
Abstract
In 2020, the European Medicines Agency approved subcutaneous (SC) vedolizumab (VDZ) for the maintenance treatment of adult patients with moderate to severe inflammatory bowel disease (IBD). This article reviews the efficacy, safety, persistence, pharmacology, patient satisfaction, and economic implications of transitioning to SC VDZ treatment and explores whether SC formulations can be recommended by the same guidelines as intravenous (IV) formulations. Clinical trials and real-world evidence indicate that transitioning from IV to SC VDZ in patients with IBD maintains clinical, biochemical, and patient-reported clinical remission and is well-tolerated, with no new safety issues identified, except for injection site reactions. Moreover, SC VDZ has an exposure–response relationship and low immunogenicity, is economical, and provides a high level of patient satisfaction. Owing to these advantages, transitioning may be advisable. In the future, more studies are needed to clarify the exact role of SC VDZ in IBD treatment, including optimization and transitioning strategies and individualized treatments based on baseline characteristics.
Plain language summary
Transitioning from intravenous to subcutaneous vedolizumab (SC VDZ) in patients with inflammatory bowel disease maintains clinical, biochemical, and patient-reported clinical remission and is well-tolerated, with no new safety issues identified, except for injection site reactions. Moreover, SC VDZ has an exposure-response relationship and low immunogenicity, is economical, and provides a high level of patient satisfaction. Owing to these advantages, transitioning may be advisable.
Introduction
Ulcerative colitis (UC) and Crohn’s disease (CD) are categorized as chronic inflammatory bowel diseases (IBD), characterized by symptoms including diarrhea, rectal bleeding, abdominal pain, fatigue, and weight loss. 1 Although the exact IBD etiology remains uncertain, genetic, environmental, microbial, and immune factors are generally implicated. 2 According to Selecting Therapeutic Targets in IBD-II, long-term goals emphasize endoscopic healing, absence of disability, and normalized health-related quality of life. 3 Current treatment options include conventional therapies [such as 5-aminosalicylates, immunomodulators, and corticosteroids (CS)], biological agents, and small-molecule drugs.4,5 Biological agents approved for UC and CD include tumor necrosis factor (TNF) antagonists (infliximab, adalimumab), the interleukin antagonist ustekinumab (UST), and the integrin antagonist vedolizumab (VDZ).
VDZ is a gut-selective humanized monoclonal antibody that specifically antagonizes the α4β7 integrin. 6 This integrin is preferentially expressed by intestinal helper T lymphocytes and interacts with mucosal address-cell adhesion molecule 1, which is predominantly expressed in intestinal endothelial cells. By binding to the α4β7 integrin, VDZ may limit the ability of certain leukocytes to infiltrate intestinal tissues. 7
Initially, lyophilized powder was reconstituted for intravenous (IV) infusion. The efficacy of VDZ was demonstrated in two phase III randomized controlled trials (RCTs).8,9 GEMINI 1 RCT revealed a UC remission rate of 41.8% at week 52, significantly exceeding that of the placebo (p < 0.001). GEMINI 2 RCT indicated that 39.0% of patients with CD on VDZ achieved remission at week 52 relative to 21.6% on placebo (p < 0.001). Accordingly, the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) approved VDZ on 20 May 2014 and 28 May 2014, respectively, for treating adults with moderate to severe UC and CD. With established efficacy and safety in real-world studies (RWS),10–12 guidelines from the last 5 years prominently feature VDZ4,5,13–18 (Supplemental Table 1). For CD, VDZ is strongly recommended for biologic-naïve individuals and those unresponsive to anti-TNF agents across all guidelines, except for the American Gastroenterological Association (AGA). Although the AGA suggests VDZ use in these situations, UST is recommended. For UC, the European Crohn’s and Colitis Organization recommends VDZ as a first-line treatment, whereas the American College of Gastroenterology and the British Society of Gastroenterology recommend it as a second-line treatment. Conversely, the AGA prioritizes UST or tofacitinib over VDZ for inducing remission after anti-TNF therapy failure.
Recently, a new subcutaneous (SC) formulation of VDZ was developed to provide patients with the choice of SC therapy. Therefore, this article reviews the efficacy, safety, persistence, pharmacology, patient satisfaction, and economic implications of SC VDZ. It also explores whether the same guidelines that apply to IV formulations can be reviewed to include SC formulations.
Approval of SC VDZ
In May 2020, the EMA approved the SC formulation of VDZ for the maintenance treatment of moderate to severe UC or CD in adults who demonstrated inadequate response, loss of response, or intolerance to conventional treatment or TNF antagonists. In September 2023, the FDA approved SC VDZ for maintenance therapy in moderately to severely active UC after induction therapy with IV VDZ and endorsed the review of the Biologics License Application for SC VDZ in CD therapy. However, approval for SC formulations for CD remains pending (Figure 1). Currently, SC VDZ is authorized for marketing in the European Union and over 50 other countries.

The gradual evolution of VDZ from intravenous to subcutaneous formulations in inflammatory bowel disease.
Patients should receive at least two IV VDZ doses before transitioning to SC VDZ maintenance therapy every 2 weeks (Q2W) at a standard dose of 108 mg. The initial SC injection aligns with the next scheduled IV infusion. After training on self-administering SC injections, patients can self-inject at home with the physician’s approval.
Contraindications for SC VDZ include hypersensitivity to active substances or excipients. Patients with active infections, such as tuberculosis, sepsis, cytomegalovirus, listeriosis, and opportunistic infections (including progressive multifocal leukoencephalopathy), should avoid VDZ injection.
Limited data is available for special populations. Dose adjustment is not necessary in older patients. As a precaution, women of childbearing age are advised to use effective contraception during SC VDZ treatment and for at least 18 months after the last injection and should preferably not use SC VDZ during pregnancy unless the benefits clearly outweigh the risks.
Effectiveness of SC VDZ
Randomized controlled trials
The efficacy of SC VDZ maintenance treatment for UC and CD was demonstrated through two randomized, double-blinded, placebo-controlled phase III trials (VISIBLE 1 and 2).19,20 The study included patients aged 18–80 years with moderate to severe UC (VISIBLE 1) and CD (VISIBLE 2) who exhibited inadequate response, loss of response, or intolerance to conventional therapy or anti-TNF agents.
After a 28-day screening period, patients with UC and CD were administered open-label 300 mg IV VDZ at weeks 0 and 2, respectively. At week 6, patients were assessed for clinical response, defined as a decrease in the Mayo score of ⩾3 points and ⩾30% from baseline, along with a decrease in the rectal bleeding subscore of ⩾1 point or an absolute rectal bleeding subscore of ⩽1 in patients with UC, and a reduction in the CD Activity Index score of ⩾70 points from baseline in patients with CD. Patients with UC who achieved a clinical response were randomized in a 2:1:1 ratio into three groups: SC VDZ (108 mg SC VDZ Q2W along with IV placebo Q8W), IV-VDZ (300 mg IV VDZ Q8W along with SC placebo Q2W), and placebo (SC placebo Q2W and IV placebo Q8W). Patients with CD who achieved a clinical response were randomized in a 2:1 ratio into two groups: SC VDZ (108 mg SC VDZ Q2W) and placebo (SC placebo Q2W). Patients who did not achieve a clinical response at week 6 were administered a third open-label 300 mg IV VDZ dose at week 6 and were reassessed for clinical response at week 14. Those who achieved a clinical response at week 14 were eligible to enroll in the open-label extension study (VISIBLE OLE), 21 and those who did not were excluded (Figure 2).
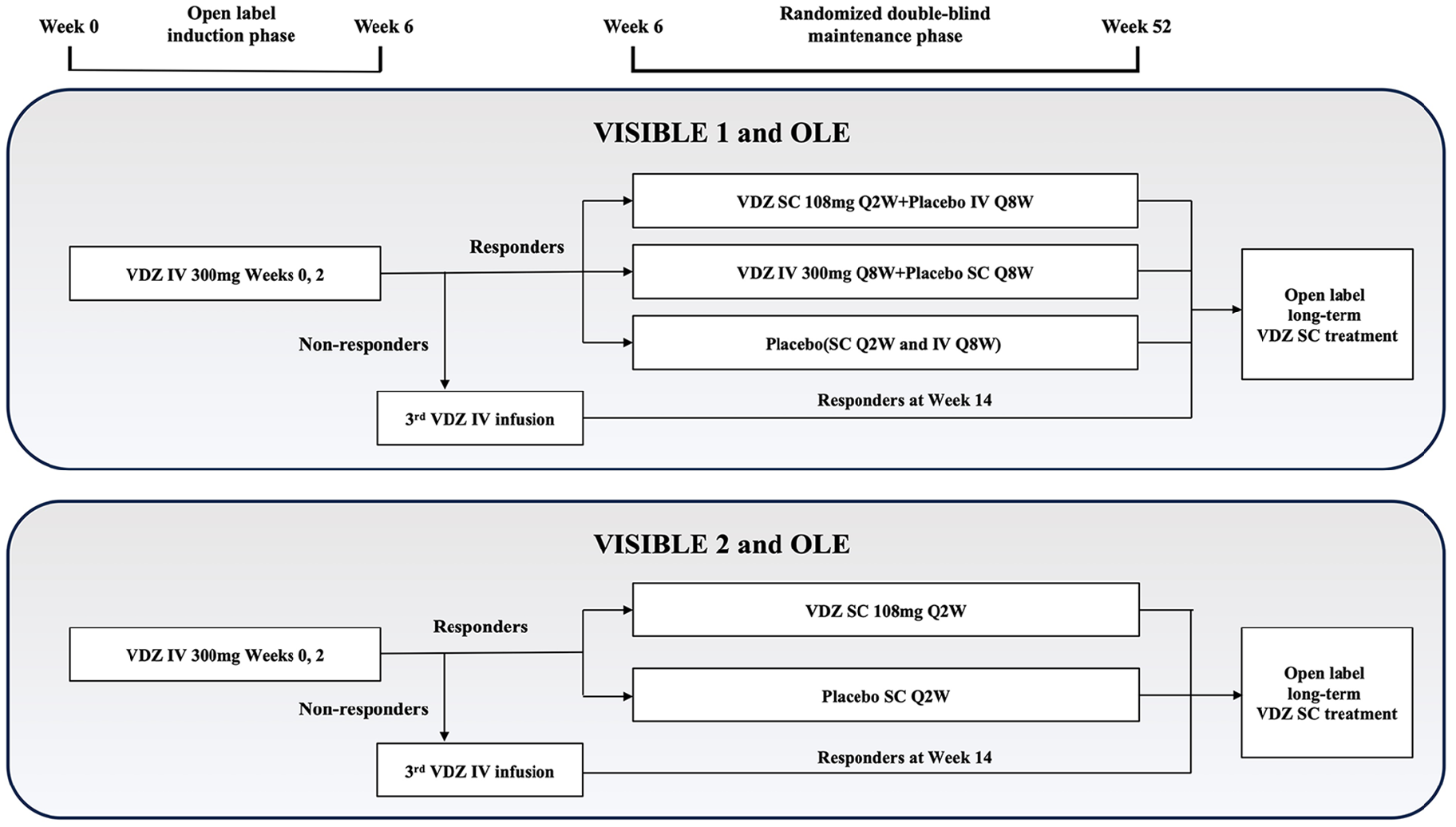
Design of the VISIBLE 1, 2, and OLE studies in ulcerative colitis and Crohn’s disease.
SC VDZ is effective as a maintenance therapy in patients with UC. Clinical outcomes, defined by clinical remission and durable clinical response at week 52, were significantly higher in patients receiving SC VDZ than in those receiving placebo (p < 0.001 for both). Although the durable and CS-free clinical remission rates did not differ significantly between the two groups, they were numerically greater in the SC VDZ group than in the placebo group. Patients who received SC VDZ were more likely to show endoscopic improvement and remission at week 52 than those receiving the placebo (p < 0.001 and p = 0.014, respectively) (Table 1). As an inflammatory biomarker, fecal calprotectin (FC) was normal (⩽250 μg/g) in 69.4% and 44.4% of the patients who received SC VDZ and placebo, respectively, whereas the proportion of normal FC was 8.8% and 8.9% in the two groups at baseline. 19 SC VDZ improved patient-reported outcomes after IV VDZ induction therapy. The Inflammatory Bowel Disease Questionnaire (IBDQ) and the EuroQoL-5D visual analog scale (EQ-5D VAS) scores improved significantly from baseline with SC VDZ compared to placebo (p ⩽ 0.001 for both). Similarly, improvements in Work Productivity and Activity Impairment-UC (WPAI-UC) scores were consistently greater in the VDZ SC group than in the placebo group. 22
Outcomes in patients with ulcerative colitis and Crohn’s disease treated with SC VDZ or placebo at week 52.

SC, subcutaneous; VDZ, vedolizumab; CS, corticosteroids; NA, not available; CDAI, Crohn’s Disease Activity Index; PRO, patient-reported outcomes; CRP, C-reactive protein.
In patients with CD, SC VDZ was also effective as a maintenance therapy. Higher rates of clinical remission and CS-free clinical remission occurred with SC VDZ than with placebo at week 52 (p = 0.008 and p = 0.002, respectively). The proportion of patients with an improved clinical response at week 52 was 52.0% with SC VDZ and 44.8% with placebo, although the differences were not statistically significant. In patients with C-reactive protein (CRP) levels >5 mg/l at baseline, 23.2% and 17.5% of patients in SC VDZ and placebo, respectively, reached CRP ⩽5 mg/l at week 52. Similarly, the proportion of patients with FC ⩽250 μg/g at week 52 was higher among patients receiving SC VDZ than in those receiving placebo 20 (Table 1). Furthermore, a higher quality of life and greater work productivity were maintained during SC VDZ versus placebo by evaluating the IBDQ, EQ-5D VAS, and WPAI-CD scores. 23
The VISIBLE OLE group comprised three groups of patients from the VISIBLE 1 and 2 trials. 21 One group included patients who had completed the 52-week maintenance period (randomized completers), and the other group included patients who were not randomized into the maintenance period and achieved response at week 14 after receiving a third IV VDZ infusion at week 6 (non-randomized week 14 responders). These groups of patients received SC VDZ 108 mg Q2W in the VISIBLE OLE trial and increased to QW after treatment failure (Figure 2). The third group included patients who retired early from the maintenance period owing to treatment failure and received SC VDZ 108 mg QW in the VISIBLE OLE trial.
The ongoing VISIBLE OLE trial is expected to be completed by January 2024. Based on the interim results of patients with UC, clinical remission [defined as a partial Mayo score (PMS) of ⩽2 and no subscore of >1] rates were maintained from weeks 6 to 108 in VISIBLE 1 randomized completers (64.5–67.0%) and from weeks 14 to 110 in VISIBLE 1 non-randomized week 14 responders (62.6–33.3%). CS-free clinical remission rates were maintained in VISIBLE 1 randomized trial completers from weeks 52 to 108 (from 73.3% to 69.2%) and in non-randomized week 14 responders from weeks 54 to 110 (from 24.5% to 25.0%). 21
Real-world studies
We searched for a combination of subject and free words, including ‘vedolizumab’ and ‘subcutaneous’, in the PubMed, Web of Science, and Embase databases. Finally, we included nine articles, five conference abstracts, and one letter, totaling 15 RWS,24–38 with 14 reporting on the effectiveness of SC VDZ as maintenance therapy (Table 2).
Real-world studies of SC VDZ in IBD.

SC, subcutaneous; VDZ, vedolizumab; IBD, inflammatory bowel diseases; CD, Crohn’s disease; UC, ulcerative colitis; IBDU, inflammatory bowel disease unclassified; HBI, Harvey Bradshaw Index; SCCAI, Simple Clinical Colitis Activity Index; CRP, C-reactive protein; FC, fecal calprotectin; AE, adverse event; ISR, injection site reaction; SAE, serious adverse event; CS, corticosteroids; PMS, partial Mayo score; IQR, interquartile range; NA, not available.
In clinical evaluations, the Harvey Bradshaw Index (HBI) was used as the disease activity score in all CD patients, and an HBI score of ⩽425,26 was defined as clinical remission. Changes in the HBI before and after the switch were reported in five studies,24–28 none of which showed significant differences. For patients with UC, Simple Clinical Colitis Activity Index (SCCAI) or PMS was used as the disease activity score in the studies, and clinical remission was defined as SCCAI ⩽225,26 or PMS ⩽1.27,28 Changes in the SCCAI or PMS before and after the switch were reported in five studies,24–28 with no observed significant differences except in one study that showed a decrease in the SCCAI. 25 Six studies24,25,27–30 compared the proportion of patients in clinical remission before and after the switch, with no significant differences observed except in one study, which showed more patients in clinical remission at week 20 compared to the time of the switch. 30
In terms of biochemical evaluations, eight studies24–28,30,32,35 documented changes in FC before and after switching. Among them, six25–28,30,32 did not show significant changes, one indicated a decrease in FC, 35 and one reported a dose increase from 31 to 47 g/g. 24 The clinical significance of the slight increase in FC was restricted owing to its small value. Eight studies reported changes in the CRP levels24–28,30,32,35 before and after switching, with no significant alterations observed. Different studies have variably defined biochemical remission, commonly relying on CRP ⩽5 mg/l and/or FC ⩽250 g/g.26,27 Five studies25,27–30 compared the proportion of biochemical remission before and after switching, with no significant difference between the two timepoints except in one study that showed more patients in biochemical remission at week 20 compared to the time of the switch. 30
Questions related to efficacy
Is QW better than Q2W?
Two distinct patient groups underwent dose escalation in the VISIBLE 1 and VISIBLE OLE trials. The first group comprised VISIBLE 1 randomized completers who entered VISIBLE OLE on a Q2W VDZ dosing regimen and escalated to QW owing to disease exacerbation. The second group included patients randomly assigned to SC VDZ Q2W during VISIBLE 1 maintenance therapy but withdrew early and received SC VDZ QW in VISIBLE OLE owing to treatment failure. After 16 and 48 weeks of escalated dosing, 27.1% (13/48) and 10.8% (4/37) regained clinical remission, respectively, 39 suggesting that transitioning from Q2W to QW restored treatment response for certain patients.
Does a longer duration of IV VDZ prior to the switch lead to better outcomes of SC VDZ?
The efficacy of SC VDZ was evaluated across three groups based on the duration of IV VDZ infusions before transitioning to SC VDZ. Group 1 included patients achieving clinical response at week 6, who then received SC VDZ maintenance therapy in the VISIBLE 1 (two IV infusions) trial. Group 2 included non-randomized week 14 responders (three IV infusions). Group 3 included patients achieving clinical response at week 6, receiving IV VDZ maintenance therapy in VISIBLE 1, and later transitioning to SC VDZ in the VISIBLE OLE (eight IV infusions) trial. Clinical remission rates were 46.2% (49/106) for Group 1 at week 52, 39.2% (40/102) for Group 2 at week 54, and 77.1% (27/35) for Group 3 at week 52. The clinical remission rate of Group 3 persisted at 76.9% (10/13) during VISIBLE OLE through week 76. 40 In an RWS by Lim et al., 31 the duration of prior VDZ treatment did not affect drug discontinuation, adverse events (AEs), CS use, or IBD-related hospitalizations. These studies showed that the efficacy of SC VDZ was independent of the duration of IV VDZ treatment.
Can SC VDZ be interrupted?
Among patients who received a placebo in VISIBLE 1, some completed 52 weeks of treatment before entering the VISIBLE OLE (with 46 weeks of interruption) trial, whereas others withdrew early owing to disease worsening and entered VISIBLE OLE (with interruptions ranging 1–45 weeks). Those discontinuing at 46 weeks showed a clinical remission rate of 52.6% at week 0 in VISIBLE OLE, increasing to 85.7% after 24 weeks. Among patients discontinuing at 1–45 weeks, the clinical remission rate was 9.4% at week 0 and 54.2% after 24 weeks. 41 This suggests that patients who respond to initial IV VDZ induction therapy may benefit from restarting SC VDZ therapy following treatment interruption. In clinical practice, promptly resuming SC VDZ therapy after interruption is recommended, followed by Q2W dosing.
First- or second-line treatment choice?
Regardless of prior anti-TNF treatment, SC VDZ demonstrated higher clinical remission rates than placebo at week 52 in VISIBLE 1 (anti-TNF-naïve, p < 0.001; anti-TNF failure, p = 0.023). 19 In patients with a previous history of anti-TNF failure in VISIBLE 2, SC VDZ also exhibited higher clinical remission rates at week 52 (46.4% versus 28.8%; p = 0.019). However, patients without anti-TNF treatment history had clinical remission rates of 42.9% and 48.6% in the placebo and SC VDZ groups, respectively, with no significant difference (p = 0.591). 20 This suggests that SC VDZ is effective as either a first- or second-line treatment in patients with UC and recommended as a second-line treatment in patients with CD.
Optimized IV infusions better than standard?
Optimized IV infusions involve shortening intervals during IV infusions from once Q8W to once Q4W. In an RWS conducted by Bergqvist et al., 25 20 patients received optimized IV VDZ dosing at baseline. After 6 months, this group remained stable in terms of FC, CRP, clinical remission rates, and biochemical remission rates. Meanwhile, patients receiving standard IV VDZ showed a statistically significant improvement in FC, with other outcome measures unchanged. Similarly, Pintar et al. 36 reported that 63 and 35 patients with IBD received standard and optimized IV VDZ, respectively, at baseline. After a median 40-week follow-up, clinical remission rates changed from 95.6% to 92% and 70.4% to 78.6% in the standard and optimized IV VDZ groups, respectively. These findings suggest similar clinical and biochemical outcomes in patients treated with standard or optimized therapies.
Which variables predict treatment efficacy?
A clinical decision support tool (CDST) was developed and validated to guide CD treatment decisions with IV VDZ. 42 To assess the predictive ability of CDST, patients with CD in the VISIBLE 2 trial were categorized as low/intermediate or high response probability based on the CDST. At week 6, 61.1% (99 patients) of high-probability patients achieved clinical remission compared to 33.9% (38 patients) in the low/intermediate-probability group. 43 While the CDST appears to differentiate clinical remission following SC treatment, McLean et al. 34 observed that there was no systemic inflammatory biomarker or demographic signature capable of predicting discontinuation of SC VDZ therapy. In addition, Volkers et al. 26 and Ribaldone et al. 32 could not identify any baseline factors associated with SC VDZ outcomes.
Safety and persistence of SC VDZ
In the RCTs,19,20 the safety profiles were similar for IV and SC VDZ treatment, except for injection site reactions (ISRs). Most AEs were of mild to moderate severity, and drug-related serious AEs occurred in 0.9% and 1.5% of UC and CD cases, respectively. The most common AE was worsening disease (14.2% for UC and 15.3% for CD). Other common AEs included nasopharyngitis, upper respiratory tract infections, headaches, arthralgia, and anemia. Regarding abdominal and gastrointestinal infections, the incidence of UC and CD was 4.7% and 4%, respectively, and a patient with CD developed a Clostridioides difficile infection during the follow-up period. The incidence of ISRs was elevated in SC VDZ, with a prevalence reaching 10.4% and 2.9% in the UC and CD groups, respectively, most of which were mild.
Among the RWS, 1024–32,38 provided safety data during follow-up, with ISRs occurring more frequently, ranging from 2.4% (4/168) 32 to 51.8% (43/83). 25 ISRs primarily present as pain, burning sensation, erythema, itching, and swelling. In one RWS, 25 38.5%, 51.8%, and 31.3% of patients reported pain, burning sensation, and erythema, respectively. Some patients switched to IV VDZ because of ISRs, and only one RWS 31 reported that 2 out of 12 patients who switched to IV VDZ developed angioedema reaction and left shin panniculitis, indicating potential allergies. Other AEs, including COVID-19, abdominal pain, headache, fatigue, arthralgia, and rash, exhibited safety profiles similar to those of IV VDZ. Furthermore, SC VDZ demonstrated a low incidence of serious AEs, with only three studies26,28,29 reporting 11 cases.
Long-term safety data for SC VDZ remain limited, with interim results from the VISIBLE OLE trial providing a 2-year follow-up data for UC. 21 The most common AEs included UC exacerbation (18%), nasopharyngitis (11%), upper respiratory tract infections (9%), and anemia (7%). ISRs occurred in 4.5% of patients, all of which were mild or moderate in severity.
Notably, SC VDZ exhibited a high treatment persistence rate across 15 RWS, ranging from 58.3% (14/24) 38 to 96% (381/397). 35 In these studies, reasons for discontinuation were predominantly related to disease worsening/loss of response, AEs, and ISRs.
Pharmacokinetics of SC VDZ
In the VISIBLE 1 trial, the median serum trough concentration (Ctrough) of SC VDZ exceeded that of IV VDZ during study visits. 19 Stratifying Ctrough of SC VDZ at week 46 by quartiles revealed increasing clinical remission rates at week 52, with higher Ctrough ranging from 50% (quartile 1) to 83% (quartile 4). Anti-VDZ antibodies (AVA) were detected in 6% (6/106) of SC VDZ recipients, similar to that observed for IV VDZ (3/54). Among AVA-positive patients, four were persistently positive, and three developed neutralizing antibodies. Subgroup analysis based on AVA positivity indicated that AVA reduced efficacy but not ISRs or hypersensitivity reactions. 44
Furthermore, for patients with UC, a study included data from four trials (VISIBLE 1, GEMINI 1, GEMINI 2, and VISIBLE OLE) and analyzed average serum drug concentrations using a population pharmacokinetic model. 45 SC VDZ 108 mg Q2W yielded similar average drug serum concentrations to those of IV VDZ 300 mg Q8W and lower than those of IV VDZ 300 mg Q4W.
In the VISIBLE 2 trial, the median Ctrough in the SC VDZ group increased from 27.5 µg/ml at week 6 to 30.2 µg/ml at week 46. 20 Similar to VISIBLE 1, clinical remission rates at week 52 for SC VDZ-treated patients rose with increasing Ctrough, from 37.7% (quartile 1) to 50.7% (quartile 4). Among 275 SC VDZ-treated patients, AVA was detected in seven (7/275), with three being consistently AVA-positive and four having neutralizing antibodies, similar to those previously reported for IV VDZ. Among AVA-positive patients, 71.4% (5/7) did not achieve clinical remission at week 52, signifying the impact of AVA on treatment efficacy. However, AVA was not associated with ISRs or hypersensitivity reactions. 46
VDZ concentrations were assessed at the time of the switch and after SC VDZ use in seven RWS.24–28,30,36 All reported elevated concentrations after the switch, with three showing statistically significant elevation. Moreover, the RWS by Ventress et al. 24 found no AVA after SC VDZ administration.
Notably, an RWS explored the therapeutic drug monitoring (TDM) of SC VDZ. 28 VDZ concentrations were regularly measured during infusions at this center, with intervals adjusted to maintain VDZ concentration >20 mg/l. Owing to differing IV infusion intervals, SC injection intervals required adjustments following the algorithm for transitioning to SC VDZ. Median intervals were 7 weeks between IV injections, 13 days between SC injections, and 26 weeks post-switch.
Patient satisfaction with SC VDZ
Several RWS indicated high patient satisfaction with SC VDZ, often citing simplicity and convenience as key factors. 24 Bergqvist et al. 25 reported that most patients favored SC over IV treatment (83.3%). In addition, patient preferences shifted after using SC VDZ, as observed by Wiken et al., 28 who reported that the percentage choosing SC injections increased from 28.0% at baseline to 59.4% at 26 weeks.
Preferring SC treatment was attributed to ease of administration, occupational–social flexibility, and reduced time commitment. By contrast, reasons for patient reluctance toward SC included concerns about efficacy loss, reduced medical follow-ups, higher administration frequency, self-administration, and reduced physician monitoring. Numerous studies are presently investigating factors impacting patient preference for SC treatment. At the University Hospital of Nancy, 47 a multifactorial analysis revealed a link between shorter treatment duration and greater SC acceptance. Studies at the Imelda General Hospital in Bonheiden 48 helped identify younger age as the sole independent factor through multivariate analysis. Notably, electronic alerts, information brochures, and personalized teaching moments proved beneficial for patients with SC treatment uncertainties. Nurses play a pivotal role in these interactions. De Dycker et al. 49 conducted a multicenter study and reported that face-to-face interactions with IBD nurses, as opposed to e-health applications, improved patient preference for SC treatment.
Economics of SC VDZ
Transitioning from IV to SC formulations presents notable economic advantages. In the UK, the net drug acquisition cost of a standard SC dose is comparable to that of a standard IV dose. Using a model built from an RWS cohort, annual drug acquisition costs are projected to reduce by £357,000 per 100 transitioning patients, with additional cost savings from reduced IV administration, estimated at approximately £104,000. 24 Similarly, Sweden reported a 15.0% lower annualized cost for SC maintenance treatment relative to IV, considering drug costs, IV infusion administration fees, and dose optimization. 25
In France, a decision-analysis model, reflecting a payer’s perspective over 5 years, evaluated the budget impact of SC VDZ as maintenance therapy for UC by subtracting outcomes of ‘a world without SC VDZ’ from ‘a world with SC VDZ’. Results indicated total cost savings of €59,176,842 for biologic-naïve patients and €2,004,135 for biologic-experienced patients relative to a scenario without SC. 50 From the payer’s perspective, Canada evaluated the cost-effectiveness of SC VDZ versus traditional and advanced treatments in patients using a hybrid decision tree/Markov model. Among advanced treatments, SC VDZ emerged as the most cost-effective, offering an annual cost reduction of $2120 per patient compared with IV VDZ. 51
Conclusion and future perspectives
Based on clinical trials and ongoing RWS, transitioning from IV VDZ to SC VDZ in patients with IBD maintains clinical, biochemical, and patient-reported outcome remission while being well tolerated and largely free of new safety signals besides ISRs. However, data regarding SC VDZ in special populations, such as adolescents, women of childbearing age, pregnant women, and those with liver or kidney disease, remain limited. In addition, present SC VDZ follow-up remains relatively short, and study sites are predominantly in Western countries such as the United States, the United Kingdom, and Sweden. Endoscopy before and after treatment has only been performed in patients with UC in the VISIBLE 1 study, while in the VISIBLE 2 study, only the SC VDZ and placebo groups were included, omitting the IV VDZ group, thus hindering direct comparison of IV VDZ and SC VDZ outcomes during the maintenance period. Consequently, future studies must include longer follow-up periods, larger sample sizes, broader geographical representation, and increased direct comparison between IV infusions and SC injections. Furthermore, including endoscopic assessment of efficacy, particularly endoscopic remission, as a long-term therapeutic objective for patients with IBD is pivotal (Table 3).
Prospects and gaps of SC VDZ in inflammatory bowel disease.

SC, subcutaneous; VDZ, vedolizumab; IV, intravenous; TNF, tumor necrosis factor index; CD, crohn’s disease; TDM, therapeutic drug monitoring.
Various treatment regimens have been employed in different clinical studies. Before SC VDZ, the duration of IV VDZ varied; however, all patients received at least two infusion doses, with IV VDZ intervals ranging from 4 to 8 weeks. Initial investigations of different IV VDZ durations and intervals among patients transitioning to SC VDZ post-treatment indicated no correlation with outcomes. Furthermore, the FDA announced that VDZ could be switched to SC injection at week 6 following the first two VDZ IV doses administered at week 0 and week 2. In addition, in cases of disease exacerbation during SC VDZ therapy, clinical remission may be restored by shortening the SC interval or switching to IV VDZ or other biological agents. Post hoc analyses of RCTs revealed that shortening the SC interval may restore clinical remission in some patients; however, the effectiveness after switching therapy requires further investigation.
Individualized treatment of patients with different baseline characteristics is a trend for future development. IV VDZ guidelines recommend its use as a first- or second-line treatment. Post hoc analysis in RCTs revealed that SC VDZ was more effective than placebo as either a first- or second-line treatment option in patients with UC and resulted in higher clinical remission rates than placebo when used as a second-line treatment in patients with CD; however, subgroup analysis was not performed in RWS. Meanwhile, in patients with perianal CD, an RWS reported that 3/10 patients had active perianal disease at baseline, whereas, after the switch, only two patients had this condition at follow-up. However, owing to limited data, the effectiveness of SC VDZ in perianal CD requires further exploration. Furthermore, the CDST has undergone validation for efficacy prediction in IV VDZ and has demonstrated equal applicability in the VISIBLE 2 trial. However, in RWS, no predictive variables of disease outcomes were identified, and CDST was not used for predicting efficacy. Therefore, this conclusion should be approached with caution.
SC VDZ demonstrates an exposure–response relationship and low immunogenicity. In the RWS, drug optimization was conducted using TDM, and the persistence rate was 92.6% at week 26. However, the utility of TDM in optimizing SC VDZ treatment and determining optimal drug concentration for targeted treatment remains a subject for further investigation.
Collectively, SC VDZ is effective, safe, cost-effective, and yields high patient satisfaction. However, patient reluctance toward SC administration owing to fear of needles or reduced physician interaction underscores the importance of nurse–physician collaboration to enhance patient acceptance of SC VDZ. Strategies may include informational brochures, physician/nurse–patient face-to-face communication prior to treatment, and ongoing email or telephone contact during the treatment process. As more studies are conducted, the role of SC VDZ in IBD treatment will become clearer.
Supplemental Material
sj-docx-1-taj-10.1177_20406223241247648 – Supplemental material for Take vedolizumab home: transition from intravenous to subcutaneous treatment
Supplemental material, sj-docx-1-taj-10.1177_20406223241247648 for Take vedolizumab home: transition from intravenous to subcutaneous treatment by Kaituo Huang, Lingya Yao, Jing Liu and Qian Cao in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.