
Abstract
Medication safety must be tailored to the distinctive issues in residential aged-care facilities (RACFs). The health and functional characteristics of their residents are different to those of hospital inpatients and community-dwelling older adults, and there are unique staffing and management issues. Understanding the aetiology and epidemiology of drug-related problems is vital in developing methods to improve patient safety. In this perspective review, we discuss tools that are used to quantify exposure to ‘high-risk’ medications and their evaluation in residential aged-care settings. Drug withdrawal interventions are described as a potential way to reduce adverse drug events in RACFs. Multidisciplinary professional interventions, education programs and improved communication between health professionals have been shown to improve medication safety in RACFs. Technological advances and other administrative strategies may also improve resident safety. This perspective addresses issues in medication safety facing RACFs and methods to improve the safety of medicines for their residents.
Keywords
Background
Pharmacological therapy is an integral part of modern health management and differs greatly between populations. Different population characteristics mean that safety issues and interventions arising in one setting may not apply to another. Community-dwelling people have multiple factors influencing their medications, including active commitment and responsibility of the patient. In the hospital setting there is more likely to be one set of records and less involvement of the patient. Older people, specifically those who live in residential aged-care facilities (RACFs), have reduced autonomy and exhibit different lifestyle, pharmacokinetic and pharmacodynamic characteristics to either of the aforementioned groups [Hilmer et al. 2007b]. There is very little evidence on the efficacy of medicines in older people living in RACFs. These people have a high risk of adverse drug events (ADEs) as they are likely to have multiple cormorbidities and, hence, multiple medicines, including medicines of a high-risk category [Catania, 1998; Harms and Garrard, 1998]. It is therefore paramount that drug safety, initiated by a multidisciplinary team of health professionals, be a component of patient care in RACFs.
Epidemiology
ADEs cause injuries and are the result of medication errors and adverse drug reactions (ADRs). An ADR is defined as ‘a response to a drug that is noxious and unintended and occurs at doses normally used in man for the prophylaxis, diagnosis or therapy of disease, or for modification of physiological function’ [Edwards and Aronson, 2000]. Application of this definition to residents of aged-care facilities is complicated by pharmacokinetic and pharmacodynamic changes that may mean that the doses normally used in man may not be the optimal doses in this population. An early study using retrospective reviews of incident reports reported a prevalence of 50 ADRs from a 700-bed long-term care facility over 1 year (0.60 per 100 resident-months), which was thought to be an underestimate due to the voluntary reporting system [Gurwitz et al. 1994]. In 1997, Gurwitz and colleagues undertook a comprehensive cohort study in 18 nursing homes in the USA investigating ADEs by RACF staff self-report, trained researcher record reviews and independent physician classification [Gurwitz et al. 2000]. They found high ADEs rates of 1.89 per 100 resident-months, with half of these considered preventable.
Studies investigating potentially inappropriate prescriptions (PIPs), a modifiable risk factor for ADEs, showed that 50–70% of nursing home residents had a PIP [Bergman et al. 2007; Rancourt et al. 2004]. A difficulty in assessing RACF ADR and ADE rates, and the interventions that aim to decrease them, is that many studies contain different groups of people from different clinical settings due to the infrastructure of healthcare in that particular region [Kaur et al. 2009]. A large study involving over one million individuals from Canada showed that residents of nursing homes were approximately half as likely to be exposed to those PIPs from the subgroups ‘therapies to always avoid’ and ‘those that are rarely appropriate’ (19/33 PIPs) when compared with community-dwelling older adults (2.3% exposure versus 3.3%, p < 0.001; odds ratio [OR] = 0.52; 95% confidence interval [CI] = 0.49–0.55), despite being on a higher number of distinct drugs [Lane et al. 2004]. The high prevalence of PIPs in RACFs across North America and Europe is reviewed by Ruggiero and colleagues [Ruggiero et al. 2009]. Residents are often already exposed to PIPs prior to admission to RACFs, and risk factors for PIPs appear to be polypharmacy, multiple prescribers, younger age (<80 years) and a low ratio of nurses to residents [Ruggiero et al. 2009].
Risk factors for ADEs give an alternative insight into what causes them. These differ between settings. Factors independently associated with higher risk of an ADE in a nursing home setting are being a new resident (OR = 2.8; 95% CI 1.5–5.2), taking 5–6 (OR = 2.0; 95% CI 1.2–3.2), 7–8 (OR = 2.8, 95% CI 1.7–4.7) or 9 or more (OR = 3.3, 95% CI 1.9–5.6) regularly scheduled medications, and taking an antibiotic or anti-infective (OR = 4.0, 95% CI 2.5–6.2), antipsychotic (OR = 3.2, 95% CI 2.1–4.9) or antidepressant (OR = 1.5, 95% CI 1.1–2.3). Conversely, taking nutrients or supplements is protective against ADEs (OR = 0.42, 95% CI 0.27–0.63) [Field et al. 2001]. For older people in an ambulatory setting, while polypharmacy remains a risk factor for ADEs, there is little overlap with residents of aged care facilities in the specific high-risk drug classes for ADEs [Field et al. 2004]. Amongst hospital inpatients, risk factors for ADEs appear to be features of the illness rather than the medicines [Bates et al. 1999].
Risk assessment tools
Tools to measure medication risk in older people.
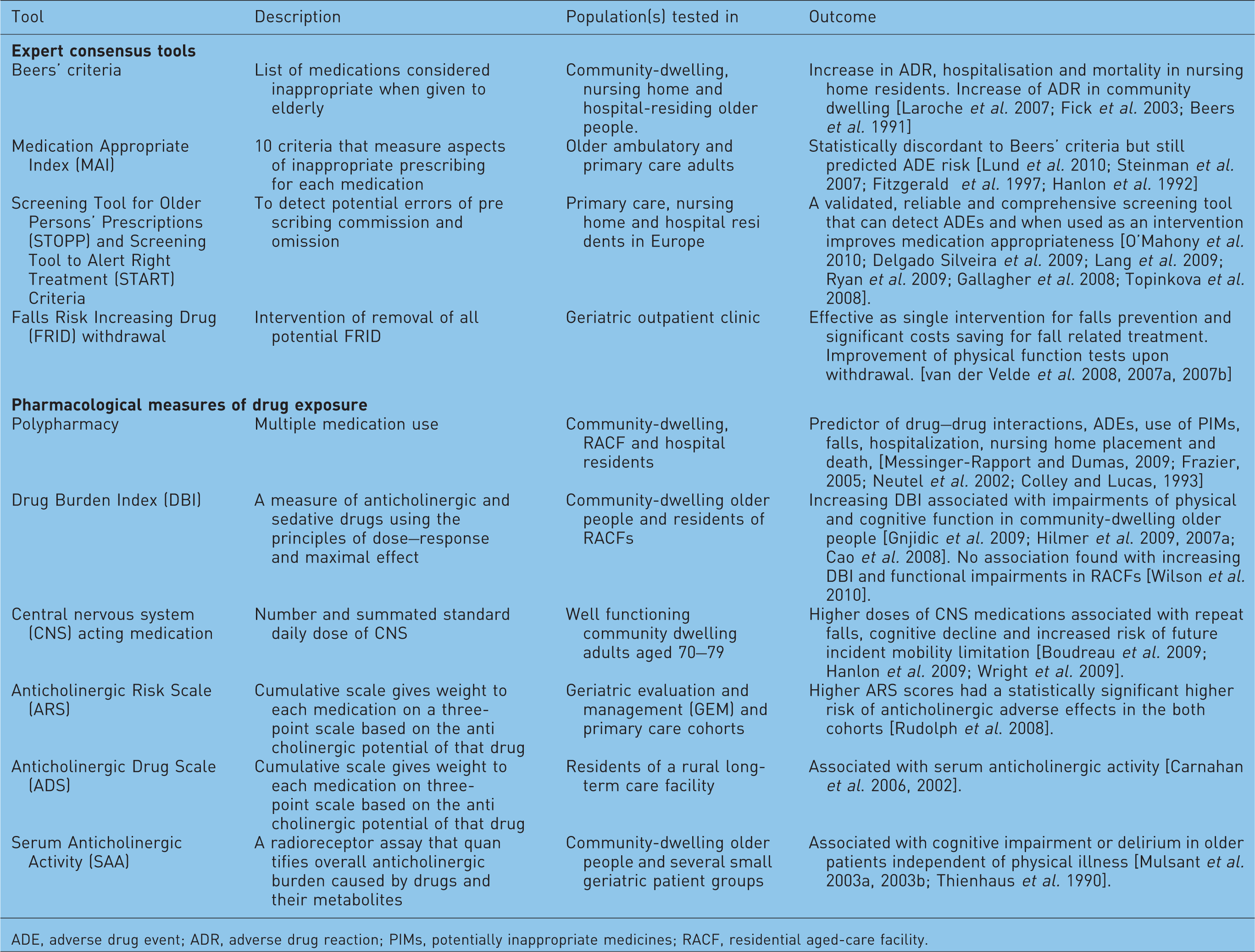
ADE, adverse drug event; ADR, adverse drug reaction; PIMs, potentially inappropriate medicines; RACF, residential aged-care facility.
In 1991 the ‘Beers’ criteria’ for determining inappropriate drug use for nursing home residents were developed by an expert consensus panel [Beers et al. 1991]. With the cessation and emergence of particular drugs, this list has been refined and updated to include 48 different medications or classes of medications, as well as 20 diseases or conditions combined with medications to be avoided in older adults (PIPs) [Fick et al. 2003]. These highly cited, updated Beers’ criteria and subsequent variations of them have formed the basis for tools that aim to improve medication safety by measuring the risk and minimizing drug related problems in older people [O'Mahony and Gallagher, 2008; Rudd et al. 2005]. The Screening Tool for Older Persons’ Prescriptions (STOPP) and the Screening Tool to Alert Right Treatment (START) criteria have been developed and validated for European countries with results that indicate they are more sensitive to detecting ADE and prescription errors than the Beers’ criteria [O’Mahony et al. 2010; Delgado Silveira et al. 2009; Lang et al. 2009; Ryan et al. 2009; Gallagher et al. 2008; Topinkova et al. 2008]. The Drug Burden Index (DBI) is another risk assessment tool that identifies high-risk medicines by pharmacologic class (anticholinergic and sedative) and calculates an individual’s cumulative exposure to these medicines, considering both the number and dose of these medicines [Hilmer et al. 2007a]. The recently developed Anticholinergic Risk Scale (ARS) is a cumulative scale that gives weight to anticholinergic medications on a three-point scale (0, no or low risk, to 3, high anticholinergic potential). The ARS score for individuals is the sum of points for their medications [Rudolph et al. 2008]. Higher ARS scores have been shown to increase the risk of anticholinergic adverse effects of older people in primary care facilities (risk ratio [RR] = 1.9; 95% CI 1.5–2.5). Alternative methods to assess anticholinergic activity include measuring the individual drug or muscarinic acetylcholine receptor in vitro; however, they contain significant clinical limitations due to the highly variable pharmacokinetics of older people and between those in different settings [Rudd et al. 2005; Tune, 2000; Tune et al. 1992; Snyder and Yamamura, 1977].
Impairment of objective measures of physical function predicts loss of independence and mortality in older people [Guralnik et al. 1994]. The association of cumulative exposure to anticholinergic and sedative medicines with impaired physical function outcome measures in community dwelling older people is well documented [Gnjidic et al. 2009; Hilmer et al. 2009, 2007a; Landi et al. 2007]. Limited research has been undertaken in RACFs; however, a recent study in people from Australian RACFs showed that while there was high exposure to medicines in these classes (>60%), there was no association of exposure to anticholinergic and sedative medicines with objective measures of function [Wilson et al. 2010].
Falls are the most important risk factor for fractures in RACFs with over 50% of residents of aged-care facilities falling every year [Kannus et al. 2005]. Regardless of setting, the majority of studies have found that polypharmacy and exposure to specific drug classes are associated with an increased risk of recurrent and single falls [Tinetti and Kumar, 2010; Leipzig et al. 1999a, 1999b]. Specifically, exposure to antipsychotics [Hien le et al. 2005], selective serotonin reuptake inhibitors [Kallin et al. 2004; Arfken et al. 2001] and hypnotics [Avidan et al. 2005; Neutel et al. 2002] are established risk factors for falls in residents of nursing homes.
Hospitalization and death are further outcome measures that can be used to assess the safety of medications in RACFs. Some studies have found that residents of nursing homes who were exposed to PIPs were at a higher risk of hospitalization and death [Lau et al. 2005; Perri et al. 2005]. This is in contrast to a recent study in nursing homes which showed no association of increasing anticholinergic exposure with mortality after adjusting for covariates [Kumpula et al. 2010]. This latest study highlights the special cohort characteristics that researchers encounter when conducting trials in the frail institutionalized elderly. Multiple cormorbidities, high mortality and dementia rates, which can limit assessments, create cohort-specific characteristics different not only to community dwelling, but other nursing home populations.
Withdrawal
Safe drug withdrawal is an obvious option to decrease the prevalence of ADEs [Iyer et al. 2008]. Nursing home residents’ behaviour has been shown not to change when haloperidol, thioridazine and lorazepam were tapered to placebo [Cohen-Mansfield et al. 1999]. Interestingly, in this study a crossover method was used whereby individuals were tapered to the reverse drug schedule, with the active drugs swapped with a placebo and vice versa, with no affect on behaviour apparent. Discontinuation of long-term antipsychotics did not affect behavioural and psychological symptoms in a recent Norwegian study of older nursing home residents with dementia [Ruths et al. 2008]. A meta-analysis on medication reviews or educational interventions in long-term care facilities demonstrated a significant decrease in the use of hypnotic (OR = 0.57; 95% CI, 0.41–0.79) but not antipsychotic (OR = 0.81; 95% CI 0.63–1.04) medicines, yet any connection with health outcomes is unknown [Nishtala et al. 2008].
Pharmacist interventions
Tools that help identify patients at high risk of ADEs are commonplace in the hospital setting yet a more comprehensive system is needed for those who move into RACFs [Bates et al. 1999]. Initial research found that retrospective drug reviews undertaken by consultant pharmacists could save United States’ nursing homes billions of dollars for the treatment of drug-related problems [Bootman et al. 1997]. The ‘Fleetwood Project’ and subsequent ‘Fleetwood Model’ were created to demonstrate and assess the value of consultant pharmacists using prospective drug reviews and interventions, improved communications between patients and professionals, patient assessment by the pharmacist and care planning for patients at high risk of medication-related problems [Harms and Garrard, 1998]. Data from nursing homes that have implemented the Fleetwood Model show they have increased clinical interaction by pharmacists, increased time spent on the planning of pharmaceutical care, superior communication among the interdisciplinary team, more efficient processes within the nursing facility pharmacy and a reduced time spent on traditional drug reviews [Bain, 2007; Lapane and Hughes, 2006a]. An electronic screening tool, linked to the prescribing system for the dispensing pharmacy identified residents at the highest risk of ADEs [Lapane and Hughes, 2004]. In the intervention study over a 1-year period, the Fleetwood Model identified 2118 activities from 4272 individuals (9.48/100 resident months). The consulting pharmacist was involved in over 80% of these activities with the reasons for the interventions being laboratory test needed (13.1%), missing information/clarification needed (13%), unnecessary drug (10.3%), product selection opportunity (10.3%), and excessive duration alert (9.1%) [Lapane and Hughes, 2006b].
While the Fleetwood Model has been successful in the USA, the nursing home infrastructure differs greatly between countries and thus models must be adapted before broader application. Variations of the Fleetwood Model have been shown to decrease the prevalence of inappropriate psychoactive medications in a Northern Ireland population when compared with those who continued with normal care (OR 0.26; 95% CI 0.14–0.49) [Patterson et al. 2010].
Pharmacist interventions can have financial benefits with the North Carolina Long-Term Care Polypharmacy Initiative that targeted patients who had received 18 prescription refills in the last 90 days [Christensen et al. 2004]. They identified a US$21.63 per resident per month drug cost saving, reduction of drug alerts and reduction of the relative risk of hospitalization for those individuals who received a retrospective review [Trygstad et al. 2009].
Pharmacist interventions, or those where a pharmacist is part of a multidisciplinary team, have been found to reduce the amount of suboptimal prescribing in older people across a variety of settings [Castelino et al. 2009]. Pharmacist-conducted medication reviews for residents of aged-care facilities significantly reduce the prescription of sedative and anticholinergic medicines [Nishtala et al. 2009]. Furthermore, a multidisciplinary case conference involving the resident’s general practitioner, a geriatrician, a pharmacist and residential care staff member has been shown to be a feasible approach to improving the medication appropriateness without altering the resident’s behaviours in high-level RACFs [Crotty et al. 2004a]. Future research on pharmacy services is required to investigate what impact the reduction of PIPs has on clinical outcomes for residents and the healthcare system overall.
Technological advances
Technological advances in medical management should provide improvements in the safety of RACF residents. In Australia, the introduction of electronic prescribing to improve patient safety has been evaluated in a RACF [Bollen et al. 2005]. Electronic prescribing terminals with information on medications, medical history and allergies were trialled in a 100-bed RACF. Medical practitioners were encouraged to prescribe using the connected electronic software. A year after the system was introduced they showed significant reduction in the use of any medications based on electronic prescribing use and a decrease in quarterly fall rate. Practices seen in intensive care suggest a likely model with computerized physician orders to decrease errors and increase legibility, electronic alerts and reminders, barcode scanning and electronic medical records, which has been shown to prevent adverse events that may not have been picked up by older technologies or protocols [Forni et al. 2010]. Owing to the complex nature of medication management, the introduction of an electronic medication system that covers only one aspect of this treatment can cause problems [Scott-Cawiezell et al. 2009]. An observational study on the use of automated medication dispensing systems or ‘robots’ found not only problems with the administration and time errors but also errors arising after the medication was handled after removal from the robot [van den Bemt et al. 2009]. Technological advances must be used as an aid to give real-time patient data and to simplify decision making for the medical team, rather than a complete approach for medical management.
Training and supervision
Supervision and continuing education of RACF staff of all disciplines is an important component in patient safety, medical management of ADRs and reducing medication errors. Institutions such as the National Prescribing Service in Australia provide ongoing education to doctors, pharmacists and nurses on medication management for residents of aged-care facilities [National Prescribing Service in Australia, 2010]. Regulation by governments and professional bodies linked to registration/licensing to practice also ensures ongoing education. Less than satisfactory levels of supervision of student nurses has been highlighted as a leading cause of medication errors or near misses [Reid-Searl et al. 2008]. One-hour teaching sessions and self-directed learning packages have proven to statistically improve registered nurses’ knowledge of medication management [Lim et al. 2010]. Technology can also assist with training and supervision. Personal digital assistants (PDAs) have been tested in some nursing homes as a medical decision support system for nurses [Johansson et al. 2009]. These PDAs that scan barcodes have the potential to be a user-friendly, medical decision support system for nurses by increasing awareness of drug–drug interactions, patient medical history, therapeutic duplication and PIPs [Johansson et al. 2010].
Communication at the interfaces of care
Residents of aged-care facilities are at high risk of medication errors when transferred between the hospital setting and the RACF due to the changing of the medical management team. Medication reconciliation by doctors, pharmacists and nurses can reduce errors associated with patient transfers [Boockvar et al. 2004; Rozich et al. 2004; Pronovost et al. 2003]. Medication-management transfer summaries from hospitals, medication reviews by pharmacists and case conferences with physicians and pharmacists have been shown to be protective against worsening pain (RR = 0.55; 95% CI 0.32–0.94) and hospital usage (emergency department visits and hospital readmissions) (RR = 0.38; 95% CI 0.15–0.99), but not against adverse drug events, falls, worsening mobility, worsening behaviours or increased confusion [Crotty et al. 2004b].
Medication management and administration within the RACF
Nursing staff in the RACF are responsible for the safe storage and administration of medicines. Nurses play an important role in determining the administration of ‘take when required’ or ‘prn’ medications such as analgesics, hypnotics and laxatives. Their responsibilities include knowing when and why to give or withhold certain high-risk medications. Nurses who treat individuals with chronic pain for example, which is prevalent in 49–84% of nursing home residents, must follow strict guidelines with patient safety the priority [Bureau of Health Professions, 2010; Won et al. 2004]. Nurses also commonly encounter problems that can affect compliance such as residents having difficulty swallowing or refusing the medication. Usage of blister packs has been shown to improve compliance of medication in community-dwelling older people and is widely used in nursing homes by facility staff to reduce errors [Doggrell, 2010; Ware et al. 1991].
Conclusions
Medication therapies and the models of care for residents of nursing homes differ greatly to those of community-dwelling older people due to the different population characteristics. Specific intervention studies are required in nursing homes to decide on the best methods of tackling the high prevalence of ADEs and ADRs. A multidisciplinary approach between professional fields with good communication and ongoing research and education are essential. Technological advances are likely to contribute to medication safety in residential aged care. An increasing level of care will translate to an increasing level of costs. Long-term care facilities and their staff are likely to bear a large burden of the expenses and workload, whereas residents will enjoy a majority of the benefit [Subramanian et al. 2007].
Footnotes
Acknowledgement
The authors acknowledge the support of the Geoff and Elaine Penney Ageing Research Unit.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that they have no conflicts of interest regarding this review.