
Abstract
Control of inflammation is indispensable for optimal oral wound healing and tissue regeneration. Several biomaterials have been used to enhance the regenerative outcomes; however, the biomaterial implantation can ensure an immune-inflammatory response. The interface between the cells and the biomaterial surface plays a critical role in determining the success of soft and hard tissue regeneration. The initial inflammatory response upon biomaterial implantation helps in tissue repair and regeneration, however, persistant inflammation impairs the wound healing response. The cells interact with the biomaterials through extracellular matrix proteins leading to protein adsorption followed by recruitment, attachment, migration, and proliferation of several immune-inflammatory cells. Physical nanotopography of biomaterials, such as surface proteins, roughness, and porosity, is crucial for driving cellular attachment and migration. Similarly, modification of scaffold surface chemistry by adapting hydrophilicity, surface charge, surface coatings, can down-regulate the initiation of pro-inflammatory cascades. Besides, functionalization of scaffold surfaces with active biological molecules can down-regulate pro-inflammatory and pro-resorptive mediators’ release as well as actively up-regulate anti-inflammatory markers. This review encompasses various strategies for the optimization of physical, chemical, and biological properties of biomaterial and the underlying mechanisms to modulate the immune-inflammatory response, thereby, promoting the tissue integration and subsequent soft and hard tissue regeneration potential of the administered biomaterial.
Introduction
Healing of oral wound entails an intricate sequence of various biological processes. Inflammation is a key factor influencing the outcome of several dental procedures including regenerative procedures and osseointegration of dental implants; therefore, immune-inflammatory modulation has been recognized as the major challenge as well as a potential therapeutic tool. All biomaterials, when implanted in vivo, elicit cellular, and tissue responses. These responses vary from inflammatory and wound healing responses, foreign body reactions (FBR), to fibrous encapsulation of the implanted materials. The immune cells, neutrophils, and macrophages in particular, are the first to respond to tissue trauma or foreign aggression and to the implantation of biomaterials, natural, or synthetic. 1 These cells carry out both phagocytic and signaling roles in the inflammatory phase following biomaterial implantation which determines the establishment of chronic inflammation, fibrosis, integration, and consequent resolution of inflammation. Other innate immune system cells including dendritic cells (DC), mast cells, natural killer cells, may also serve an immunomodulatory role. DC are antigen presenting cells which make a bridge between the innate and adaptive immune responses. Since the over activation of immune cells upon biomaterial implantation is an undesirable outcome, 2 it is mandatory to understand their potential response to the scaffold in order to design the biomaterials such that they do not trigger sustained proinflammatory reactions. Biomaterial-based modulation of the immune-inflammatory axis can significantly ameliorate the outcomes of the tissue engineering therapies. The use of biomaterials, with and without the incorporation of pharmacological agents or bioactive molecules, has revolutionized the oral wound healing and tissue regeneration process. 3 Oral surgeries employ different surgical techniques, often including implantation of various types of biomaterials including bone graft and/or bone substitutes, guided tissue regeneration, growth, and differentiation factors, enamel matrix proteins, or various combinations thereof, to achieve tissue repair or regeneration. 4 The trend has recently been shifted from biocompatible “immune-evasive” biomaterials to “immune-interactive” materials that modulate the inflammatory response, thereby, supporting biomaterial integration as well as improving healing and tissue regeneration. 5
The aim of this review is to determine the physical, chemical, and biological properties of the biomaterials that can be optimized for the modulation of inflammatory-immune response to improve the soft tissue and hard tissue repair and regeneration.
Physical modification of biomaterials to modulate inflammation
Role of protein adsorption
The protein adsorption on the scaffold surface can be mainly modified and controlled through electrostatic interactions, covalent linkages, nucleic acid hybridization, and chemosorption.6,7 Protein adsorption on the biomaterial surface is the key determinant of the subsequent processes of cell growth, differentiation, and extracellular matrix (ECM) formation. Regardless of the type of biomaterial, the first event that takes place at the material-cell/tissue interface is wetting followed by rapid protein adsorption to its surface (fibronectin, albumin, fibrinogen, immunoglobulins (IgG), complement C3 from blood and bone marrow, vitronectin). In Phase II, it is crucial for cells to adhere to the protein film before the bacteria (“the race for the surface”). In the Phase III, non-specific cellular adhesion occurs through ECM anchoring proteins. The biomaterial-cell interface is complex. Local growth factors and intercellular cytokines secretion, cell proliferation, and differentiation are induced at Phase IV 8 (Figure 1).

Local reactions to biomaterial surface by time. Phase I: surface wetting and adsorption of molecules (proteins) mainly derived from blood. Phase II: battle between local cells or bacteria for adhesion onto the surface. Phase III: formation of extracellular matrix (ECM) and focal adhesion contacts. Phase IV: the cells started to proliferate and differentiate hence tissue is re-modeled.
Successful application of biomaterials is restricted by the inflammatory response elicited after their implantation. Early adsorption of proteins on the biomaterial surface triggers the activation of the innate and acquired immunity. 9 Macrophages are considered as key effectors in this inflammatory response known as FBR. Their direct contact with the biomaterial surface can induce the secretion of chemokines and pro-inflammatory cytokines such as interleukin-1β (IL-1β) and Tumor necrosis factor-α (TNF-α) (Figure 2). Prolonged unresolved inflammation leads to the fusion of macrophages into foreign body giant cells (FBGCs) in an attempt to phagocytose the implanted biomaterial causing recruitment of fibroblasts for subsequent fibrous encapsulation, isolation, and premature scaffold failure. 10
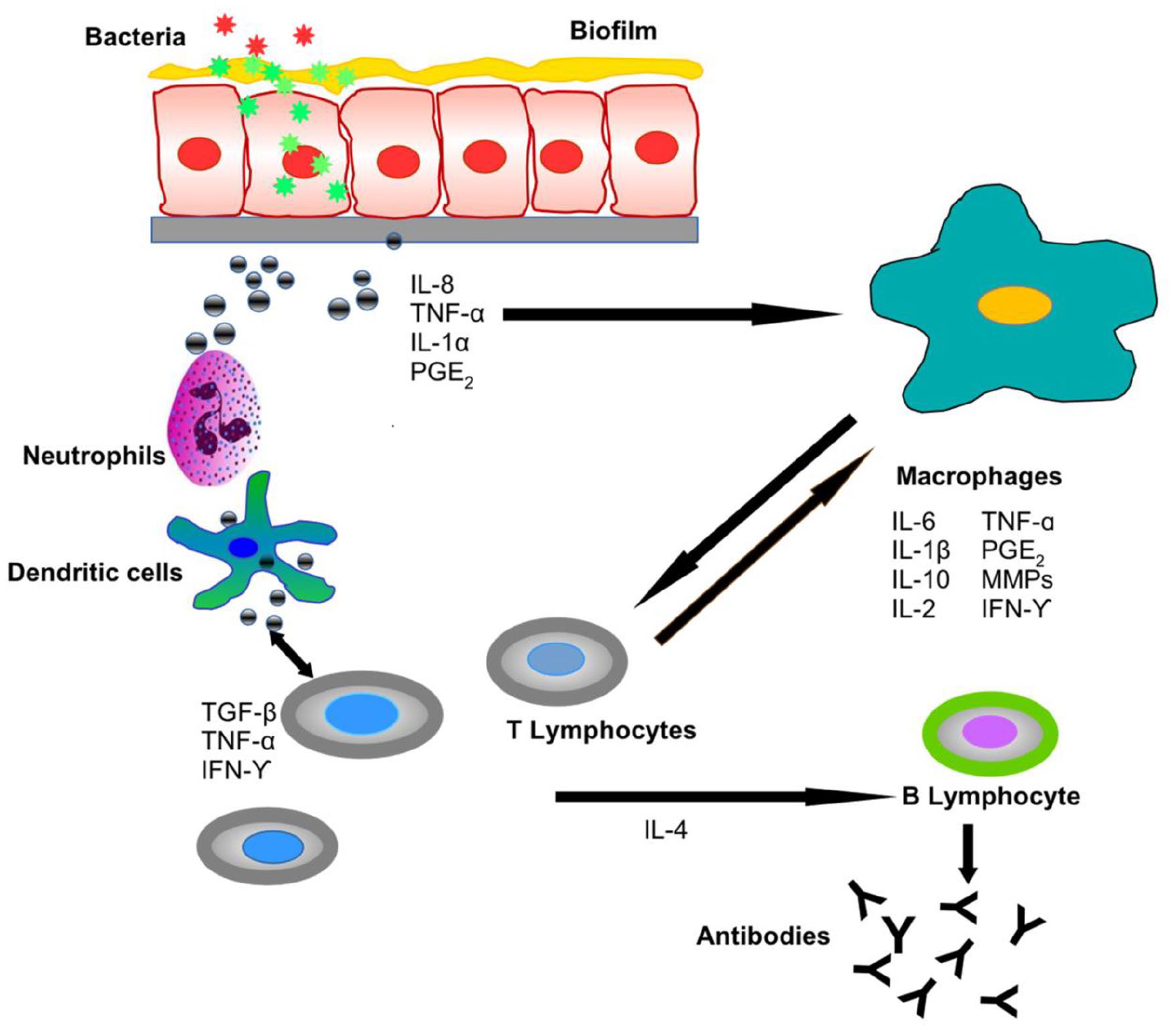
The implantation of a biomedical implant triggers innate and adaptive host inflammatory responses. Periodontal pathogens in the biofilm activate a host immune response that leads to the production of several cytokines (represented by gray spheres) from oral epithelial cells and immune cells. Macrophages and neutrophils play an important role in the initial phase of inflammation, followed by the adaptive immune response orchestrated by lymphocytes.
Initially, blood proteins, such as albumin, fibrinogen, fibronectin, immunoglobulins, adsorb on the biomaterial surface directly after its surgical implantation. The composition of these adsorbed proteins and the conformational changes that these proteins undergo upon adsorption dictate opsonization of biomaterials initiating the coagulation and complement cascades, thus, triggering the inflammatory responses. 9 Adsorbed fibrinogen has been reported to promote macrophage activation leading to increased production of TNF-α, whereas the polymerization product fibrin exerts an anti-inflammatory effect by preventing TNF-α production. Furthermore, the presence of fibrinogen is considered an important regulator for macrophage phenotype switch during the inflammatory responses through their interaction with Toll-like receptor 4 (TLR-4) and secretion of anti-inflammatory mediators like interleukin-10 (IL-10) and transforming growth factor β (TGF-β). 11 Surprisingly, most adsorbed blood proteins have been observed to support initial monocyte adhesion with the exception of vitronectin that causes FBGC formation. 12 Therefore, modification of ECM proteins adsorbed on the biomaterial surface in order to mimic the surface proteomics of natural tissues can improve biomaterial-cell integration and modulate the consequent inflammatory response. For instance, the incorporation of cell adhesion peptide, arginine-glycine-aspartic acid (RGD), present in many ECM proteins, into Poly(ethylene glycol) (PEG) hydrogels as coatings on implantable devices has shown promise in tissue engineering applications by reducing the exaggerated inflammatory response or FBR. 13
Role of surface topography
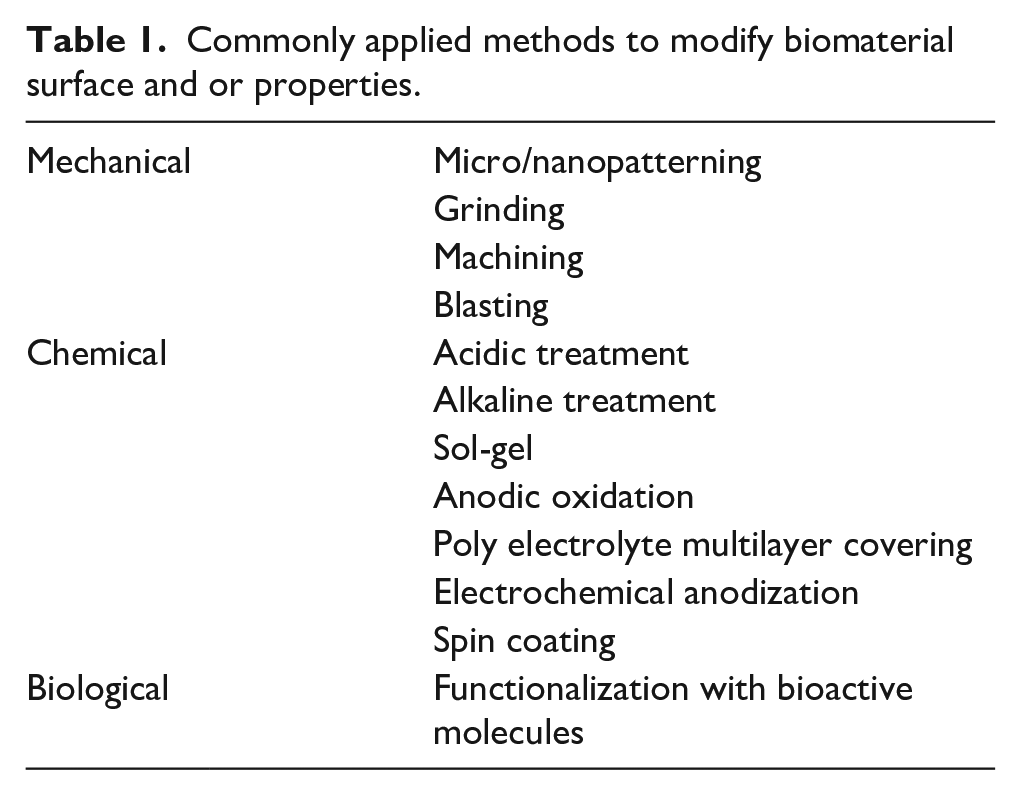
Alveolar bone is a natural nanostructure consisting of nano-hydroxyapatites periodically distributed in self-assembled collagen fibrils. Topographical properties of biomaterials, such as macroporosity and surface micro or nanostructures, can mimic the natural structure of the tissue and modulate the local microenvironment, subsequently, dictating the host response and influencing the tissue healing cascades. 14 Due to these optimizable characteristics and biomimicking properties, nanotopography can be a valuable tool for osteoimmunomodulation in order to promote bone regeneration or bone healing. Thus, biomaterial surface properties such as topographical features, stiffness, can be modified through several techniques (Table 1) to improve biomaterial–cell interaction and modulate host inflammatory response to enhance biomaterial integration and regenerative ability.
Commonly applied methods to modify biomaterial surface and or properties.
Surface topographies can either be ordered or unordered. In order to create ordered topographical patterns, lithographic techniques such as photolithography, electron beam lithography, soft-lithography, colloidal lithography, scanning probe, and electrospinning are mostly used. Phase separation, chemical etching, self assembly, moulding, and electrospinning can be used to develop unordered surface topography in biomaterials.15–17
Studies reveal that nanoscale features influence and regulate the morphological and phenotypical properties such as filopodial sensing, improve cell spreading adhesion and growth of various cell types, for instance, mesenchymal stem cells (MSC). 18 Interestingly, osteoprogenitor cell differentiation can be directed toward an osteoblastic phenotype via tuning the nanotopographical size down to 10 nm. 19 It has been shown that topography can be used to control human monocyte attachment and macrophage differentiation. Moreover, micropatterns such as micropillars (5–10 μm in diameter) play a dominant role in driving macrophage attachment. Optimizing the micropillar size and density is instrumental in the modulation of cell phenotype from pro to anti-inflammatory states. It has also been demonstrated that nanohydroxyapatite (nHAP) enhanced cell proliferation and osteogenic differentiation of bone marrow stem cells but decreased degradation rate of the scaffold. 20
Surface roughness and topography of the biomaterials is influenced by hydrophobicity and plays a major role in bacterial attachment. Nano- and microstructures, such as tubes, fibers, grooves, pillars, colloids, and pits, significantly increase the surface area, which may create more effective bactericidal activity than flat surfaces. 21
Hydroxyapatite (HA) coatings used in dental applications, due to their biomimetic nature, have osteoconductive effects and facilitate the attachment and differentiation of osteoblasts (OB) and suppression of osteoclastic activity (OC). OB attachment and differentiation were observed to be higher on microrough HA surfaces (surface roughness (Ra) = 2 mm) than on smoother topographies (Ra = 1 mm). At contrary, greater OC marker tartrate-resistant acid phosphatase activity has been shown on smoother than on micro-rough surfaces. 22
Similarly, the inclusion of bioactive glass (BG) nanoparticles, another biomaterial with osteoconductive and osteoinductive properties, in the gelatin-chitosan-bioactive nanoceramic composite scaffolds significantly enhanced the bone regenerative capacity. 23 Additionally, adjusting the scale of nanotopography (68 nm) has shown appreciable decrease in the expression of pro-inflammatory cytokines and OC. 24
Modification in surface roughness and topography of titanium (Ti) implants influences greatly the survival, adhesion, and secretion of macrophages. 25 For instance, nanoscale roughness resulted in a greater downregulation of the inflammatory/immune response and a significantly improved significantly greater osteogenic differentiation in comparison to the micro-roughened surface. 26 In addition, the introduction of parallel gratings with widths ranging from micron to sub-micron scales (250 nm–2 µm) on implant affects macrophage behavior suggesting that nanoscale structure of implant surfaces can influence bone implant interactions via M1/M2 polarization. 27
The important role of scaffold specific surface area in initial cell adhesion, pore size is critical in cell attachment, migration, and proliferation and cannot be undermined as exhibited by improved cell migration in scaffolds with pores above 300 μm. Additionally, larger pores reduce cell aggregations developed at the scaffold margins. Scaffolds with a mean pore size of 325 μm are proposed as optimal for bone tissue engineering. 28
Besides other factors, surface patterns are also one of the key determinants of surface characteristics and consequent biological behavior of cells at the cell-biomaterial interface. Interestingly, nanostructured ceria (nano-CeO2) of different shapes (nanorod, nanocube, and nano-octahedron) developed on Ti surfaces have demonstrated anti-inflammatory and antibacterial effects in vitro and in vivo. The hydrothermally prepared ceria possess specific crystal planes that promote intrinsic catalysis. In vivo, the different shapes of nano-CeO2 on Ti, implanted subcutaneously in rats, reduced the gene expression of TNF-α, IL-6, and IL-1β in the tissues surrounding the implant. All three types of CeO2-modified Ti showed similar antibacterial properties, whereas nano-octahedron CeO2 showed the strongest anti-inflammatory effect. 29
In this context, microgrooves are the most used pattern to control cell behavior. For example, the polarization of the macrophages on a polydimethylsiloxane surface with 20 and 50 μm grooves has been investigated. It was reported that elongation of cells induced release of cytokines (IL-4, IL-13) and polarized macrophage toward M2-like phenotype together suggesting that cell shape plays a role in the modulation of phenotypic polarization. 30 In another study, Ti surfaces with 400–500 nm wide grooves triggered the highest elongation and also drove macrophages toward an anti-inflammatory, pro-healing phenotype. 31 Similar effects of microtopography on reduction of pro-inflammatory polarization have been observed in Ti or its alloys and with other materials such as zinc, zirconia polycrystal, shape memory PCL-PEG substrates and polyethylene films, and silicon.32–34 Such anti-inflammatory effect associated with material topography has also been demonstrated on nanostructured biomaterials. Interestingly, nanocrystalline hydroxyapatite and nanocrystalline silicon substituted hydroxyapatite decreased the M1 population and increased macrophage polarization toward an M2 phenotype. 35 Nanostructures created on Ti by anodization with a size of 100 nm favor an M1 macrophage, whereas 30 nm favor an M2 polarization. 36
On the other hand, several studies revealed that macrophages can be polarized into both pro-and anti-inflammatory phenotypes, on microstructured polyvinylidene fluoride substrates. For example, the use of medical and dental grade implant materials with surface roughness varying between 0.5 and 3.5 µm differentially enhanced anti-inflammatory activation of primary murine macrophages compared to smooth surfaces, while also upregulating the pro-inflammatory markers as well.37–39 These conflicting results may be a due to the diverse cell types (primary cells vs cell lines, species, cell source) and culture conditions used in these studies.
In addition to surface topography and wettability, stiffness has also been shown to modulate neutrophil activation. It has been observed that neutrophil migration speed was decreased on stiff (100 kPa) polyacrylamide hydrogel compared to that on a soft hydrogel (5 kPa). Thus, it can be suggested that NETosis, which is defined as the extrusion of neutrophilic chromatin together with antibacterial proteins originating from the neutrophil granules to kill extracellular pathogens, can also be regulated by stiffness via modulation of their migration rate. 40
Regarding stiffness of materials, contradictory data can be found about the macrophage activation. For instance, a study on collagen-coated polyacrylamide gels has demonstrated that increasing stiffness increased pro-inflammatory macrophage polarization. 41 However, in a similar study, the use of polyacrylamide hydrogels showed that increased stiffness enhances M2 polarization by modulating reactive oxygen species (ROS)-mediated NF-κB signaling. 42 Mechanistically, Wnt/β-catenin signaling 43 and MAPK signaling44,45 have also shown to play a role in macrophage responses to high-stiffness biomaterials.
Hierarchical macro-pore/nanosurface implant surfaces decreased the levels of inflammatory gene expression while enhancing the anti-inflammatory gene expression and inducing a macrophage M2 polarization. When culturing bone marrow MSC in the conditioned media from these macrophages, osteogenic differentiation was observed. 46 Similarly, DC cultured on 3D micropatterns revealed significantly higher expression of MHC-II compared to the DC cultured on the flat substrates indicating the role of substrate dimensionality in regulating their adhesive and immunomodulatory properties. 47
Likewise, nanonets (NN) and nanopores (NP) were developed by electrochemical anodization of Ti surfaces and the comparison of these three surfaces (NN, NP, and unmodified Ti) showed that surface roughness was higher in NN (pore size of 77.7 ± 0.7 × 47.4 ± 0.5) compared to NP and unmodified Ti, while, hydrophilicity was greater for NP in comparison to NN and Ti. Also, NN and Ti induced oriented alignment of MSC and oral fibroblasts and lead to osteogenic differentiation of MSC and upregulated alkaline phosphatase (ALP) activity and collagen deposition. Moreover, such modification has demonstrated a great potential for dental implant abutments to improve both soft and hard tissue integration. 48
Chemical modification of biomaterials to modulate inflammation
Role of surface chemistry
Covalent immobilization, alkaline hydrolysis, wet chemical methods such as etching, chemisorption, chemical vapor deposition, plasma treatments are generally employed for the transformation of biomaterials’ surface chemistry.24,49 For instance, modification of the surface chemistry with amine or acrylic acid has shown to significantly modulate the osteoimmune environment including osteogenic, angiogenic, and fibrogenic factors as well as the immune-inflammatory response. Furthermore, surface functionalization with carboxyl acid enhanced the osteogenic differentiation of bone marrow stromal cells. 24 Similarly, intrafibrillarly mineralized collagen scaffold, with a similar nanotopography and surface chemistry as that of natural mineralized collagen, has shown to direct human periodontal ligament stem cells toward osteoblastic differentiation have exhibited improvement in bone tissue regeneration. Recently, fabrication of 3D architectures or the chemical modifications of biopolymeric materials have shown to promote osteogenesis and cementogenesis. 50 Another approach for modification of biomaterial surface chemistry to mimic bone ECM, by coating synthetic dicalcium phosphate bioceramics with bone ECM proteins, has shown modulation of the host immune reactions and improvement in their regenerative performance. 51
A study involving periodontal defect model of beagle dogs demonstrated the surface functionalization of chitosan nanoparticles with ε-aminocaproic acid incorporated fibrin resulted in significant cementum formation on the exposed root dentin compared to fibrin-only and enamel matrix derivative (EMD) which is often used clinically to achieve periodontal regeneration. 52
In vivo, the tissue healing response to Jellagen®-3D scaffold composed of jellyfish collagen, with an average pore size of 100 µm and crosslinked with various chemical agents to improve mechanical properties has been compared to the porcine pericardium matrices. The calvarial implantation of the former scaffold showed significantly improved bone formation in comparison to the control group and significantly higher numbers of anti-inflammatory macrophages at the implantation site. 53
Besides macrophages, in the context of DC activation, the effect of various biomaterial surfaces on DC phenotype showed that poly(D,L-lactic-co-glycolic acid) (PLGA) as well as chitosan films induced DC maturation, whereas, hyaluronic acid inhibited formation of mature DC phenotype. Similar to chitosan and PLGA, alginate film promoted proinflammatory cytokine release by DCs. 54 Chitosan has been widely used in wound healing and hard tissue engineering. Especially, high molecular weight hyaluronic acid and chitosan are reported to have intrinsic anti-inflammatory properties due to their ROS-scavenging properties. 55
Magnesium-based alloys have been tested for osseous regeneration but they are prone to undesirably rapid degradation owing to their high corrosion rate, leading to infection in vivo and implant failure. A study demonstrated the modification of a magnesium alloy with graphene nanoparticles (0.18 and 0.50 wt%) showed compressive properties comparable to that of the native cancelous bone (elastic modulus 6 GPa), reduced their degradation rate by four-fold and improved their antibacterial activity by five-fold. In vitro, human mesenchymal stromal cells showed significantly superior cytocompatibility osteogenic potential in graphene-modified magnesium alloy compared to non-graphene-modified alloy implants. 56
Role of hydrophilicity
Surface modification of biomaterials, carried out by employing hydrophilic functional groups, is a key chemical phenomenon, enhancing biomaterials’ accessibility to biological molecules. There are several methods to make the surfaces of biomaterials hydrophilic such as plasma modification or hydrolysis. 57 For instance, OB cultured on surface-modified hydrophilic Ti showed an increased level of TGF-β/BMP signaling compared to an unmodified hydrophobic surface. 58 Hydrophilicity of a material also affects the macrophage activity. Increased levels of anti-inflammatory IL-10 and reduced levels of pro-inflammatory cytokines TNF-α, IL-1α, IL-1β, and chemokines CCL-2 have been observed in macrophages cultured on surface-modified hydrophilic Ti. 59 Similarly, polarization into the M2 phenotype was observed in primary murine macrophages cultured on hydrophilic Ti, subsequently, improving OB activity. 37
Noteworthy, Ti implants of varying wettability (rough, and rough-hydrophilic) placed in the femur of mice demonstrated that increased surface roughness and wettability can lead to polarization of the adaptive immune response toward a Th2, pro-wound healing phenotype, thereby, promoting resolution of inflammation. Moreover, an increased stem cell recruitment was seen around rough hydrophilic implants. 60
Optimization of biomaterial surface properties such as roughness and hydrophilicity can activate anti-inflammatory phenotype of macrophages. The regulation of Wnt signaling in macrophages during pro- and anti-inflammatory polarization in response to smooth, rough, and rough-hydrophilic Ti surfaces was studied in macrophage-ablated (MaFIA) mice where Wnt signaling was significantly attenuated compared to the untreated controls. Wnt ligand mRNA expression was increased in a surface modification-dependent manner in macrophages isolated from the surface of Ti implanted in C57Bl/6 mice. Loss of macrophage-derived Wnt also compromised MSC and T-cells recruitment to Ti implants in vivo. Furthermore, inhibition of integrin signaling reduced surface-dependent upregulation of Wnt genes suggesting that Wnt signaling regulates macrophage response to biomaterials and it modulates inflammation and healing responses. 60
The surface hydrophilicity or wettability is one of the most major surface properties that modulates anti-inflammatory macrophage activation via increased surface energy. Interestingly, the combination of surface roughness and hydrophilicity has shown to remarkably enhance the release of anti-inflammatory markers.37,38 The mechanism of the effects of hydrophilicity has been explained by the conformational adsorption of fibronectin and fibrinogen though integrin signaling and consequent PI3K and NF-κB activation. 61
Macrophages and neutrophils also respond differentially to changes in surface roughness and hydrophilicity of Ti implant surfaces with neutrophils secreting higher levels of pro-inflammatory cytokines and causing NETosis on smooth/rough hydrophobic surfaces, compared to those on rough-hydrophilic surfaces. 60
Hydrophobic polymers like poly(lactic-co-glycolic acid) (PLGA) have shown to induce mature DC phenotypes via integrin-β2 receptors.62,63 On the other hand, hydrophilic hyaluronic acid surfaces induce immature DC phenotypes. 64 This can be due to a lower ability of protein adsorption on hydrophilic surfaces and their distinct surface energy profiles which permits adhesion and maturation of DCs.
A study, carried out in femoral bone defect in mice, demonstrated that surface modifications applied to Ti implants to increase their surface roughness and wettability can polarize the adaptive immune response toward a pro-wound healing phenotype Th2, speeding up resolution of inflammation and increased MSC recruitment around rough hydrophilic implants with macrophage ablated clodronate liposomes. 38
Interestingly, several commercial implants have been compared with Ti alloy dental implants that were specifically characterized for surface topography, chemistry, and hydrophilicity. Macrophages on hydrophobic implants produced the highest levels of pro-inflammatory mediators in vitro. The hydrophilic implants upregulated the release of anti-inflammatory mediators. Similarly, pro-inflammatory CD80hi macrophages predominated in vivo in the vicinity of hydrophobic implants, and M2 CD206+ macrophages predominated in the tissue surrounding the hydrophilic implants. 65
Role of surface charge
Surface charge modification of biomaterials greatly affects adsorption of biological molecules, cell adhesion and mineralization notably at the bone-implant interface, consequently, influencing osteogenesis. 66 In case of Ti implants, TiO2 layer on the surface typically has a slight negative charge. Therefore, efforts have been recently directed toward the optimization of the surface-charge to enhance osseointegration of a Ti dental implants. 67 Additionally, positively or negatively charged surfaces maybe more hydrophilic in comparison to neutral surfaces. Several techniques are used to modify the surface charge density, for instance, chemical etching, surface heat treatment, electrical stimulation, sandblasting, and grafting of bioactive materials.67,68 The surface charge can also be modified by controlling surface porosity and texture, or by modifying the electrolyte composition, consequently, modifying the protein adsorption on the biomaterial surface. 69
A study involving acrylamide based biomaterials with anionic poly(acrylic acid) and cationic poly(dimethylaminopropylacrylamide) functional groups revealed that the anionic substrate upregulated IL-10 levels and downregulated IL-8 secretion. At contrary, the cationic substrate inhibited IL-10 and IL-1RA production, which are critical for osteoblast maturation. 70
Notably, MSCs attachment and osteogenic differentiation has also been shown to enhance significantly by rendering the biomaterial surface more positively charged through conjugation of charged poly(amidoamine) to alginate-based hydrogels. 66 Also, pH-induced surface charge transformation has demonstrated improved antibacterial activities of gold nanoparticles (AuNPs) decorated with carboxyl betaine groups. 71
Role of surface coatings and delivery systems
Several biomaterial surface transformation strategies such as soft-lithography, photolithography, X-ray lithography, sol-gel method, physical/chemical vapor deposition, electrodeposition, thermal spraying, plasma spraying, electroplating, microarc oxidation, layer by layer electrostatic self assembly, grafting, immobilization have been used to coat the biomaterial surfaces.72–74 Coprecipitation, sputtering, micro/nanoemulsion, laser ablation, mechanical milling, electrospinning, and vapor deposition are the main techniques used for the synthesis of micro/nano delivery systems and have shown promise in the regenerative medicine.75–79
Several controlled-drug release carriers such as micro/nanoparticles, liposomes, exosomes, or surface coatings on biomaterial scaffolds or implants have been developed and optimized to modulate inflammation, control infection, and eventually, promote tissue regeneration (Figure 3).

Schematic presentation of various surface coatings for dental implants and controlled-drug release systems for immune-inflammatory modulation.
For instance, nanoparticles can be coated on dental implants for the regeneration of alveolar bone. Silver, gold, hydroxyapatite, titanium oxide (TiO2), and zirconia-based nanoparticles are also widely used in dental applications including oral surgery, imaging, endodontics, periodontics, and tissue engineering. Their high surface-volume ratio, mechanical, and potential antibacterial properties make them effective vehicles for dental applications. 80
Regarding microcarriers, porous polyetheretherketone (PEEK) microcarriers coated with mineralized extracellular matrix promoted cell proliferation and osteogenic activity. Additionally, such porous microcarriers exhibited excellent bone regeneration in a rat calvarial defect repair model in vivo, suggesting a potential application in bone tissue engineering. 81
Furthermore, chitosan-based gold nanoparticles (AuNPs) composite films showed high antibacterial activity against antibiotic-resistant strains of Pseudomonas aeruginosa and Staphylococcus aureus. 82 Interestingly, spherical AuNPs were shown to be formed inside dentinal tubules by an in situ photothermal reduction that can be used as a contrast agent for imaging. Chitosan AuNPs conjugated anti-inflammatory molecules peroxisome proliferator activated receptor gamma (PPARγ) on Ti implant surface were used to reduce implant-induced inflammation and to induce bone mineralization of MC-3T3E1 osteoblast-like cells. 83
Similarly, optimized silver nanoparticles AgNP-coated collagen membrane exhibited excellent anti-bacterial effects against Staphylococcus aureus and Pseudomonas aeruginosa, significant anti-inflammatory effects reflected by the down-regulation of IL-6 and TNF-α. Moreover, they induced osteogenic differentiation of MSC and promoted bone regeneration, thus, highlighting their potential application in preventing inflammation and infection after bone graft introduction in alveolar ridge reconstruction. 84
A study involving antibacterial silver nanoparticle-loaded TiO2 nanotubes (Ag TiO2-NTs), prepared on the Ti surfaces through electrochemical anodization, showed suppression of inflammation and improved osteogenesis in vitro and in vivo in comparison to TiO2-NTs and polished Ti surfaces. Strikingly, Ag TiO2-NTs induced macrophage phenotype switch to the pro-healing M2 by inhibiting PI3K/Akt, decreasing GLUT1 expression, and triggering autophagy. 85 Likewise, a study on chitosan sponge coated with 50% TiO2 nanoparticles exhibited enhanced bone regeneration potential and osteogenic differentiation of MSC. 86
In vivo, the modified Ti implant with peptide LL-37-loaded silk fibroin nanoparticles immobilized on the Ti surface promoted MSC and macrophage recruitment to injury sites and positively modulated the inflammatory response. Moreover, improved bone formation was observed around the modified Ti implant 28 days post-operatively. 87
Notably, NP coatings on Ti surfaces have demonstrated antibacterial effect that helps prevent peri-implantitis and can promote osteogenic integration. NPs can stimulate periodontal ligament cells and can promote periodontal regeneration. Moreover, addition of organic NPs to controlled drug delivery systems cause apoptosis of tumor cells, preventing their metastasis. However, further in vivo and in situ studies are necessary to establish their effectiveness in clinical application. 88 Even herbal substances such as asiaticoside loaded sulfobutylether β-CD/chitosan NPs have been shown to promote collagen I synthesis and osteogenic differentiation in human periodontal ligament cells. 89
Interestingly, in mouse bone marrow-derived macrophages, superparamagnetic iron oxide nanoparticles (SPIONs) released IL-1β in a size-dependent manner, with the smaller SPIONs (30 nm) triggering the greatest IL-1β secretion compared to the two larger SPIONs (80 and 120 nm). 90 Likewise, a study involving PEGylated poly(ethylene glycol) coated magnetic iron oxide-silica nanocomposites of various sizes (20, 40, 100, and 200 nm) tested in fibroblasts and macrophages demonstrated that sizes smaller than 100 nm and concentrations <100 μg/mL induced low cytotoxicity and inflammatory response. Such size based trends can be useful in designing novel drug carrier systems. 91
The modification of physicochemical properties of dental implants through coatings composed of silica, magnesium, graphene, dopamine, and bioactive molecules has shown to accelerate bone-to-implant response. Modified zirconia surfaces also demonstrated faster osseointegration than that with untreated surfaces. 92
A study comparing chitosan-coated calcium hydroxide-loaded microcapsules to Bio-oss and pure Ca(OH)2 powder in a mandibular bone defect in rabbits significantly downregulated inflammation, expression of IL-6 and TNF-α, and improved osteogenesis. 93
Exosomes are important secretory factors for MSC therapeutic effects. MSC exosomes have great potential in regenerative medicine. Exosomes have been shown to promote angiogenesis, regulate migration, proliferation, and differentiation of the cells making them promising vectors for dental tissue regeneration. Furthermore, a dose-effect relationship between exosomes and osteogenic potential of MSC has been demonstrated. 76 Dental pulp stem cells regenerate a dentin/pulp-like complex under appropriate growth conditions. Importantly, their exosomes have shown to have odontogenic, neurogenic, and angiogenic properties.
In addition to regenerative capacities, stem cells-derived exosomes exert therapeutic effects due to their anti-inflammatory and immunomodulatory properties. Importantly, exosome administration rarely induces immune reactions because exosomes do not contain MHC class I or II molecules. 94 Previous studies indicated that the activation of NF-κB and p38 MAPK signaling is responsible for persistent periodontal inflammation. 95 Interestingly, recent data suggests that stem cells-derived exosomes contain miRNAs such as miR-223 96 and miR-182 97 that are active players in modulating the macrophage phenotype. Also, it has been demonstrated that dental pulp stem cell derived exosomes incorporated into chitosan hydrogel can accelerate the healing of alveolar bone and periodontal endothelium in mice with periodontitis. It was further revealed that miRNA 1246 mediated the effects of exosomes by facilitating macrophages to convert from a pro-inflammatory type to an anti-inflammatory type. 98
Apart from downregulating inflammation, a recent study showed effective antibacterial effects of a novel antimicrobial peptide Nal-P-113 loaded poly (ethylene glycol) combined chitosan NPs (size 216.2 ± 1.6 nm, drug encapsulation efficiency 89.33 ± 1.67% (w/w)) against periodontal pathogens including Fusobacterium nucleatum, Streptococcus gordonii, and Porphyromonas gingivalis with a MIC of 23, 6, and 31 µg/mL, respectively. 99 The antibiotic doxycyclin loaded chitosan/carboxymethyl chitosan nanoparticles showed antibacterial effect against P. gingivalis and downregulated NLRP3 inflammasome and IL-1β in human gingival fibroblasts. 100 Similarly, doxycyclin containing Lecitin-based liposomes coated with quaternary ammonium N,N,N trimethyl chitosan showed antibacterial action against P. gingivalis and Prevotella intermedia and reduced inflammatory cell infiltrate, osteoclastic activity and periodontal pocket depth in an experimental periodontitis rat model 101 .
Recently, the focus regarding scaffolds for periodontal regeneration has been largely shifted toward composite scaffolds composed of 3D scaffolds loaded with nanosystems that can ensure efficient and controlled drug release and desirable mechanical properties. 102
In this regard, novel thermosensitive injectable hydrogels composed of chitosan, β-sodium glycerophosphate and gelatin with controlled release of aspirin and erythropoietin, 103 and statins 104 exerted anti-inflammatory and tissue regenerative effects in vitro and in vivo. As the incorporation of MSC into the biomaterial scaffolds has shown to improve the biomaterial-tissue interface due to their immunomodulatory potential, 105 a study carried out with murine MSC seeded on alginate hydrogels of varying stiffness (3, 18, and 30 kPa) showed a direct correlation between hydrogel stiffness and inflammatory mediators release such as Indoleamine 2, 3-dioxygenase 1 (IDO1), and prostaglandin E-2 (PGE-2). 106
Besides gels, various nanofibrous membranes containing nanoreservoirs of bioactive molecules have also shown promise in promoting the tissue regenerative potential. For example, Polycaprolactone (PCL) membrane loaded with the anti-inflammatory agent ibuprofen showed downregulation of pro-inflammatory markers in vitro and confirmed decreased periodontal pocket depth and OC activity in experimental periodontitis mouse model as well. 75 Likewise, MSC incorporated on BMP-2 functionalized PCL membrane exhibited significantly improved maxillary bone regeneration in vivo. 107
Biomaterial-induced neutrophil activation in response to surface properties alters macrophage polarization. Murine neutrophils on rough-hydro Ti decreased pro-inflammatory cytokine and enzyme production as well as decreased NET formation compared to neutrophils on smooth and rough Ti. Hydrophilic Ti surfaces reduced neutrophil inflammatory response and NETosis, and enhanced anti-inflammatory macrophage polarization, thereby, highlighting that neutrophils are sensitive to modifications in biomaterial surface characteristics and exhibit differential activation in response such changes. 108
Certain carbon-based materials such as graphene and its derivatives also present remarkable physical, chemical, and biological properties owing to their high specific surface area and mechanical strength. They promote differentiation of stem cells and improve mechanical properties of biomaterials. The structure and strong C-C bonding in graphene enhances proliferation and differentiation of bone cells because of high electrical conductivity. Polymeric biomaterials are widely used in reconstructive and regenerative dentistry, however, are not suitable for load bearing areas. To overcome such issues, graphene and its derivatives can be blended with polymers to produce composites with improved properties. Recently, the reduced graphene oxide combined with photo-crosslinked gelatin hydrogel mimicking the procallus induced bi-differentiation of MSC for rapid bone repair through osteogenesis and angiogenesis, by activating Erk1/2 and AKT pathways. The methyl vanillate delivered by gelatin-n-reduced graphene oxide also contributed to the bioactive signals of the biomimetic procallus through osteogenesic differentiation of MSC. In a calvarial defect in vivo, bi-differentiation of MSC promoted rapid bone regeneration. 109 In this context, several studies have tested graphene coated dental implants in vitro and in vivo and demonstrated better cytocompatibilty, cellular attachment and proliferation, higher osteogenic differentiation of stem cells, antibacterial activity and bone formation.110,111
Currently, the trend has shifted from bioinert to bioactive biomaterials for the regulation of local inflammatory environment to promote bone healing. Literature shows that copper ions (Cu2+) released from micro/nano-topographical bio-ceramic surface exhibited anti-inflammatory effect by regulating integrin and TLR signaling. 112 Besides, bioactive Ti metals prepared by anodic oxidation exhibited appreciable anti-inflammatory properties. 113
Biological modification of biomaterials to modulate inflammation
Various bioactive molecules can be incorporated into the scaffolds or implant surfaces through nanoreservoir deposition, nanoemulsions, core-shell electrospinning, grafting, immobilization.75,104,107
Several studies have established the immediate anti-inflammatory capacity of coatings based on glycosaminoglycans (GAGs) that are long, unbranched polysaccharide chains including hyaluronic acid, chondroitin sulfate and heparan sulfate. GAGs are sulfated to varying degrees, however, hyaluronic acid is unsulfated. 114
Macrophage adhesion, macrophage spreading morphology, FBGC formation, as well as β1 integrin expression and IL-1β production were all significantly decreased on GAG-modified surfaces. 115 Besides, anti-inflammatory surface coatings composed of multilayers of heparin and naproxen loaded NPs demonstrated reduced IL1-β secretion due to an anti-inflammatory activity of heparin as polyanion amplified with naproxen release from NPs with cationic surface charge. 116
Interestingly, heparin has the ability to bind with various chemokines, cytokines, and growth factors, ultimately, modulating inflammatory response. In this regard, heparin inhibits the NFκB, which in turn suppresses leukocyte activation, thus, down-regulating the pro-inflammatory cytokines production. Moreover, heparin-based coatings have demonstrated superior properties when compared to other GAGs-based systems due to high wettability, negative surface charge, and intrinsic anti-inflammatory activity. Such surface coatings also help in reducing FBR to some extent. 117
In addition to the anti-inflammatory scaffold strategies, antibacterial matrix biomaterials, antibacterial coatings and films, nanostructured materials and antibacterial fibers that possess anti-infective, bacteriostatic/bactericidal properties, or anti-biofilm activities have also been proposed. Such strategies involve the utilization of bioglass-based or graphene-based antibacterial matrix, nano-coated metallic ions. 118 Peptide-modified PLGA nanoparticles against oral biofilms have also shown success in a murine model of periodontitis. 119
Interestingly, polymer brush coatings have been proposed to link biomaterial surfaces with biological cues in order to modulate the response of adhering cells. 120
The bioactivation of gelatin scaffolds by inorganic cues induced positive cellular response compared to neat scaffolds in terms of increased cell proliferation and early osteogenic differentiation of human MSCs, as evidenced by the ALP expression. Similarly, BMP-2 peptide decorated scaffolds showed higher values of ALP than biomineralized ones at longer time, demonstrating an osteoinductive effect of bioactive signals (either inorganic or organic) at nanoscale level on human MSCs, thereby, promoting bone regeneration. 121
Besides, biomimetic chitosan-based scaffolds promoting bone tissue regeneration and controlling inflammatory response have also been widely tested. For instance, chitosan was also effective at reducing IL-8 expression in stimulated fibroblasts. 122 Moreover, highly microporous chitosan/agarose/nanohydroxyapatite bone scaffolds induced osteogenic differentiation (Runx2 synthesis) in undifferentiated MSCs. The surface of such scaffolds is extremely hydrophilic, prone to protein adsorption with the highest affinity toward fibronectin binding, which allows for good OB adhesion, spreading, and proliferation. 123
Besides, N-acetyl-d-glucosamine oligomers (chitin oligosaccharide; NACOS) and d-glucosamine oligomers (chitosan oligosaccharide; COS) have anti-inflammatory properties. NACOS also significantly inhibited the LPS-induced RAW264.7 inflammatory response with some differences between various polymerization degrees. 124 Besides, pretreatment with COS could attenuate the lipopolysaccharide (LPS)-induced macrophage inflammatory response through competitive binding of COS with LPS that inhibits the binding of LPS to its pathogen-associated molecular pattern (PAMP) receptor TLR4, to diminish the pro-inflammatory pathways including NF-κB and MAPK. 125
PEEK presents a potential dental material owing to its excellent mechanical and chemical properties, specially, a similar elastic modulus to that of human bone. Surface modification using dexamethasone plus minocycline-loaded liposomes bonded by a mussel-inspired polydopamine coating decreased pro-inflammatory response and discouraged bacterial colonization in vitro. Furthermore, in vivo, anti-inflammatory effects of this surface modified PEEK were demonstrated in beagle dog’s femur defect model. 126
Several modifications can simultaneously be incorporated on the same implant surface. For instance, computer-aided design model and selective laser sintering were used to design Ti implants with a dense inner porosity (pores diameter, 400 µm) and a highly porous external surface (pillar diameter 300 µm), and chitosan/hydroxyapatite composite coating was added to their surfaces. In vivo, the implantation of surface modified implants into the rabbits’ femoral defects exhibited no inflammatory cell infiltration and improved osteogenic response. 127
Discussion
Bone defects resulting from trauma, diseases such as periodontal disease present a common health problem worldwide. Globally, there is an unprecedented high demand for soft tissue and bone tissue engineering alternatives. In the United States and Europe, more than half a million patients annually receive bone defect repairs with a cost estimated to be >US$3 billion. The global biomaterials market size is projected to reach USD 47.5 billion by 2025 from USD 35.5 billion in 2020. 128
Dental implants and certain bone graft or regenerative procedures are extremely expensive and, therefore, their failure is a huge economical concern for the patients. The optimization of their composition and surface properties to enhance their longevity and successful tissue integration and regenerative outcomes is, hence, imperative to improve their cost-effectiveness. Nevertheless, development of cheaper yet efficient alternatives is the need of the hour in this context.
Natural biomaterials possess relatively poor mechanical properties limiting their applications in anatomical sites with demanding mechanical loading such as hard tissue regeneration. Thus, in order to improve such properties, natural polymers are often combined with synthetic ones to produce hybrid biomaterials that enjoy the advantages of both classes of polymers without compromise. 129 Combining biomaterials with osteogenic, angiogenic, or anti-inflammatory agents to enhance their pro-osteogenic potential presents a powerful therapeutic tool. However, despite various tissue engineering strategies and their surface modification techniques, very limited scaffolds have qualified for preclinical testing. For instance, in the context of periodontal regeneration, only Emdogain and hyaluronic acid have been approved clinically, however, it still needs improvement to ensure predictability of tissue regeneration.130,131
Biological scaffolds show degradation upon long term storage. Furthermore, depending on the source, they exhibit high variability in terms of reproducibility and compatibility. Their undefined degradation rate poses another challenge for optimizing the regenerative outcomes. At contrary, synthetic scaffolds have potential toxic degradation of byproducts. 132
Indeed, it is challenging to develop scaffolds that mimic closely the native bone tissue by steering local MSC migration into the scaffold, thereby, promoting osteodifferentiation and ECM deposition. 133 The synchronization of the biomaterial’s resorption with bone remodeling so that the bone can eventually replace the scaffold is a critical point in determining the success of the regenerative therapy. In this regard, surface modifications that can control this rate and adapt it to allow subsequent bone remodeling and maturation will be important to promote the regenerative potential of the scaffold. 28 Furthermore, soft tissue adhesion with the dental implant is of prime important in determining the outcome of the implant success. In this regard, development of porous Ti coated with laminin-5 functionalized multilayered polyelectrolyte films composed of Poly(l-lysine) and poly(l-glutamic) acid showed tightly sealed the soft tissue -implant interface, consequently, preventing peri-implant inflammation. 134
Mechanotransduction is a process by which cells sense mechanical stimuli such as elasticity, viscosity, and nanotopography of extracellular matrix and translate them into biochemical signals. The mechanotransduction regulates several aspects of the cell behavior, including migration, proliferation, and differentiation in a time-dependent manner. Hence, it will be instrumental to explore further the dynamics of mechanotransduction to understand better the interaction between cells and biomaterials in order to design new optimized biomaterials for clinical therapeutic applications in tissue regeneration. 135 Implantation of biomaterials can induce an exaggerated inflammatory and immune response in tissue with local effects due to interactions between blood and biomaterial surface such as foreign body reaction, infection, influence on the normal therapeutic course or outcome, edema, toxicity, and carcinogenesis. Besides the local risks, systemic effects such as biomaterial particle embolization, hypersensitivity reactions, and increased amounts of chemical compounds or degradation by products can result with the biomaterial scaffold implantation in the body. The potentially toxic components of biomaterials include surfactant-like compounds, residual monomers, and plasticizers. Damage to the metabolic activity of the cell can be caused by reactive substances, for example, heavy metal ions, residual monomers, or radicals. 136 Such toxic substances can exert biological effects such as inhibition of cellular enzymes, calcification, and absorption of the synthetic material and also the physical and mechanical effects such as fatigue, abrasion, corrosion, and dissolution. Besides, the possibility of a host versus graft reaction further establishes the intricate yet highly important interaction of biomaterials with the targeted tissues. 137
Indeed, oral cavity is a complex of soft and hard tissue with several different cell types having different rates of proliferation and migration. Therefore, it is challenging to achieve a co-ordinated healing and regenerative response of the soft and hard tissue in the dynamic oral micro-environment. The implanted biomaterial scaffolds should have a strong affinity for targeted cells in order to stimulate neo-tissue formation, which depends on optimization of their associated physical, chemical, and biological surface properties (Figure 4). Further improvement in the analytical techniques and standards could be instrumental in the investigation and visualization of the interface between biomaterials and cellular/tissular component in order to promote tissue regeneration.

Physical, chemical, and biological modifications of biomaterials can dictate the cellular response to biomaterial scaffold implantation, thus, preventing foreign body giant cell formation. Such modifications can limit biofilm formation and can promote bacterial phagocytosis, opsonization, and apoptosis by macrophages. Optimization of surface properties of biomaterials can cause the macrophages to switch to the anti-inflammatory M2 phenotype.
An intricate interplay of immune and inflammatory pathways comes into action due to implant-tissue interaction, for instance, nanotubular TiO2 demonstrated regulation of macrophage M2 via the ERK1/2 and PI3K/AKT pathways. 138
It is note-worthy that different modification produce different biomaterial surfaces, leading to a surface-specific immune-inflammatory response. All biomaterial scaffolds possess some inherent weaknesses that must be overcome through modification techniques to ensure their successful tissue integration. For instance, PEEK is biocompatible and has an elastic modulus similar to that of natural bone. Nevertheless, implantation of smooth-surfaced PEEK implants forms a fibrous interface leading to poor integration with surrounding bone and eventual implant failure. This is mainly caused by the hydrophobic and chemically inert nature of PEEK. However, plasma-sprayed Ti coating to PEEK has shown direct bone ongrowth effect in long bone defect model in sheep.139,140 Interestingly, a study demonstrates that porous Ti with a mean pore size of 279.9 ± 31.6 μm developed by melt extrusion method showed better osteogenic differentiation in vitro and superior implant osseointegration in vivo when compared to a plasma-sprayed Ti coated PEEK (0.13–0.25 mm thick layer of Ti) in a tibial bone defect rat model. 141 PEEK implants still lack the desired physical properties and osseointegration capacity to be clinically applied and are being rigorously tested and improved.
Ti and its alloys are considered as the most biocompatible implant material because of their inert biochemical nature. Intrinsically, Ti has a relatively poor shear strength and a tendency for severe wear and tear, specially in a harsh oral environment. 111 However, till date, there has not been a system that could completely replace Ti dental implants. Current Ti dental implants are used universally and have a high success rate except in some cases. Several coatings are also applied to modify Ti implant surface and the particles can be released from the coating layers or from the Ti implant itself. Studies involving Ti powder plasma-spray-coated Ti implants and fluorohydroxyapatite-coated Ti implants demonstrated Ti dispersion inside the medullary spaces caused by the friction at the implant-bone interface, compromising integration in the coating layer with subsequent release of detached metal particles into surrounding tissue. 142 Note-worthily, therapeutical agents such as fluorides and hydrogen peroxide can also promote the degradation of Ti-based dental implants and abutments causing toxic ions release. Specifically, corrosion is significant in case of low pH or high concentrations of fluoride or hydrogen peroxide environment. 143 Moreover, wear and corrosion debris such as ions and micro- and nanoparticles released into the surrounding tissues can stimulate peri-implant inflammation promoting pathologic bone resorption. 144
Furthermore, there have been reports of hypersensitive reactions such as erythema, urticaria, eczema, swelling, pain, necrosis, and bone loss due to Ti ion leaching from the dental implants.145–147 Appropriate measures must be taken to avoid such complications and their timely diagnosis is important for a symptomatic management of the issues.148,149
Interestingly, zirconia exhibits good biocompatibility and biomechanical properties, and a low plaque affinity, however, a significantly higher number of early failures and fractures have been reported for zirconia implants compared to Ti implants. 150 Zirconia implants lack elasticity, which is further augmented with the use of ceramic or zirconia crowns. 151
Several recent studies have demonstrated the beneficial impact of nanoparticles such as AgNPs, for the modulation of inflammatory response, nonetheless, most of the studies have been solely carried out in vitro. For effective and safe clinical application of such NPs, long-term in vivo data envisaging their anti-inflammatory and anti-bacterial action is indispensable. 152
Human monocytes incubated with nano (approximately 100 nm) and micro (approximately 5 μm) sized ZnO particles in a concentration range of 10–100 μg/mL revealed a higher propensity of nano ZnO particles in inducing cytotoxicity and inflammation thus warranting their cautious optimization for a clinical application. 153
Hyaluronic acid, inherently, is a weak scaffold material owing to its rapid degradation in vivo by hyaluronidase and high solubility leading to dissolution. Moreover, hyaluronic acid itself does not bind well to the surrounding tissue owing to its high molecular weight. Therefore, it is imperative to chemically modify, crosslink, or combined it with another polymer to promote cell adhesion and proliferation.114,154
For bone regeneration, calcium phosphate bone fillers and growth factor-based substitute bone grafts are currently used in the clinic. However, substitute grafts lack bone regeneration potential when used without growth factors. However, growth factors can present unwanted side effects such as uncontrolled bone growth. Collagen-based hydrogel grafts available on the market fail to provide structural guidance to native cells due to high water-solubility and faster degradation. To overcome these limitations, nanoscale banding patterns were developed with nanocomposites that promoted biomimetic apatite-like mineral deposition in vitro. Additionally, chitosan-kappa carrageenan mineral-hydrogel nanocomposites enhanced bone regeneration in critical size mouse calvaria defect model without added growth factors compared to non treated defects. 155
Implantation of biomaterials can induce an exaggerated inflammatory and immune response in tissue with local effects due to interactions between blood and biomaterial surface such as foreign body reaction, infection, influence on the normal therapeutic course or outcome, edema, toxicity, and carcinogenesis. Besides the local risks, systemic effects such as biomaterial particle embolization, hypersensitivity reactions, and increased amounts of chemical compounds or degradation by products can result with the biomaterial scaffold implantation in the body. The potentially toxic components of biomaterials include surfactant-like compounds, residual monomers, and plasticizers. Damage to the metabolic activity of the cell can be caused by reactive substances, for example, heavy metal ions, residual monomers, or radicals. 136 Such toxic substances can exert biological effects such as inhibition of cellular enzymes, calcification, and absorption of the synthetic material and also the physical and mechanical effects such as fatigue, abrasion, corrosion, and dissolution. Besides, the possibility of a host versus graft reaction further establishes the intricate yet highly important interaction of biomaterials with the targeted tissues. 137 Implantation of scaffolds may cause an inflammatory and immune response in tissue, FBR, systemic toxicity, and imminent infection.137,156
Also, biomaterial scaffold implantation can cause both local and systemic complications such as damage to organs, for instance, following administration with large doses of TiO2 NPs as NPs can also cross the blood-brain barrier leading to toxicity.157–160 Therefore, caution must be exercised while optimizing them for size, concentration, micro/nano architecture, or surface chemistry.
Given the intricate nature of the immune-inflammatory cascades following biomaterial implantation, no single surface modification strategy can successfully control inflammation control. Therefore, combination of two or more such techniques could be a promising tool in future regenerative medicine.161–163
The main limitation of this review is that heterogeneity of the biomaterials, cell types, animals, and experimental conditions of the concerned studies hampers a comparison between the various surface modification techniques for the control of inflammation. In the future, a greater understanding of macrophage polarization and induction of other inflammatory-immune cascades triggered in response to specific surface properties of biomaterial scaffolds will be highly instrumental in the therapeutic modulation of inflammation through optimization of biomaterial surface properties.
Conclusion
The interphase between the biomaterial scaffold and cells plays a key role in determining the latter’s response toward the former. The physical, chemical, and biological properties of biomaterials influence significantly the orchestration of such response involving inflammatory and immune pathways. Several studies have demonstrated in vitro and in vivo that the cell-biomaterial interaction can be positively regulated by harnessing the biomaterial surface properties. This review highlights the feasibility and importance of modulating inflammatory response by optimizing the physical, chemical, and biological characteristics associated with the biomaterial scaffolds, thereby, downregulating the pro-inflammatory inflammatory-immune cascades and upregulating the anti-inflammatory and pro-resolution pathways. Further research into strategies to control inflammation through biomaterial surface modification is, therefore, warranted.
Footnotes
Author contributions
Fareeha Batool, Hayriye Özçelik, Olivier Huck contributed to conception and design, data acquisition and interpretation and drafted the manuscript. Céline Stutz, Pierre-Yves Gegout, Catherine Petit, Nadia Benkirane-Jessel contributed to analysis and critically revised the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Authors were supported by their Institutions.