
Abstract
Background:
Fecal microbiota transplantation (FMT) is a promising treatment for active ulcerative colitis (UC). Understanding patient preferences can identify treatment features that may impact treatment decisions, improve shared decision-making, and contribute to patient-centered care, which is especially important in the context of novel treatments like FMT.
Objectives:
We aimed to quantify preferences for active UC treatments, specifically FMT and biologics, and identify patient characteristics associated with different preference patterns.
Design:
This is a cross-sectional survey study.
Methods:
We administered a discrete choice experiment (DCE) survey to elicit preferences in a sample of Canadian adults with UC. DCE data were analyzed using a main-effects mixed logit model and used to predict uptake of hypothetical scenarios reflecting alternative combinations of treatment features. Latent class modeling identified heterogeneity in patient preference patterns.
Results:
Participants’ (n = 201) mean age was 47.1 years (SD: 14.5 years), 58% were female, and most (84%) had at least some post-secondary education. Almost half were willing to undergo FMT. When considering treatments for active UC, the most important attributes were chance of remission and severity of rare unknown side effects. All else equal, participants were most likely to uptake treatment that involves oral capsules/pills. Participants in the class with the highest utility for chance of remission were younger, had more severe disease, and 58% indicated that they would be willing to undergo FMT.
Conclusion:
We identified characteristics of UC patients who are more likely to be interested in FMT using preference elicitation methods. Patient-centered care can be enhanced by knowing which patients are more likely to be interested in FMT, potentially improving satisfaction with and adherence to treatments for active UC to maximize the effectiveness of treatment while considering heterogeneity in patient preferences.
Plain language summary
Background and aims:
Fecal microbiota transplantation (FMT) is a promising new treatment for active ulcerative colitis. Questions remain around the benefits and risks of FMT treatment for patients with ulcerative colitis. Understanding how patients weigh the treatment features and how treatment features influence their decisions may improve shared decision-making and contribute to patient-centered care, which is especially important for novel treatments like FMT.
Using an experimentally designed survey, we aimed to:
1. Elicit patient preferences for features of active ulcerative colitis treatments, specifically FMT and biologics; and,
2. Identify patient characteristics associated with different preference patterns.
Results:
We found that younger patients with more severe disease are more likely to try FMT for the treatment of active ulcerative colitis. Oral capsules/pills are the preferred mode of treatment administration.
Conclusions:
These findings can enhance patient-centered care by characterizing patients who are more likely to be interested in FMT. Aligning treatment with the features that are important to patients can potentially improve satisfaction with and adherence to treatments for active ulcerative colitis to maximize their effectiveness for individual patients.
Introduction
There are several widely accepted and emerging therapies for the treatment of ulcerative colitis (UC). The main treatment targets for UC are symptom relief (short-term), clinical remission, and mucosal healing (long-term). 1 Individuals with UC may need to undergo multiple treatments to achieve these goals, and some may need to transition to a new treatment if they experience disease relapse. 2 Treatments for active UC are selected based on a variety of clinical factors such as disease location, severity and response, and most commonly include aminosalicylates (5-ASA), corticosteroids, immunosuppressants, targeted synthetic small molecules, and biologic therapies. 2
An emerging treatment option for persons with active UC is fecal microbiota transplantation (FMT). FMT involves the transfer of human microbiota using stool from a healthy donor into a patient, with the goal of treating gut microbial dysbiosis. FMT has proven to be effective in the treatment of recurrent Clostridium difficile infections (rCDI)3,4 and, more recently, has shown promise as treatment for active UC.5–8 Although there are both positive and negative randomized trials, the overall signal from systematic reviews is that FMT is likely effective at inducing remission for active UC.5–8 While generally considered safe, FMT has been linked to infectious transmissions, prompting safety warnings and regulation.9–12 In the United States, for example, FMT is regulated by the Food and Drug Administration (US FDA) as a biological agent, and the use of FMT to treat rCDI is under enforcement discretion. 13 The use of FMT for other indications, such as UC, requires the Investigational New Drug application with the FDA.
FMT has generated interest among adults with UC, with previous qualitative and mixed-methods research exploring attitudes toward FMT as a treatment for UC and Crohn’s disease finding that adults are receptive to and willing to try FMT as a treatment.14–18 Understanding patient preferences toward treatments for UC can help identify features of treatments that are most important to patients and potentially support shared decision-making and patient-centered care. 19 Ultimately, this could contribute to improving treatment satisfaction and adherence. 20 In the context of preference-sensitive choices such as novel treatments like FMT, 21 this is particularly important, especially with the recent FDA approval of the first FMT product, which once commercially available can be prescribed for off-label use, such as for treatment of active UC. 22 While there has been research on patient attitudes and perceptions toward FMT, to our knowledge, studies have not explored benefit-risk trade-offs to quantitatively estimate the utility (value) of FMT as a treatment for active UC. Discrete choice experiments (DCEs) are a stated preferences method grounded in economic theory that can be used to estimate the utility of different features or attributes of a treatment or healthcare intervention. The higher the utility, the higher the preference for a particular treatment attribute relative to others and the greater the effect on the treatment decision. 20 Parameter estimates from DCEs can be used to predict uptake of new treatments relative to current treatments.
We conducted a survey with a DCE in a sample of adults with UC to: (1) quantify preferences for treatments for active UC, specifically estimating preferences for treatments with features that reflect FMT and biologics; and (2) determine patient characteristics associated with different patterns of preferences.
Materials and methods
Study sample
We administered an online survey to a sample of Canadians with UC (>18 years) enrolled in the Inflammation, Microbiome & Alimentation Gastro-Intestinal & Neuropsychiatric Effects (IMAGINE) Chronic Disease Network’s Mind and Gut Interactions Cohort (MAGIC) study. 23 Participants with UC who had agreed to be contacted for future research were recruited for the online survey by email from four IMAGINE Chronic Disease Network sites. Nonresponders were emailed two reminders to participate. Survey information and instructions for how to participate were included in the recruitment emails.
Ethics approval and consent to participate
The University of Calgary Conjoint Health Research Ethics Board (REB17-2460), the University of Alberta Health Research Ethics Board (Pro00100546), the University of Manitoba Research Ethics Board [HS22526 (H2019:050)], and McMaster University Hamilton Integrated Research Ethics Board (10862) approved this study. Informed consent (written) was obtained from all individual participants included in this study.
Study design
We conducted a cross-sectional survey study. A DCE was included in the survey to estimate the utility associated with different features of UC treatments. In DCEs, respondents evaluate a series of alternative scenarios described by specific attributes (treatment features) over a series of questions (choice tasks) and are asked to choose the scenario they prefer (example in Figure 1). 20 Respondent preferences can be estimated from DCE data and expressed as utilities. Respondents’ value for different attributes of treatment can be derived from the estimated utility, and the estimated coefficients reflect participants’ relative preferences; higher utility indicates higher value.

Example of discrete choice experiment choice task completed by participants.
Attribute development in our DCE was informed by previous research by members of our research team (DAM, GGK, GH, RP), 24 literature review, feedback from our IMAGINE Chronic Disease Network Patient Research Partners, and feedback from gastroenterology clinical experts on our research team (DK, CNB, GGK, HJ, RP, YN, MR, PM). Although FMT is a novel treatment for active UC, we used published findings from clinical trials and guidance from clinical experts on our research team to identify relevant attributes and levels. Following good research practice, we pretested and pilot tested the survey.25,26 A draft of the survey was pretested with IMAGINE MAGIC study participants (n = 6) from the University of Calgary site. Pretesting was done using one-on-one cognitive interviews to assess understanding of the survey including background information, all non-DCE questions and the DCE (attributes and levels), as well as overall feedback on survey content, length and cognitive burden. 25 The survey was updated based on results of pretesting then pilot tested online with an additional sample of IMAGINE MAGIC study participants (n = 31) from the University of Calgary site. Pilot testing allowed for a quantitative assessment of DCE performance, online survey performance and length of survey.
After modifications based on pilot testing, the final DCE included four attributes with three to four levels each that reflect both FMT and biologics (tumor necrosis factor inhibitors): (1) chance of (clinical) remission; (2) severity and chance of known side effects; (3) severity of rare unknown side effects; and (4) what treatment would involve (Table 1). What treatment would involve compared two common modalities of administering FMT (i.e. capsule ingestion or rectal enema) to two routes of dosing a biologic (i.e. injection or intravenous infusion). In addition to the DCE, the final survey included the following components: (1) screening questions; (2) background information about inflammatory bowel disease (IBD) and UC; (3) disease experience questions (current disease status, year of diagnosis, attitudes about their medications); (4) background information about FMT; (5) attitudes toward FMT (questions adapted from survey by Kahn et al. 16 ); (6) Short Inflammatory Bowel Disease Questionnaire [SIBDQ; measures quality of life using 10 items and is scored from 10 (poor quality of life) to 70 (optimum quality of life); use of the SIBDQ, authored by Dr. Jan Irvine et al., was allowed under license from McMaster University, Hamilton, Canada]; 27 and (7) participant demographics.
Summary of attributes and levels included in the DCE.

Denotes reference level.
DCE, discrete choice experiment.
Following good practice in DCE experimental designs, 28 we used Ngene software 1.2.1 (ChoiceMetrics, Australia) to generate a d-efficient design, based on a multinomial logit model, with 24 choice tasks and two blocks (12 choice tasks per block). We selected a design based on low MNL d-error and minimal correlation. Each choice task was unlabeled (i.e. Treatment A, Treatment B) and included two alternatives. We used a dual-response choice format, whereby participants first completed a forced-choice task followed by a question which allowed participants to state they would not choose either of the alternatives described in the choice task (Figure 1). In addition to the 12 experimental choice tasks per block, we included three nonexperimental choice tasks to test internal validity of the DCE: stability test (repeated choice task), within-set dominated pairs test (choice task with one alternative that was unambiguously ‘better’ than the other for all ordered attribute levels and the level oral capsule/pill for the unordered attribute) and a forced trade-off task (choice task with two attribute levels held constant, forcing participants to make trade-offs between the other attribute levels). Internal validity tests are used in DCEs to assess participant choice logic, response consistency, participant trade-offs and validity and reliability of participant choices. 29 Data from nonexperimental choice tasks are not included in the analysis of parameter estimates. Overall, participants completed 15 choice tasks for the DCE component of the survey. In DCEs, the sample size for robust estimates is influenced by the number and complexity (number of attributes, levels, and nature of the attributes/levels (i.e. probabilistic attributes)) of choice tasks.28,30,31 Based on the number of experimental choice tasks (24 total) and attributes (four with 3–4 levels each, two probabilistic), a sample size of 200 participants was the estimated minimum required to achieve an acceptable level of statistical precision (standard error less than 0.05 for each attribute) and to investigate heterogeneity.
Statistical methods
Descriptive statistics were used for all non-DCE questions (disease experience questions, attitude questions, SIBDQ, and demographics). Data from the DCE were analyzed using a main-effects (no interactions) mixed logit model to estimate the utility function and obtain overall estimates of utility for each attribute level.32,33 Mixed logit models account for heterogeneity of preferences by using probability distributions and a mean and standard deviation of the preference distribution for each attribute level is estimated.32,33 We assumed that preferences were randomly distributed and that all parameters followed a normal distribution. We used 1000 Halton draws for the mixed logit model simulations. All attributes were categorical and dummy coded so that the estimated parameters are relative to the reference attribute level denoted in Table 1. The opt-out question was considered a third alternative. More details on the statistical methods for the DCE are available upon request.
Predicted uptake of hypothetical treatment scenarios reflecting alternative combinations of treatment features (defined in Table 2 with guidance from gastroenterology clinical experts on our research team) was assessed using relative probability of uptake rates. Predicted uptake of hypothetical treatment scenarios also serves as a sensitivity analysis providing insight into the effect of changes in attributes levels on probability of uptake. Participants are assumed to choose a treatment alternative if the utility derived is greater than the utility derived from the other alternative. To identify heterogeneity in patterns of preferences in our sample, we used a latent class conditional logit model. 34 In a latent class model, class membership is the probability of a participant being in a class based on characteristics of the participant. The number of classes is determined in an iterative procedure by assessing model performance after the addition of a class. We estimated posterior probability of class membership for each participant and assigned each participant to the class to which they had the highest probability of belonging.
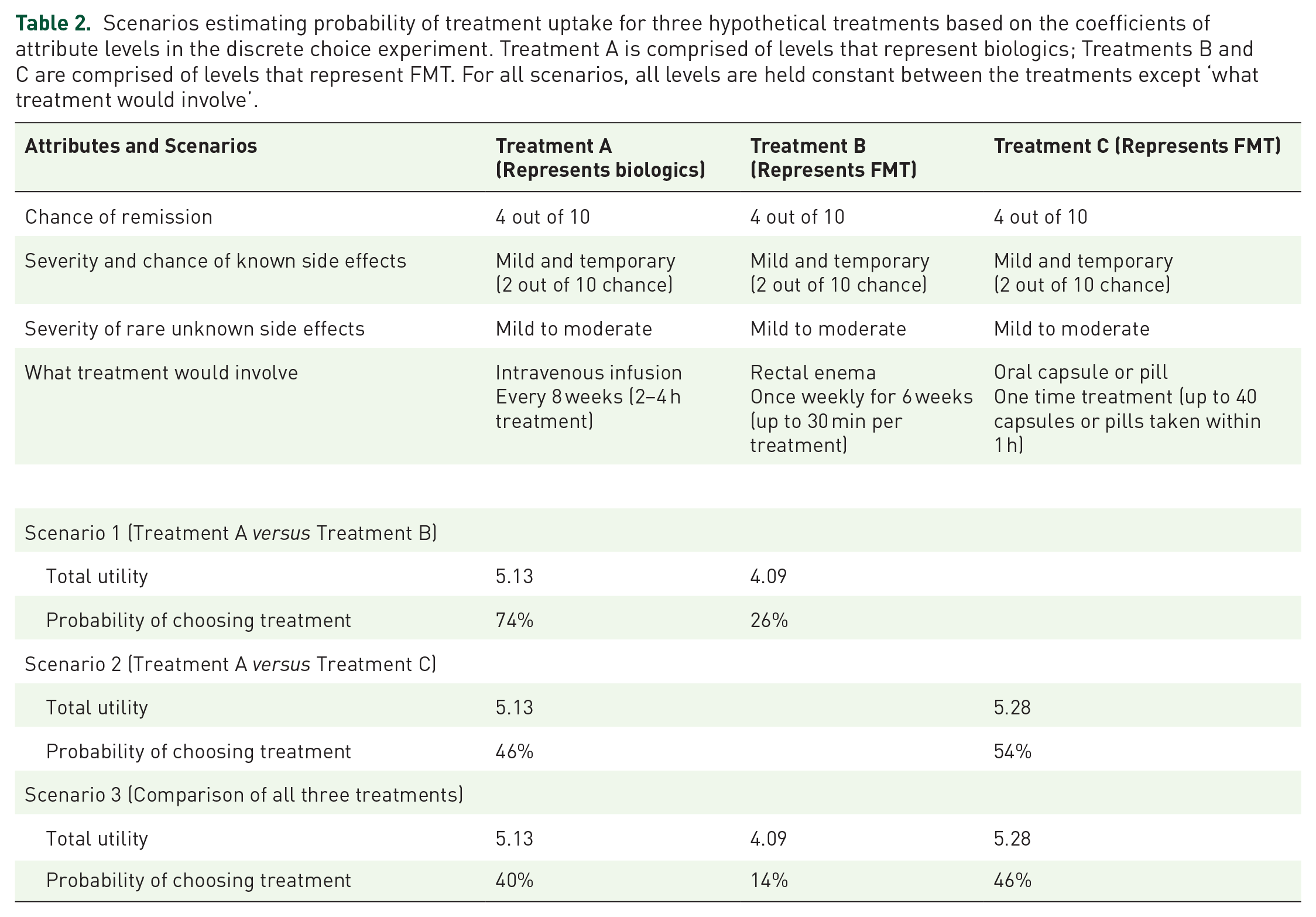
Scenarios estimating probability of treatment uptake for three hypothetical treatments based on the coefficients of attribute levels in the discrete choice experiment. Treatment A is comprised of levels that represent biologics; Treatments B and C are comprised of levels that represent FMT. For all scenarios, all levels are held constant between the treatments except ‘what treatment would involve’.
For all models, model performance goodness-of-fit was assessed using log-likelihood ratios, Akaike information criterion (AIC) and Bayesian information criterion (BIC). Attribute levels with a p value < 0.05 were statistically different from the reference level. If the 95% confidence intervals (CIs) of an attribute level overlap with another level within that attribute, they are not statistically different from each other. All analyses were performed using Stata SE 16.1 (College Station, TX, USA). 35
Results
Participant characteristics and experiences
Overall, 478 recruitment emails were sent across the four sites, n = 237 people started the survey (50% response rate) and n = 201 fully completed the DCE (42% completion rate). Participants (n = 201) were an average of 47.1 years old (SD: 14.5 years), 58% female gender, and highly educated (84% with at least some post-secondary education). The mean age at UC diagnosis was 31.8 years (SD: 13.3 years) and the mean disease duration (time since UC diagnosis) was 15.4 years (SD: 11.1 years). In Canada, most individuals with UC are diagnosed between age 20 and 30 years and UC is diagnosed more commonly than Crohn’s disease in those older than 65 years. 36 Further, women are equally as likely to be diagnosed with UC as men. 36 Most participants reported their current disease status at the time of completing the survey as ‘remission’ (71%). Participants’ mean SIBDQ score was 52.4 (SD: 11.3). When asked if their current health depends on their UC medications, 69.5% (n = 140) agreed or strongly agreed (Table 3).
Participant characteristics (n = 201).

SIBDQ is scored from 10 (poor quality of life) to 70 (optimum quality of life).
For these characteristics, total n = 200 due to n = 1 participant not completing the demographic component of the survey.
CAD, Canadian dollars; SD, standard deviation; SIBDQ, Short Inflammatory Bowel Disease Questionnaire.
Attitudes toward FMT
When asked if they would be willing to undergo FMT as a treatment for their UC, given what they know about FMT, 47.8% (n = 96) of participants said yes, 40.8% (n = 82) said unsure and 11.4% (n = 23) said no. Participants ranked preferred sources of fecal matter for FMT and the top choice was an anonymous donor (41.3%, n = 83), followed by a family member (31.8%, n = 64). Participant attitudes regarding the ‘ick factor’ associated with using a treatment involving fecal matter were divided with 41.3% (n = 83) indicating it was moderately important/important/very important and 40.3% (n = 81) indicating it was moderately unimportant/unimportant/very unimportant. The remaining 18.4% (n = 37) were indifferent (Table 4).
Participant attitudes toward FMT.

Source: Questions adapted from survey by Kahn et al. 16
Overall DCE results
Chance of (clinical) remission was the most important treatment attribute with the highest utility to participants, followed by severity of rare unknown side effects, as defined for participants in Table 1. The magnitude of the coefficients and utility for severity and chance of known side effects and what treatment would involve were similar. For each attribute, all levels were statistically different (p < 0.001) than the reference level. Within each attribute, the order of the levels is logical and follows the expected direction, but participant responses do not reflect significant differences between the attribute levels, with the exception of remission where some levels are statistically different but marginal utility decreases (Table 5).
Mixed logit model estimates of participant utility coefficients for each treatment attribute level (n = 201). Higher values indicate higher utility (higher preference) for a particular attribute level relative to other levels of that attribute.

Denotes reference level.
All coefficients have standard deviations which are available upon request.
p Value < 0.001.
AIC, Akaike information criterion; BIC, Bayesian information criterion; CI, confidence interval; SE, standard error.
By including an opt-out option after the forced choice task, we were able to measure the frequency of participants opting-out of treatments. On average, participants opted-out (selected ‘No, I would not actually choose this treatment’) 21% of the time (range: 8–30%) over the 12 experimental choice tasks. This reflects that treatment alternatives were sufficiently attractive that participants would more frequently choose one of them rather than none of the alternatives.
Within our DCE, we included nonexperimental choice tasks to test internal validity. For the stability test, 88% (n = 177) had the same response in the repeated choice task. For the within-set dominated pairs test, we expect most participants to choose the alternative that was unambiguously ‘better’. For this task, 94% (n = 189) of participants selected the ‘better’ treatment option. These results indicate that participants were attentively answering the choice tasks and that responses are reasonable.
Latent class results
Through our latent class analysis, we found four classes of participants with unique patterns of preferences. The covariate disease duration (year of diagnosis minus year of birth) was the only characteristic that had a statistically significant influence on class membership. With regard to probability of class membership, 27.4% of participants (n = 55) had the highest probability of being in Class 1 (focused on treatment effectiveness and benefit), 26.4% (n = 53) in Class 2, 12.9% (n = 26) in Class 3, and 33.3% (n = 67) in Class 4. Classes 2, 3, and 4 were averse to unknown risks of treatment but had different preference ordering with regard to chance of remission, known side effects, and what treatment involves (Figure 2 and Table 6).

Latent class model estimates of participant utility coefficients for each treatment attribute level (positive values indicate higher utility for a change in attribute level from the reference level; negative values indicate disutility for a change in attribute level from the reference level).
Summary of four classes of participant preferences and associated characteristics identified with latent class analysis.

Short Inflammatory Bowel Disease Questionnaire (SIBDQ) is scored from 10 (poor quality of life) to 70 (optimum quality of life).
The most important attribute for Class 1 was chance of remission. This class was the youngest and had the shortest disease duration and the lowest mean SIBDQ score for quality of life. This class had the most participants with severe UC (5.5%) at the time of the survey. Nearly 60% of participants in this class indicated they would be willing to undergo FMT as a treatment for their UC. Almost half of this class (45.5%) indicated that the ‘ick factor’ associated with using a treatment involving fecal matter was moderately unimportant to very unimportant. Class 2 preferences focused on severity of rare unknown side effects and chance of remission. Although this class had high utility for severity of rare unknown side effects, they also had high utility for chance of remission. This class had the highest mean SIBDQ score and the highest proportion of participants in remission (77.4%) at the time of the survey. Class 3 preferences focused on the severity of rare unknown side effects and the severity and chance of known side effects. This class had the highest proportion of participants who indicated they would not be willing to undergo FMT as a UC treatment and 61.5% were in remission at the time of the survey. Lastly, Class 4 focused on the severity of rare unknown side effects and what treatment would involve. This class was the oldest, had the longest disease duration, and was mostly in remission (74.6%) or had mild UC (22.4%). Almost 70% of this class indicated that their present health depends on their medications and almost half indicated that they were unsure about undergoing FMT as a treatment for their UC. More than half of this class (52.2%) indicated that the ‘ick factor’ associated with using a treatment involving fecal matter was moderately important to very important.
Probability of treatment uptake
We explored three scenarios estimating probability of treatment uptake for three hypothetical treatments. As described in the methods section, we used an unlabeled DCE design and did not specifically ask participants to choose between FMT and other specific treatments in the DCE. The hypothetical treatments in the scenarios were designed to represent possible UC treatments with different combinations of features. One treatment was comprised of attribute levels that represent biologics (Treatment A), and the other two treatments were comprised of attribute levels that represent FMT (Treatments B and C). For all treatments, the levels were held constant except for what treatment would involve (Table 2).
We found that in a scenario where the treatment options are an intravenous infusion compared to a rectal enema (scenario 1), most individuals would choose the treatment with intravenous infusion. However, in a scenario where the treatment options are intravenous infusion compared to an oral capsule or pill (scenario 2), just over half of individuals would choose the treatment with an oral capsule or pill. In a scenario where all three treatment options are compared (scenario 3), a treatment with an oral capsule or pill would be most likely to be chosen, followed by a treatment with intravenous infusion. The rectal enema would not have a high probability of being chosen.
Lastly, we explored the trade-offs between alternative modes of administration (what treatment would involve) and the chance of remission. Based on the coefficients of the attribute levels in our DCE, we found that participants were willing to accept a treatment that involves a rectal enema (least preferred mode) rather than oral capsule or pill (most preferred mode) for an approximately 30 percentage point increase in the chance of remission.
Discussion
More recently, FMT has shown promise as a potential treatment for active UC. Understanding patient preferences can identify treatment features most important to patients, support shared decision-making, and patient-centered care, which is important when exploring uptake of novel treatments like FMT. We quantitatively estimated treatment preferences of adults with active UC, specifically treatments with features that reflect FMT and biologics, and identified patient characteristics associated with different patterns of preferences. We found that almost half of participants would be willing to undergo FMT, and in the context of our DCE, the most important treatment attribute overall was chance of clinical remission. Oral capsules or pills (to represent FMT) were the preferred mode of administration compared to rectal enema or to intravenous infusion (to represent a biologic). Analysis of preference heterogeneity revealed distinct classes of participants – some who focused on treatment effectiveness and benefits, and others who were more averse to unknown risks of treatment.
To our knowledge, our findings are the first quantitative estimates of patient preferences for treatments with features that reflect FMT and biologics. Other DCE studies with different designs and research questions have explored treatment preferences of persons with UC for medications broadly or for specific medications (e.g. biologics, corticosteroids, or 5-ASAs),37–45 and most found that persons with UC prefer high treatment efficacy, high chance of remission, mucosal healing or symptom control, increasing time to next relapse or decreased risk of future flare, low risk of side effects, and bowel urgency control.37–39,41–45 Persons with active UC or recent flares have different patterns of preferences; those who had flared in the past 12 months had the highest utility for avoiding future flares compared to other treatment attributes, 44 persons with active UC had a high utility for avoiding abdominal pain, 43 and persons with active UC were more accepting of treatments with increased risks if they increased the chance of benefit. 40 Louis et al. 43 also found that disease duration was associated with different patterns of preferences; those with a longer disease duration (>5 years) had a high utility for mode of treatment administration and controlling bowel urgency compared to those with shorter disease duration (⩽5 years). Similar to this previous research, through our latent class analysis, we found that disease duration had a statistically significant impact on patient preferences and those with longer disease duration had different patterns of preferences than those with shorter disease duration.
Our results also align with previous mixed methods and qualitative research specific to FMT, which found that a high proportion of adults with UC are receptive to the idea and willing to try FMT as a treatment.14–18 These studies found that those who were hospitalized were more likely to be willing to undergo FMT, 16 and many patients reported feeling like it was a last resort treatment or that they would be willing to undergo FMT after exhausting all other treatment options. 17 Almost half of participants in our study stated they would be willing to undergo FMT as a treatment for their UC, given what they know about FMT. When asked about attitudes toward FMT, almost all participants indicated that safety, effectiveness, screening for infectious diseases, safety of delivery mode, and risk of worsening UC activity were moderately important to very important. The qualitative study by Kahn et al. 15 also found that some patients thought FMT would be easier and safer than other available treatments.
Currently, FMT is not an approved treatment for active UC and it remains unclear which patients may be most likely to respond to FMT. Recent systematic reviews and meta-analyses exploring the efficacy of FMT in UC have found that rates of short-term clinical remission (within 12 weeks of FMT) are approximately 40% in the FMT group compared to approximately 20% in the control group.5–7 Two of these studies found no significant differences in serious adverse event rates during the intervention (i.e. events or infections requiring further treatment(s), hospitalizations, surgery, malignancy, death) between the FMT group (7%) and the control group (5%).5,6 Shi et al. 7 reported that ‘the majority of adverse events were bloating, abdominal pain, cramping, blood in stool, diarrhea and fatigue’. These studies concluded that FMT appears to be beneficial in terms of clinical remission and safety for the short-term treatment of active UC. While generally considered safe, FMT has been linked to infectious transmissions, prompting safety warnings and regulation.5,9–12 Although evidence on the long-term efficacy and the safety of FMT are still not clear,5–7 certain data have demonstrated its potential long-term efficacy 8 months to beyond 2 years after treatment.46–49 The long-term effectiveness of single FMT, 46 low-intensity FMT from a single donor, 47 or daily oral FMT 48 in the treatment of active UC have been documented. In comparison, biologic therapies (tumor necrosis factor inhibitors) have demonstrated rates of short-term clinical remission between 16 and 39% in patients with UC, 50 and more recently, Singh et al. 51 have estimated rates of short-term clinical remission between 18% and 31% when used as a first-line therapy. While some biologic therapies are significantly better than others in terms of inducing clinical remission, they are associated with higher rates of adverse events. 52 Rates of adverse events vary by the type of biologic therapy and some patients may need to try more than one biologic to induce clinical remission.51,52 Understanding preference heterogeneity related to the benefits and risks of treatments can help clinicians and IBD care providers understand which patients may be most likely to choose FMT as a treatment for active UC. In our study, we found four distinct classes of participants with unique patterns of preferences. Information about which patients may be more or less likely to take treatments with specific features can facilitate better informed decisions, satisfaction and adherence by personalizing treatment approaches that are aligned with patient preferences. 20 For example, participants in the class with the highest utility for chance of remission were younger and had more severe disease. More than half of this class indicated that they would be willing to undergo FMT. In contrast, participants in Class 4 had high utility for severity of rare unknown side effects, were older, mostly in remission or mild disease, and more than half indicated they would not undergo or were unsure about undergoing FMT. Offering FMT to patients who are like those in Class 4 may not result in high satisfaction or adherence to treatment.
While our study had several strengths, it also had some limitations. We estimated the probability of treatment uptake using the relevant coefficients from the attribute levels in our DCE to reflect scenarios that represented hypothetical treatments. These estimates from our DCE may differ from direct elicitation from participants about their likelihood to take FMT or other treatments. It is possible participants may have interpreted our attribute level one-time oral capsules or pills as curative, which may have impacted their preferences. We also did not specify that the oral capsules or pills were filled with fecal matter or represented FMT. This may have influenced participant preferences as approximately 40% stated that the ‘ick factor’ associated with FMT was moderately important to very important. We limited the attributes and levels in our DCE to two common modalities of administering FMT and two common routes of dosing a biologic and this did not capture all possible protocols for FMT and/or biologics or combination therapies. The long-term effectiveness of FMT in conjunction with other therapeutic approaches, such as anti-inflammatory diets, 49 for the treatment of active UC is a noteworthy and pertinent strategy that necessitates further discussion. Our DCE choice tasks were hypothetical stated preferences, which can be different from revealed preferences (i.e. choices that patients make in real life). However, we did find that on average, 80% of the time participants did not opt out of the treatment alternatives in the DCE choice tasks (selected ‘yes, I would actually choose this treatment’). This reflects that treatment alternatives were sufficiently attractive that participants would more frequently choose one of them rather than none of the alternatives. By recruiting participants who were already enrolled in a large, national cohort study, we may have captured people who are more engaged in research and different or experimental treatment options, and it is possible that participants were not representative of the UC population. However, the average age at the time of diagnosis for participants in our study was 32 years and 58% of our participants were female, which is similar to previous reports that most Canadians with UC are diagnosed between age 20 and 30 years, and women are equally as likely to be diagnosed with ulcerative colitis as men. 36 Our response rate of 50% was also was higher or similar to the range of 44–52% reported in a meta-analysis of DCE survey studies. 53
Conclusion
Understanding patient preferences toward treatments for active UC can help identify features of treatment that are most important to patients and groups of patients who may be more likely to choose FMT. These are especially important to understand with the recent FDA approval of the first FMT product. 22 Those who are younger with more severe disease may be more likely to try FMT for active UC than those who are older with less severe disease, and oral capsules/pills are the preferred mode of administration. Patient-centered care can be enhanced by knowing which patients are more likely to be interested in FMT, potentially improving satisfaction with and adherence to treatments for active UC to maximize the effectiveness of treatment while considering heterogeneity in patient preferences.
Footnotes
Acknowledgements
We would like to acknowledge our IMAGINE Patient Research Partners (Sandra Zelinsky, Sara Blake, Kim Daley, Alysia De Nino, Anny Fernandez, Sophia Khan, Shawn Reynolds) for their contributions to our survey design and interpretation of survey results. We would also like to acknowledge the IMAGINE study participants who completed our survey and contributed to this important body of research. Lastly, we would like to acknowledge the following IMAGINE Network sites for their contributions to recruitment for our survey: University of Calgary (61 participants recruited), University of Alberta (60 participants recruited), University of Manitoba (85 participants recruited) and McMaster University (69 participants recruited).