
Abstract
Hollow, tubular organs including oesophagus, trachea, stomach, intestine, bladder and urethra may require repair or replacement due to disease. Current treatment is considered an unmet clinical need, and tissue engineering strategies aim to overcome these by fabricating synthetic constructs as tissue replacements. Smart, functionalised synthetic materials can act as a scaffold base of an organ and multiple cell types, including stem cells can be used to repopulate these scaffolds to replace or repair the damaged or diseased organs. Epithelial cells have not yet completely shown to have efficacious cell–scaffold interactions or good functionality in artificial organs, thus limiting the success of tissue-engineered grafts. Epithelial cells play an essential part of respective organs to maintain their function. Without successful epithelialisation, hollow organs are liable to stenosis, collapse, extensive fibrosis and infection that limit patency. It is clear that the source of cells and physicochemical properties of scaffolds determine the successful epithelialisation. This article presents a review of tissue engineering studies on oesophagus, trachea, stomach, small intestine, bladder and urethral constructs conducted to actualise epithelialised grafts.
Introduction
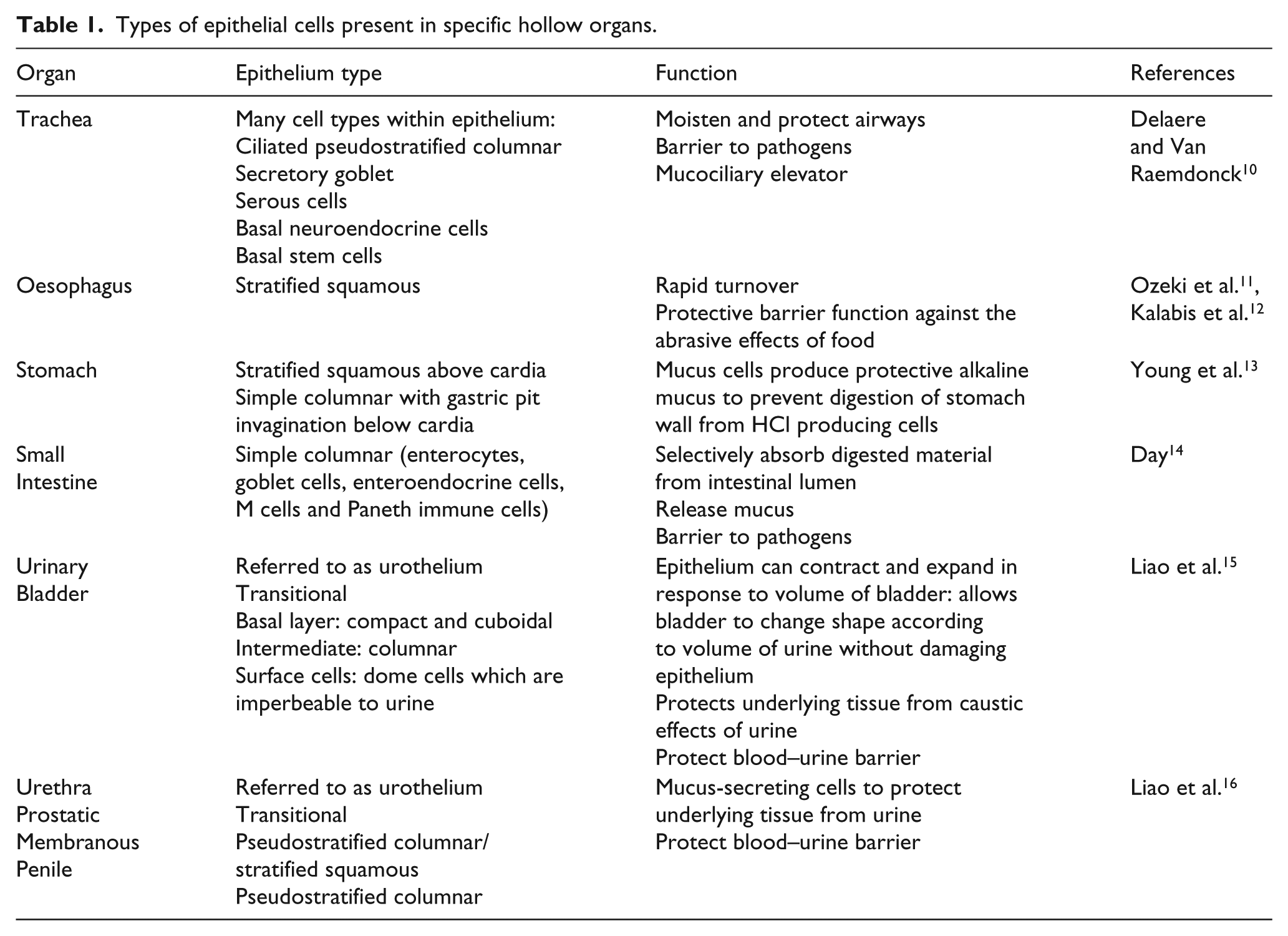
Hollow organs may be affected by a variety of disease processes – congenital malformation, autoimmune disease, inflammation, infection and cancer to name but a few potential problems. Current treatment generally relies on resection and/or replacement of this tissue. Resection of tissue is often only successful when relatively small segments of the organ are affected. Ultimately, having less surface area by large-scale removal of tissue leads to the organ having reduced functionality as seen in problems such as short bowel syndrome arising from loss of a component of the digestive system.1–5 Attempts to replace tissue have been made using mucosal grafts from other parts of the body; however, this can cause subsequent problems at the donor site: reconstruction of hollow organ tissue is susceptible to leakage, rejection, stricture formation, stenosis and may require continuous stenting to maintain patency.6–8 Epithelialisation is crucial to maintain patency of organs, and a lack of epithelial cell layer can lead to over-proliferation of underlying fibroblast layer leading to stricture formation, stenosis and potential graft failure 9 in addition to organ-specific functions. (Table 1)
Types of epithelial cells present in specific hollow organs.
This increasing burden of unmet clinical need is driving the search for effective procedures to develop functional epithelialised organs. Tissue engineering has already advanced sufficiently to create various organs synthetically for transplantation or reconstruction: examples include the world’s first tissue-engineered bladder. 17 However, epithelialisation of these synthetic organs is a process that is proving difficult to replicate in vitro.
Understanding the nature of epithelial cells is an important consideration when designing epithelialised tissue-engineered structures. Epithelial cells are finely tuned to their specific organ (Table 1). Epithelial cells can be lining hollow organs as surface epithelium 13 (Figure 1). At this interface, epithelial cells carry out functions such as creating a protective barrier for underlying organ; absorption of luminal contents; secreting substances into the lumen such as mucus by the goblet epithelial cells in the trachea or digestive enzymes secreted by the stomach and small intestine; controlling passage of materials across body surface by selective diffusion; and containment of luminal contents. 18 Cells are usually found as a continuous sheet of cells that, in some organs, can be stacked to form layers. The cells reside upon a basement membrane, which demarcates the border between epithelial cells and underlying cells. This basement membrane is not penetrated by blood vessels, and therefore, epithelial cells rely on simple diffusion for supply of oxygen and nutrients. 19

Types of epithelium corresponding to distinct physiological systems.
This article focuses specifically on the epithelialisation of hollow organs such as trachea, oesophagus, stomach, small intestine, colon, urinary bladder and urethra, where their tubular forms distinguish them from other more solid, visceral organs such as the heart and liver and give a prominent role to the luminal epithelial layer, which is in contact with the external environment. This review aims to evaluate the materials and fabrication methods, which have been successful in producing scaffolds and their limitations, with a view to present these as lessons in designing more optimal scaffolds for a functional epithelium associated with tubular structures.
A host of factors determine epithelial–material interactions which include mimicking extracellular matrix (ECM). For example, scaffold pores should be large enough to allow vascular infiltration and angiogenesis, but not too large to prevent formation of cell layering and epithelial cells slipping through; hydrophilic surface to promote cell adhesion; appropriate tensile strength appropriate to the replaced organ; biodegradable and appropriate rate of degradation to allow successive replacement with native tissue; surface morphology to support cell adhesion; ability to mould into appropriate tubular structures; non-immunogenic; non-toxic; responsive to growth; and easy to produce and transplant into patient.22,23
Numerous types of scaffolds have been developed for hollow organ development. The wide range of materials available and their interaction with epithelial cells are illustrated in Table 2.
Epithelialisation of tissue-engineered scaffolds.

PCL: polycaprolactone; SF: silk fibroin; PLGA: poly(lactic-co-glycolic) acid; PLLA: poly(lactic acid).
Types of scaffolds
Biological scaffolds
Decellularised scaffolds
Biological, decellularised scaffolds can be created from donor human or animal tissue. Decellularisation involves removing cells expressing major histocompatibility complex (MHC) class I and II antigens to stop an immunogenic response using detergent. 26 Decellularisation of tissue can be done using chemical treatment of NaClO4; 37 however, this method has not been widely used. Detergent-enzymatic method has been very popular and generally yields good results.11,38–42
This method removes immunogenic components of tissue while maintaining structural integrity to cope with the biological flow stresses in vivo. The scaffold is biologically active due to native ECM proteins and with pro-angiogenic, chemotactic growth factors remain intact even after the decellularisation process. 42 They facilitate cells forming crucial cell–ECM interactions, culminating in organ remodelling required for transplantation. 17 However, there are several limitations to this method.
Decellularised scaffold relies on donor organs; thus, it does not overcome the global issue of transplant donor organ shortage. Furthermore, decellularisation does not lead to absence of inflammatory response but it is a comparatively reduced inflammatory response in comparison with allogeneic or xenogeneic grafts. While this may be some form of progress, inflammation can still arise. Both inflammation stenosis and stricture formation have been observed in various decellularised tubular scaffolds, in the absence of cells.16,35,43 Therefore, decellularised scaffolds may require stenting to prevent graft collapse and the long-term biodegradability of decellularised scaffolds being unknown. There is also a lack of uniformity between scaffolds and unable to tailor the graft to the requirements of the recipient. 44
Fibrin gel
Fibrin gel is created from fibrinogen and thrombin found in the blood to create a gel-like substance, and this can be easily extracted from autologous blood. 45 Bronchial epithelial cells were shown to produce confluent layer and ciliary production when seeded on fibrin gels. 24 However, in another study, the cells that grow show less structured layering, rounder cells and more immature cilia formation than original tissue, as cytokeratin patterns in experimental models do not correspond to cytokeratin patterns in native trachea. 46 And the significance of epithelial tissue is reiterated by Heikal et al., 47 where fibrin constructs with cells were not implanted and it led to fibrosis and stenosis.
Advantages of fibrin gel are that it is easy to seed cells and mould the gel into appropriate structures. However, due to its relatively fragile nature, it needs to be supported by a mesh if used to replace tubular organs. 48
Collagen
Abundant in the ECM, collagen is a good source to use when culturing epithelial cells. A collagen-coated polypropylene mesh has been used for airway reconstruction, 49 while collagen scaffold–incorporated fibroblasts have been shown to regenerate tissue and enhance wound healing. After 14 days, epithelialisation and cartilage formation was observed throughout the scaffold, more rapidly than the control. 50 This use of collagen-modified scaffolds with stem cell–epithelial cell co-culture encourages mesenchymal cell migration into the scaffold, which may produce basement membrane proteins and growth factors. 51
Basic fibroblast growth factor (bFGF) was incorporated into a collagen vitrigel membrane, which then covered an artificial trachea made of Marlex® polypropene mesh and collagen sponge. There was stratified epithelium, columnar cells and ciliated cells at day 5, 7, and 14, respectively. 52
OptiMaix-3D collagen-coated scaffolds are prone to epithelial cells passing through or clustering rather than seeding uniformly on the surface. Two-dimensional (2D) scaffolds showed monolayer formation and no cell migration through the scaffold but have limited applicability.53–55 As collagen coating may lead to slow or partially epithelialised surfaces, coating the collagen surface with L-C co-polymer keeps this collagen layer intact and yields more positive results. 56
The useful effects of collagen may not be specifically restricted to its physical properties as a scaffold, but also after its degradation, it can improve vascular growth and lead to desmin-positive tissue formation. 57
Chitosan
Chitosan is a natural polymer derived from chitin. It can be easily modified and complexed with other proteins. Unmodified chitosan leads to no cell adhesion. Modified chitosan scaffold coated with fibronectin or elastin transiently leads to the formation of strong cell adhesion contacts, but cells eventually undergo de-adhesion. There has been some link to collagen–chitosan complexes supporting oesophageal epithelial cell adhesion and proliferation. 31
Gelatin
Gelatin is often complexed with other materials. It is shown to be a biodegradable and bioabsorbable natural polymer, with neovascularisation and epithelial growth seen and degeneration after 2 months. Epithelial markers such as pan-cytokeratin staining, while initially positive, become negative after 4 months. It is a good material for initial adhesion and growth of cells, but poor at maintaining differentiation of buccal mucosa. 36
Gelatin has also been combined with other proteins such as decorin–gelatin electrospun complexes. There was greater adhesion of cells and increased cell layer formation in comparison with simple gelatin scaffold. To improve differentiation, there is a need for greater exposure to biophysical flow stress exposure. Also, the pore sizes created by electrospinning technique are too large for successful epithelialisation. 25
Gelatin was also combined with dextran sulphate to form dextran sulphate–gelatin membrane. Full tracheal regeneration was observed, but it took 2–3 months and there is a high risk of stenosis in the organ. Furthermore, immunogenic reaction was seen towards this membrane. It is worth noting that hyaluronate-rich extracellular components allow it to have strong cell–scaffold interactions. 9
Synthetic scaffolds
Synthetic polymers being increasingly investigated as natural materials prove to be mechanically weak. However, while the physical strength, biocompatibility and bioabsorbability of these polymers are promising, poor cell adhesion hinders their use. Synthetic scaffold success with regard to epithelialisation relies on four main stages epithelial cells have to progress: migration to correct site; adhesion of cells to surface; proliferation of cells to increase in number and repopulate area; and finally, differentiation to mature cell type or cell type seen in vivo models. Different factors target different stages, and thus, the challenge is to create a scaffold material that can successfully progress through all four of these stages.
Silicone stents were used as a scaffold for urothelial growth with an attempt to grow bladder epithelial cells in porcine models. Better results were in fact seen on latex scaffolds, but this may not be universally clinically applicable. 4 Polyglycolic acid (PGA) mesh using poly(lactic acid) (PLLA) glue was used to seed stomach epithelial cells such as gastric patches. The results show neomucosa formation with smooth muscle proliferation and no clear discontinuity between donor and recipient mucosa. 1 Previous work on polycaprolactone (PCL) has been developed in the fields of bone58,59 and oesophageal 27 tissue engineering. Electrospun PCL was seeded with primary oesophageal epithelial cells. While PCL nanofibres show high tensile strength and slower degradation, there was greater cell proliferation on PCL–gelatin hybrid. A PCL–silk fibroin hybrid also promoted the epithelial cell attachment and proliferation. Mitochondrial activity increased when the material was coated with extracted basement membrane proteins. 27 These findings demonstrate the importance of a combination of molecular profiles to enhance cell attachment. Poly(lactic-co-glycolic) acid (PLGA) is a biodegradable polymer, and the material shows rapid degradation and useful biocompatibility properties. It also has reduced irritation of sensitive tissues and so may be applicable to urethral stents. 60 Precoating with collagen type IV has shown to increase adhesion and proliferation but differentiation is limited. 29 A mesh knitted with PLGA and polypropylene for tracheal reconstruction showed good mechanical properties, which were enhanced after coating with polyurethane. However, there was patchy ciliated columnar epithelium intermittently along the graft, rather than the desired confluent layer, even after 6 weeks. 61
Scaffold fabrication with three-dimensional printing
A range of biofabrication methods can be used to develop tubular scaffolds (Figure 2). Conventional methods to create scaffolds for tissue engineering such as gas foaming 62 and phase separation 63 are useful, and there is a need to regenerate the scaffold’s submicron internal architecture and initiate a degree of bioactivity for scaffolds to support epithelialisation. Additive manufacturing methods or three-dimensional (3D) printing can offer methods that can enable precise reproduction of the tissue’s size and shape. 64 There are a variety of bioprinting methodologies that include stereolithography apparatus, thermal inkjet printing, fused deposition modelling and powder binding. Stereolithography (SLA) 65 uses an excess layer of liquid photopolymer or epoxy resin. A low-power ultraviolet (UV) laser is then used to cure the excess liquid into a solid object. The excess raw materials and supporting structures must be removed and then cured in a UV chamber. A platform is positioned such that a thin layer of photopolymer/epoxy resin (0.05–0.15 mm) exists above the platform, exposing it to the UV laser. 66 As the UV beam comes into contact with the liquid plastic, it instantly hardens forming a thin, solid layer at the surface of the platform. 67 Each layer produced represents a cross section of the desired 3D object. The platform then moves to allow the superposition of subsequent layers until the desired thickness is reached. This system can be used with living cells and biomaterials. 68 Thermal inkjet printing shows promise in regenerative medicine and has generated the foundation for future organ-printing technologies.69,70 With this method, living cells are printed in the form of droplets from a printhead onto a substrate (as opposed to printing them on scaffolds) in accordance with instructions sent digitally from a computer to the printer. The droplets are ejected using compression generated either mechanically or using thermal energy. The droplet size can be as small as 10–150 pL. This can be modified by altering the pulse frequency, temperature gradient or the viscosity of the bio-ink. Fused deposition modelling has a printhead similar to that used in a thermal inkjet printer. 71 Layers of material are created by the deposition of material such as plastic as the printhead moves.70,72 The process is repeated allowing very precise control of the amount and location of each droplet of material at each layer. 73 As the material is heated, it fuses as it cools to the layers below. 73

Possible biofabrication methods to develop hollow, tubular scaffolds to replace/repair tubular organs.
There is also powder binding, by which a layer of powdered material placed on a surface and a solvent (or liquid binder) is selectively deposited onto the powdered surface by a printhead. The solvent (or liquid binder) causes the powdered material to bind together to form a fragile but solid material of a predetermined geometry. In addition to hollow, tubular scaffolds, stents are widely used to address disease and damaged tubular structures. Strut structure, high radial strength (needed to maintain tubular diameter), low recoil, high radiopacity (to ensure precise positioning) 79 and conformability (lack of conformability or increased stent rigidity) leading to failure are significant features. 80 Table 3 contains a summary of the advantages and disadvantages of various 3D printers.
Advantages and disadvantages of 3D printers.

3D: three-dimensional; UV: ultraviolet.
Stainless steel can be used to make stents which has the main advantage of being highly biocompatible and sufficient mechanical strength. However, there were a number of limitations such as high strut thickness, limited flexibility and low corrosion resistance. 79 Cobalt–chromium stent alloys are also used which allow for thinner struts without compromising radial strength or resistance to corrosion. The introduction of a platinum–chromium alloy stent appears to incorporate many properties such as radiopacity, thin struts, high radial strength and biocompatibility. These stents can be designed as drug-eluting stents 81 and can potentially modify to ensure epithelialisation or to eliminate patency-limiting factors through the introduction of functional epithelium mimicking bio-factors.
Properties considered when fabricating scaffolds for hollow organ development
Pore size and porosity
Pore size and porosity play an important role in mimicking natural ECM and for cells to attach. Electrospinning, salt sintering and 3D printing 82 are some methods by which pores are introduced. Porosity determines the mechanical strength of the polymer and the rate of biodegradability in non-biostable materials. Epithelial adhesion is shown to be optimal in scaffolds with pore sizes <10 µm. 18 Nanosized porous or fibrous surfaces have also been shown to be advantageous to cell and protein adhesion within scaffold surface but larger pores created by methods such as electrospinning produce larger diameter pores do not optimally suit epithelial cell seeding. 83
Hence, a laminated model seems to present a better solution with large pore sizes on the basal layer but smaller pore sizes on the luminal surface to allow for epithelial adhesion and prevent cell penetration. In the small intestine, cell sheets of varying porosity and cell size were compounded to make multi-layered scaffold. 84 The bilayered concept was also explored using electrospun scaffold where smaller pores are used in luminal surface and bigger pores for basal surface which is conducive for fibroblasts. 39 There is a need for scaffolds with a smaller pore size at the luminal surface for optimal epithelium attachment and proliferation. However, larger pores have shown to encourage bronchial epithelial cell aggregation, integration and vascular growth. 85
Stretchability/stiffness
The role of scaffold stiffness was long recognised to influence cell–material interactions, where soft polyacrylamide gels (E = 0.1−1 kPa) would direct mesenchymal stem cell differentiation towards neuronal phenotype such as brain. Relatively harder gels (E = 8 to 17 kPa) directed mesenchymal stem cells (MSCs) to become muscle cells, while the stiffest scaffolds (E = 25 to 40 kPa) produced osteogenic cells. 86 Recently, peristalsis has been shown to stimulate micromechanical processes such as rearranging lateral cell–cell adhesions and aligning cytoskeletal components. 87
Surface modification
Surface modifications to scaffolds such as introducing bioactive molecules88–90 can alter the surface chemistry, thereby modulating cell attachment and proliferation. Plasma treatment can introduce hydroxyl and carbonyl groups that increase hydrophilicity of the scaffold and increase cell adhesion. 91 The argon plasma ablation of polyethylene led to oxidation and increased surface roughness which had positive effect on fibroblasts cells. 92
An optimal scaffold mimics the basic structure of the ECM. The ECM co-ordinates the binding of cells. Cells also respond to the ECM via integrin receptors which recognise and interact with ECM components. Subsequently, leading to signal transduction intracellularly modifies cell behaviour.
Therefore, an ideal scaffold must be more than a passive support for cells. It is a much more dynamic and influential structure: binding various signals (such as growth factors and hormones) that are tailored to the surrounding cell type is responsive to the action of cells and adjusts nutrient supply to the cell accordingly.
The concentration of calcium to which epithelial cells are exposed enhances different stages of epithelial cell growth. Cells cultured under low calcium conditions show greater proliferative capacity. When calcium concentration increases, there is raised differentiation of epithelial cells and reduced proliferation. In synthetic scaffolds, it is the crucial step of adhesion, that is, one of the great challenges of tissue engineering. The calcium concentration was initially low, and after reaching confluence, it increased. 30
Such chemical and biological modifications on a scaffold can influence the surface wettability of a scaffold surface. Surface wettability refers to the hydrophilic or hydrophobic nature of the scaffold surface. Hydrophilic scaffolds tend to resist proteins, while hydrophobic scaffolds absorb proteins. Absorption of proteins might lead to distortion of the 3D conformation of the protein, making changes to the degree of cell adhesion and migration. 23 Moderately, hydrophilic materials are optimum for adsorption of proteins. Neither super hydrophilic nor super hydrophobic materials have shown to be ideal. 93
Cell sources for epithelialisation
Current scaffolds seem unable to rely on native cells for repopulation, as independently forming functional epithelium can be time-consuming and may impact the regeneration of underlying tissues due to reciprocal differentiation factors released from neighbouring tissue layers.30,94 The current studies on cell sources used for epithelisation are listed in Table 4.
Typical cell sources used for epithelialisation.
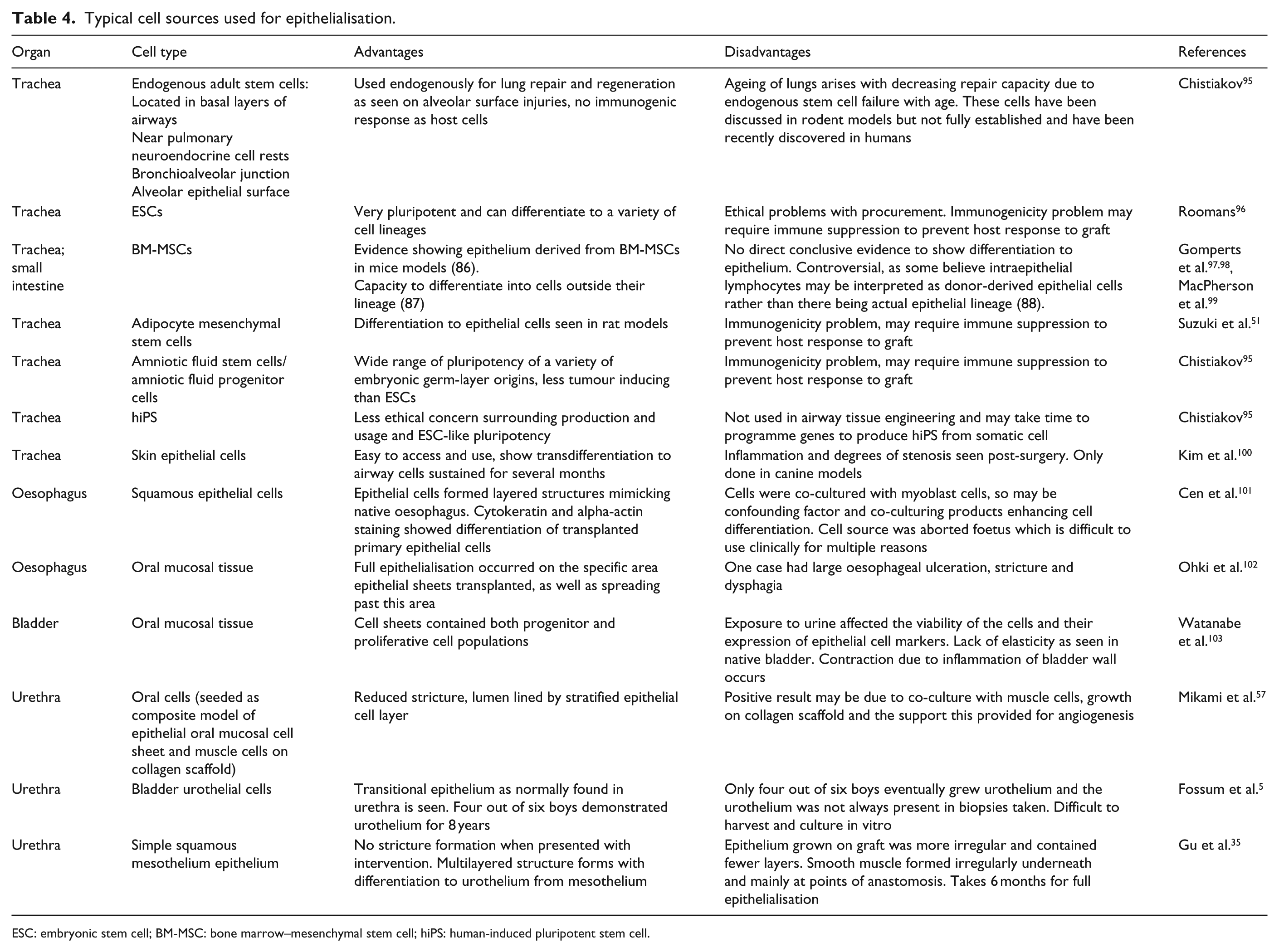
ESC: embryonic stem cell; BM-MSC: bone marrow–mesenchymal stem cell; hiPS: human-induced pluripotent stem cell.
Autologous source
It is also important to consider the immunogenic potential of grafted cells, a common concern in allogeneic or xenogeneic transplants. One way to solve this problem is relying on autologous cell transplantation. Studies have been carried out to establish culture systems for tracheal epithelial cells using tissue explant technique.104,105 While it would be intuitive to directly seed epithelial cells to allow epithelialisation, there is difficulty in epithelial cell extraction, optimal cell adhesion and sustained differentiation.41,106
There have been attempts to locate endogenous stem cells found within the site of the organ by looking at models in response to organ injury and determining where the new generation of cells to repair the organ and replace lost cells arise from, hoping to use this pool of undifferentiated cells for seeding. However, there are some cases where this proves difficult, such as in patients with reduced intestinal length due to ulcerative colitis or Crohn’s disease and may not have the capacity to provide the number of stem cells for adequate population of the graft. One solution for this may be in-vitro expansion of cells; however, intestinal epithelial cells have poor in-vitro growth, and this may reduce the clinical translatability of this method. 14
Stem cells
Pluripotent stem cell is a viable option. Bone marrow–mesenchymal stem cells (BM-MSCs) hold much potential, as BM-MSCs show cytokeratin expression and migration to replace damaged epithelial cells. Several papers reiterate the idea that epithelial progenitor cells are derived from bone marrow, which circulate and then recruit to the site of injury to reconstitute the repaired epithelium to some extent.97,98 Adipocyte MSCs showed a pseudostratified columnar epithelium along with goblet cells, cilia and angiogenesis in rat models for tracheal epithelial growth. 51 Human embryonic stem cells hold great potential but are wrapped in controversy. However, amniotic fluid stem cells or amniotic fluid progenitor cells display similar characteristics of bone marrow stem cells, but in rodent models have been shown to have ‘higher healing properties’, perhaps by influencing local oxygen levels. The stem cells have similar properties to the embryonic stem cells, but there are less ethical dilemmas surrounding these cells as well as less risk of being teratogenic. 95 Another cell source is human-induced pluripotent stem cells, and these can show embryonic stem cell–like activity using similar signalling pathways by modification of around four key genes. 107
Transdifferentiation of skin epithelial cells to tracheal epithelial cells presents a different method of obtaining epithelial cells. Results show cilia formation, and cells remain viable for several months. Despite inflammation after 1 month post-surgery and some stenosis 4 months post-surgery, this presents an interesting avenue of alternative cell sources for epithelialisation. 100
Co-culture
The use of cells seeded on scaffolds is actually one of some debates. Some papers argue that research should move to focus on ensuring the scaffold has sufficient factors to stimulate cell migration, proliferation and differentiation in vivo rather than using valuable resources procuring cells and fine-tuning technique to graft onto scaffold.
The bipotential scaffold fabricated by Tada et al. 108 aimed to show that native tissue infiltration is able to produce mucosal repair using native cells without the need for seeding.
Epithelialisation has shown to be optimal when co-cultured with fibroblasts or media conditioned with fibroblasts. The interaction between neighbouring mesenchymal cells and epithelial cells is crucial in differentiation of epithelium and graft development. Fibroblasts produce essential ECM, which also supports epithelial cells, secrete growth factor molecules such as bFGF, epidermal growth factor (EGF) and keratinocyte growth factor among others, each helping to develop the epithelium and surrounding mesenchyme. 109
Nasal respiratory epithelial cells and fibroblasts were grown together for 1 week using a fibrin and titanium mesh in ovine models, which reconstituted the basement membrane. 47 Fibroblasts continue to have this positive effect even in larger tracheal defects with ciliated, pseudostratified epithelium still seen. 106 Kobayashi et al. 110 also co-cultured epithelial cells with fibroblasts, leading to pseudostratified cilia goblet and basal cells formation and reciprocally, fibroblasts increasing mucin secretion by epithelial cells. However, their novel work was co-culturing fibroblasts and adipose-derived stem cells with tracheal epithelial cells. It transpires that each cell plays its own unique role in epithelial cell regeneration. The fibroblasts drive differentiation and pseudostratification of the epithelial cell layer, and adipose-derived stem cells drive proliferation, multilayering of epithelial cell sheets and accelerate neovascularisation. There are detailed synergistic effects of epithelialisation on both types of cells, as well as ion channel and basement membrane construction. 53
The inclusion of adipose-derived stem cells has indicated that other cells may also be implicated in improving epithelialisation shown by promising results with BM-MSCs and chondrocytes co-culture. 95 Pfenninger et al. co-cultured many human epithelial cells with various combinations of other cells including chondrocyte pellets, articular cartilage chips and collagen membrane plus chondrocytes. Epithelial cells were seeded internally and chondrocyte externally on the luminal surface of a decellularised tracheal grafts and placed in a bioreactor. Both cell types covered the matrix within 72 h and improved epithelialisation and graft survival. 109
Endothelial and epithelial cells have crucial and differing roles in response to injury. The epithelial cells contain the extent of the injury and stimulate mesenchymal hyperplasia to allow proliferation of cells to replace injured cells, while endothelial cells maintain and preserve epithelial cells and perfuse the injured tissue. This in turn produces factors for fibroblast migration and remodelling and further enhances epithelium growth. 111 This supports Beckstead in the oesophageal model, who has suggested that the regeneration of epithelium is crucial as it is linked to the regrowth of the underlying muscular layers in the oesophagus. 30
Other techniques of improving epithelialisation
The way in which cells are seeded onto the scaffold is important in epithelialisation of the tubular structures. Conventionally, cells are usually seeded onto scaffold while in a solution with the appropriate media, with individual or clusters of cells forming attachments. This method works fairly well; however, alternative methods of cell seeding onto scaffolds have been investigated. Figure 3 summaries the various factors involved to create the ideal tubular scaffold.

Factors influencing an ideal tubular scaffold.
Air–liquid interface
Air–liquid interface cultures are useful in airway epithelium formation. 39 In submerged conditions, murine embryonic stem cells differentiated to non-ciliated secretory Clara cells, but when using air–liquid interface culturing techniques, the stem cells differentiated to all three cell types of airway epithelium ciliated, basal, and secretory. 115
Epithelial cell sheets
The use of epithelial cell sheets has been shown to have regenerative potential even without scaffold support, commonly used therapeutically in oesophageal endoscopic submucosal dissection.102,113,116 The cell sheet is formed by lowering the temperature of the flask containing cells to around 20°C rather than trypsinising cells to seed them on scaffold in solution; however, mild fibrosis and substantial degree of constriction are still seen.94,117,118
In the context of synthetic scaffolds, cell sheet seeding may overcome the practical problem of epithelial cell adhesion as epithelial cells often infiltrate into the scaffold pores rather than forming a surface layer. 55 A skin graft of epithelial cells seeded upon cartilage sheets wrapped with external abdominal oblique muscle flaps and a silicone stent was performed and are well-vascularised and remodelled except for thin layers that led to poor epithelialisation. 119
Organoid units
An organoid is a bud of an organ which preserves the various cell layers on a smaller scale than the native organ, thereby allowing for interactions between different cell layers such as small intestines. 120 In intestinal models, epithelial differentiation through goblet and/or Paneth cell formation, as well as a progenitor cell layer forming below, is consistent with gastric epithelium and expression of gastric stem cell markers. 121 However, most of the cells die after implanting the construct as the complex organoid structure no longer receives adequate nutrition to the inner, more densely packed layers. In the gastric model, heterogeneity of cell types in different regions of the stomach meant that organoids may not have the full variety of cells seen in the native stomach. 121
Bioreactor
Exposure of the cell–scaffold construct within in-vivo environment may enhance tissue formation. All hollow organs mediate an interface between internal and external environments, and exposure of the graft to this interface allows important additional tissue development, such as immune cell lymphoid tissue. 14
A bioreactor can simulate this in-vivo environment as the graft matures. There was greater chondrocytes seeding on collagen scaffold when the scaffold rotated 5 to 20 r/min in a bioreactor. 122 This mimics in-vivo physiological signals such as shear stress, compression and pressure, thereby allowing cells to respond to them in vitro.
Using in-vivo bioreactor such as implanting urethral scaffolds in peritoneal cavities of rabbits and scaffolds was well covered in fibroblasts and mesothelium. There was no stricture formation when scaffolds were transplanted into rabbits. 123 Similarly, omentum was used as a bioreactor where oesophageal scaffolds were implanted. Results showed vascularisation, and its anatomical position can be used as a pedicle for subsequent transposition. 124 In-vivo bioreactors should be explored further to understand its interaction with host tissue.
Angiogenesis
The delivery of nutrients and oxygen to epithelium plays a key role in epithelisation. The diffusion limit of nutrients and oxygen is approximately 200 µm, and the lack of vessels severely restrict the size of tissue-engineered scaffolds. Hence, angiogenesis is important. 125 Therefore, vascular endothelial growth factor (VEGF) can be introduced to improve vessel infiltration. The administration of VEGF is, however, difficult but continuous delivery of VEGF may be possible through a bioreactor. Improved oxygen delivery may decrease lactate concentration in the graft and improve epithelial metabolism. 126 This has been investigated using perfluorocarbon-based artificial oxygen carrier (Oxygent). This has benefits in maintaining a functional basal lamina and decreased lethal airway obstruction, but also may lead to decreased chondrocyte function. 127
Concluding remarks and future direction
Biological scaffolds so far have presented relatively more successful results for tubular scaffold epithelialisation, originating from their ability to provide tissue-specific cues for cell–matrix interaction. Biomimicry of the natural tubular structures with synthetic scaffolds with the state-of-the-art materials and fabrication methodologies might be the way forward for effective epithelisation. Current non-biological approaches involve seeding cells on suitable scaffolds, but still lack the full range of crucial structures that mimic the ECM which are required to replicate these organ-specific cellular cues.
The best bioactive scaffolds would be those that use cell-signalling pathways to mimic the in-vivo repair and regeneration process. This is the strength of decellularised scaffolds, despite them lacking suitable mechanical strength, which could lead to graft failure. Furthermore, topography and physicochemical characteristics such as porosity, material strechability and surface wettability play a major role in epithelialisation. Embedding relevant growth factors within the scaffold may further enhance epithelial cell binding. Ultimately, to produce functional organs, it will be unlikely to rely solely on optimising cell seeding. It would be practical to improve scaffold intrinsic properties to allow autologous cells to migrate towards the scaffold of interest and transform into a functional tissue that can restore physiological homeostasis.
Footnotes
Author contribution
Authors Rhea Saksena and Chuanyu Gao contributed equally to this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.