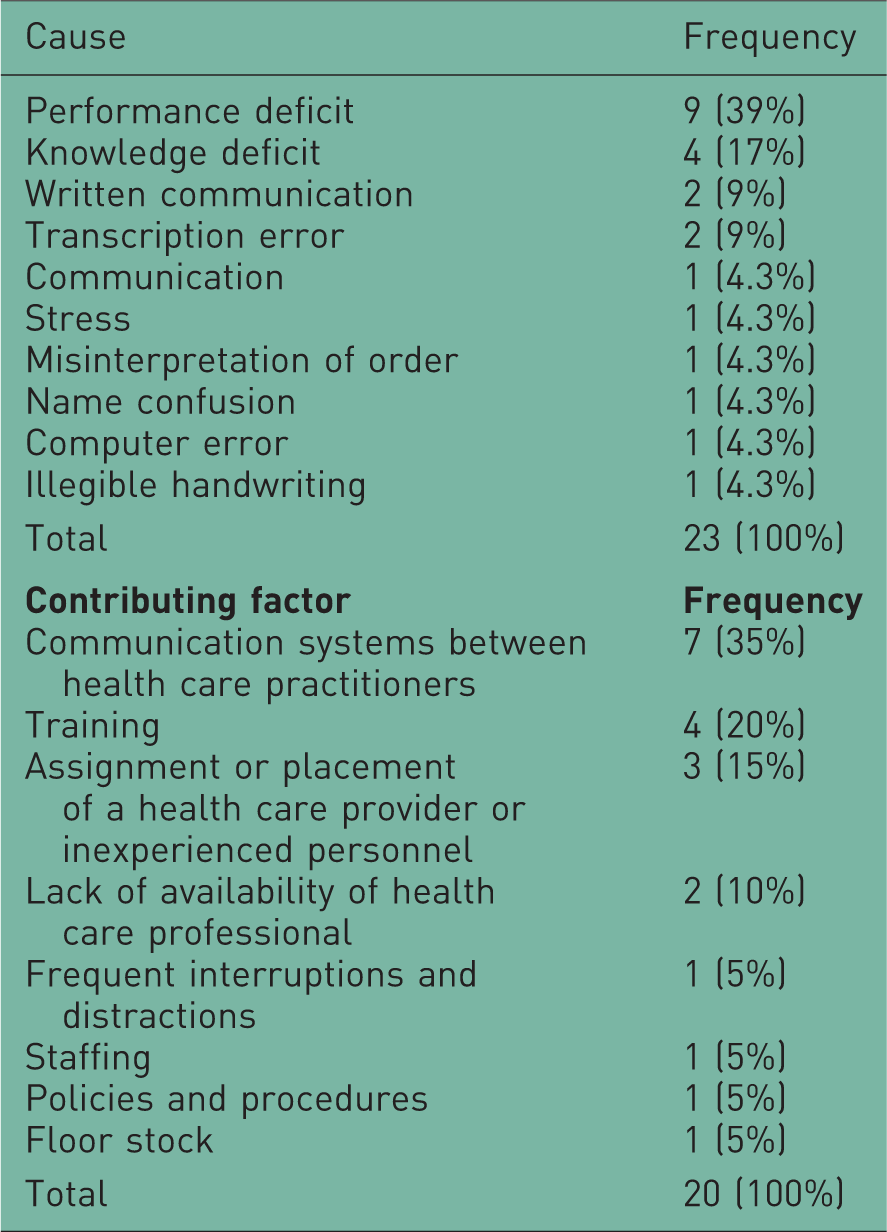
Frequency of reported causes and contributing factors after the integration process from 11 articles.
Discussion
Factors affecting integration of information
The findings indicate that although different studies used different terminologies to report causes or contributing factors of medication errors, we were able to integrate the information from the reports into a single database using a medication error taxonomy. The study utilized the NCC MERP Taxonomy of Medication Errors to standardize the different terminologies, and this enabled the integration of 57% of the reported causes or contributing factors of medication errors into a database. Ideally, a taxonomy utilized for such purpose would have integrated a higher percentage of information. However, in this study, two factors prevented the taxonomy from integrating more information.
First, each publication defined the causes and contributing factors of medication errors differently to the taxonomy this study utilized. This in itself is noteworthy, as it reflects the wide variety of taxonomies used in this field. For example, in the study by Kane-Gill, Kowiatek and Weber [Kane-Gill et al. 2010], ‘workflow disruption’ was identified as a cause of medication errors. In the NCC MERP Taxonomy of Medication Errors, the most similar category to workflow disruption would be ‘frequent interruptions and distractions’; however, this category was defined by the taxonomy as a contributing factor of medication errors, instead of a cause of medication errors. Owing to this difference, ‘workflow disruption’ was not integrated into the database. Second, the different studies reported causes or contributing factors of medication errors that did not have corresponding categories or similar categories in the taxonomy. For example, the studies by Senghera, Franklin and Dhillon [Sanghera et al. 2007] and Kopp and colleagues [Kopp et al. 2006] reported ‘violations’ as a cause of medication errors. Violation was not available as a category in the NCC MERP, neither was there any category similar to it; therefore, the information was not integrated into the database. Judging by the amount of information that failed to be integrated, it was felt that the NCC MERP Taxonomy of Medication Errors was incomplete for integrating information from different sources, and new categories, such as ‘violations’ and other information reported by the different studies, can be added to expand it. Such expansions can increase the amount of information that can be integrated to form the database.
Causes of medication errors
The database indicated that the three most frequent causes of medication errors were ‘performance deficit’, ‘knowledge deficit’ and ‘written communication’. In our study, performance deficit was interpreted as personnel not performing as intended. Performance deficit was used to standardize terms such as ‘slip’, ‘lapse’ and ‘not concentrating or careless’. Steps that may reduce performance deficit include reducing workplace fatigue, and this can be done through better work schedules and workload distribution [Institute of Medicine, 2007]. Knowledge deficit was interpreted as not having sufficient information about a procedure or material. Knowledge deficit was used to standardize terms such as ‘lack of knowledge’ and ‘unfamiliarity with medication’. Knowledge deficit may be reduced by providing access to required information. For example, having a pharmacist available during rounds at wards or available by phone after office hours may prevent medication errors due to unfamiliarity with medications [Institute of Medicine, 2007]. Written communication was used to standardize ‘written order’ and ‘written miscommunication’. Medication errors caused by written communication can be reduced by eliminating the use of certain abbreviations in written communications and by adopting computerized communication systems [Institute of Medicine, 2007].
Contributing factors to medication errors
The database indicated that the three most frequent contributing factors to medication errors were ‘communication systems between health care practitioners’, ‘training’ and ‘assignment or placement of a health care provider or inexperienced personnel’. Communication systems between health care practitioners included ‘verbal communication systems’ and ‘written miscommunication’. The contributing factor suggests the need to improve existing communication systems. Training included ‘lack of knowledge’ and ‘knowledge deficit’. The contributing factor suggests the need to improve training and supervision. Assignment or placement of a health care provider or inexperienced personnel included ‘inexperience’. The contributing factor suggests the need to improve training and supervision.
The need for more specific categories
It was difficult to propose any interventions based on the database alone. The standardized terminology did not provide sufficient information. It did, however, provide an overview of the causes and contributing factors of medication errors. In the discussion above, the preventive steps for causes and contributing factors were identified by using the information reported in the different studies, and not the database alone. For example, the term ‘knowledge deficit’ alone did not reveal sufficient information upon which to base interventions. However, because we knew that ‘knowledge deficit’ was used to standardize lack of knowledge and unfamiliarity with medications, it could be used to target the lack of knowledge about medications. Another example is the phrase ‘communication systems between health care practitioners’. This phrase alone does not illuminate the underlying issues.
It is likely that the ‘performance deficit’ and ‘knowledge deficit’ were the top two causes of medication errors because they were not specific to a particular situation. The terms may be linked to a variety of situations, and this increased the number of times they were used to integrate information from different studies. ‘Communication systems between health care practitioners’ may be linked to different forms of communication and was the top contributing factor for medication errors.
The information in the database after integration was not specific enough. Since the role of the database is to aid users to prevent mediation errors and ADEs, such categories limit the database’s usefulness. Such categories, for example ‘communication’, suggest a variety of solutions such as the need for computerized systems, use of formal verbal communications or other solutions targeting communication [Institute of Medicine, 2007]. An organization with little resources cannot afford to tackle many issues or invest in many solutions simultaneously. One possible solution is to have subcategories for these causes and contributing factors in the taxonomy. This would provide more specific information upon which to base interventions. For example, ‘communication systems between health care practitioners’ could be divided into verbal, written or online communication while ‘performance deficit’ could be divided into slips, lapse and mistakes [Reason, 1990]. This would also begin to add a human factors focus to the taxonomy and related analyses.
Implication of findings
The study demonstrates the difficulty in integrating information from studies that use different terminologies. Although it is possible to integrate the information by standardizing the terminologies, the standardized terminology may become more generic compared with the terminologies used in different studies. The generic terminology may not provide information as rich as the original terminologies used by the different studies, and this may affect how the information is interpreted. This implies that different centres that collect information on medication errors will need to adopt a standardized terminology as soon as possible. The longer the adoption is delayed, the more information is collected in different terminologies with its inherent challenges. The opportunity to review and work on these studies reinforced the authors’ opinion that taxonomies based on human factors or human error theories may improve the quality and utility of the medication error studies. Such error theories identify systemic factors as influencing the occurrence of errors [Schutz et al. 2007]. In particular, taxonomies could be improved by providing a process that identifies systemic factors and how they interact with individual human characteristics when medication errors arise.
Limitations
The study method required the interpretation of the causes and contributing factors reported by different studies as well as interpreting the categories provided by the NCC MERP Taxonomy of Medication Errors. This is a limitation in the primary coding of medication error ADEs as well. Although the study attempted to include as many relevant studies as possible, some may have been missed. The methodology involved in determining the relevance of articles depended on their title and abstract. There was a possibility that studies may have reported the causes or contributing factors of medication errors but did not mention this in their abstracts. The study also did not include the severity of the ADEs in the analysis process. The results did not reveal whether the causes and contributing factors were skewed towards very severe or near-miss medication error cases. The studies compiled have categories with different levels of detail. This would mean some studies may have similar levels of detail with the NCC MERP taxonomy while others did not, and this may have had an influence on the results of the study.
Conclusion
Although different studies used different terminologies to report causes and contributing factors of medication errors, their reports can still be integrated to a limited extent to form a single database by using a medication error taxonomy. The NCC MERP Taxonomy of Medication Errors was utilized to integrate the reported causes and contributing factors reported by different studies. Fifty seven percent of the reported causes and contributing factors were integrated using the taxonomy to form a single database, while 43% were not integrated. A taxonomy can be expanded to increase the amount of information integrated. The database indicated that the top three causes of medication errors were ‘performance deficit’, ‘knowledge deficit’ and ‘written communication’. The top three contributing factors were ‘communication systems between health care practitioners’, ‘training’ and ‘assignment or placement of a health care provider or inexperienced personnel’. The information in the database may not be sufficient to inform interventions adequately, for this reason the taxonomy should be expanded to provide more detailed information. The paper highlights the need for the adoption of a standardized terminology.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflict of interest in the preparation of this article.