
Abstract
Alopecia areata (AA) is a chronic inflammatory disease mainly involving Th1 immunoreaction, but Th2 is also involved. A 9-year-old girl presented to our clinic with severe alopecia for 2 months and pruritus-related rashes for 8 years. She was diagnosed with AA and atopic dermatitis (AD), and the Severity of Alopecia Tool (SALT) score was 98. She used a 0.05% halometasone cream (occlusive dressing) topically applied overnight (6 days weekly) for 10 months. After 2 months of treatment, she had regrowth of both black and white hair. However, relapse occurred and she gradually lost all black terminal hair, but white terminal hair remained, with a SALT score of 70. Continuous topical occlusion resulted in white hair regrowth with a SALT score of 20 at the end of month 10. Dupilumab was initially prescribed as a 600-mg subcutaneous injection and maintained at 300 mg every 4 weeks thereafter. Hair repigmentation (10% of whole hair density) started, with black hair shaft appearing at the proximal end in parietal-occipital and occipital areas after three injections at week 12 of dupilumab therapy, with a SALT score of 10. After seven injections at week 28, the percentage of black hair shaft reached up to 90, and she regained her black hair and the pigmented section of hair shaft continued to grow longer at the rate of normal hair growth. Nevertheless, 4 months after termination of dupilumab therapy, the black terminal hair began to fall off, and white vellus hair gradually regrew on the scalp, with a SALT score of 80. Dupilumab induces hair regrowth and repigmentation of white terminal hair without disturbing the anagen phase of hair follicles. Therefore, melanocytes in AA may be a potential target of Th2-related factors. Persistent regrowth of white hair may be used as a signal of Th2 dominance in AA management.
Introduction
Alopecia areata (AA) is a non-scarring hair loss disease and chronic inflammation caused primarily involving T lymphocytes and then Th1 cytokines, such as interferon-γ produced by activated NKG2D+CD8+ T cells around the hair follicles. 1 These Th1 cytokines induce regression of hair follicles possibly by the destruction of immune privilege and exposure of the autoantigen, as well as infiltration of a large number of inflammatory cells around hair follicles. 1 However, Th2 cytokines such as interleukin (IL)-4 and IL-13 are also involved in the pathogenesis of AA, especially in patients with alopecia totalis (AT) and alopecia universalis (AU), 2 consistent with the finding that Th2 cytokines are closely related to the severity and persistence of AA. 3 Regrowth of white hair in individuals with pigmented hair after recovery from AA is not rare, but there is a lack of firm evidence and understanding regarding the underlying pathogenesis and adequate treatment. In this study, we report a case of hair repigmentation in a 9-year-old girl with AA and atopic dermatitis (AD) who had white hair regrowth after dupilumab treatment.
Case report
A 9-year-old girl visited our hair clinic in the First Affiliated Hospital of Sun Yat-sen University and reported gradual worsening of severe hair and eyebrow loss for 2 months. She had a history of allergic rhinitis, asthma for 2 years and infantile eczema 8 years ago. She also had a family history of allergic rhinitis, which was reported in her mother and younger brother. On physical examination, she had scratches on her elbow fossa and abdomen, mild body dryness and ichthyosis on both legs. Therefore, a diagnosis of AA and AD was made based on her medical history and clinical manifestation, plus dermoscopic signs on her scalp. The Severity of Alopecia Tool (SALT) score was 98, and Eyebrow Assessment (EBA) score was 0. Thyroid-stimulating hormone, FT3, FT4, antinuclear antibody and anti-double-stranded DNA antibody were found to be in the normal range. However, serum total IgE (tIgE) was high at 999.6 IU/mL (normal range: 0–120 IU/mL). Additionally, specific IgE (sIgE) for dust mite was higher than 100 IU/mL, grade 6 (normal range: grade 0). Both percentage and absolute value of peripheral eosinophils were elevated at 0.121 (normal range: 0.005–0.05) and 1.03 × 109/L (normal range: 0.05–0.5 × 109/L), respectively.
Initially, she was treated for AA with a 0.05% halometasone cream (occlusive dressing) as a topical application overnight (6 days weekly) for 10 months. After 2 months of therapy, white vellus hair regrew and terminal hair appeared evenly on the scalp, while a small amount of black vellus hair appeared on the occipitalia. In the following months, growth of both white and black hair was observed, reaching a SALT score of 40. However, AA relapsed as early as the fourth month of topical steroid therapy without obvious triggers, resulting in the loss of all black hair and part of white terminal hair. Her SALT score was 70 by the end of the fifth month, with a sparse white hair distribution. However, the same treatment was extended for five more months, leading to the growth of more white terminal hair, with a SALT score of 20. At that time, her eyebrows showed regrowth of white and sparse hair, with an EBA score of 1. A negative result in Wood’s lamp examination eliminated the possibility of scalp vitiligo.
Because of the unsatisfactory treatment response of AA and concomitant AD, dupilumab was initiated, initially administered at a dose of 600 mg as a subcutaneous injection and then maintained at a dose of 300 mg every 4 weeks thereafter. Informed consent signed by the patient’s parents was obtained before the injection. Four weeks after the first injection, a small amount of black hair appeared on the eyebrows. After three injections at week 12 of dupilumab administration, a short segment of black terminal hair shaft appeared at the proximal end in the parietal-occipital and occipital areas, with a density of 10% amongst white hair areas, together with hair regrowth, and her SALT score decreased to 10. Black and white eyebrows co-existed with an EBA score of 2. After seven injections at week 28, the percentage of pigmented hair shaft reached up to 90 and hair density fully restored to the normal range. Her eyebrows totally recovered with an EBA score of 3. At the same time, the repigmented segment of the hair shaft continued growing longer (Figure 1).

Clinical images showing the occipital view of hair regrowth and colour before and after dupilumab treatment. (a) Before dupilumab treatment. (b) After one injection at week 4 of dupilumab treatment. (c) After three injections at week 12 of dupilumab treatment. (d) After seven injections at week 28 of dupilumab treatment.
To understand the rate of repigmentation and elongation of the pigmented hair shaft, five patches of area 1 × 1.5 cm2 were observed by dermoscopy in seven selected locations after administering six injections at week 24. Seven locations on the scalp were chosen, that is, in the frontal, parietal, parietal-occipital, temporal (left and right) and occipital (upper and lower) areas (Figure 2). The length of the repigmented hair shaft was measured and recorded at multiple time points at all locations except in the lower occipitalia, wherein the shaft had been trimmed regularly before the clinical visits, starting from week 24 of dupilumab administration. The proportions of pigmented hair in the seven locations on the scalp were 89.9%, 91.5%, 94.4%, 97.5%, 93.8%, 94.3% and 25.3%, respectively, at week 24, wherein the lowest pigmented hair was observed in the lower occipital area. During treatment, the proportion of white hair continuously decreased and that of repigmented black hair increased (Figure 3), showing a significant negative correlation between them (r = −1, p = 0.0004). The length of the repigmented hair shaft was measured and recorded from six locations except in the lower occipitalia area on days 164 (week 24), 204 (week 30), 241 (week 35), and 281 (week 41) after the first injection of dupilumab (Figure 4). The average length of the overall elongation of black hair in the whole head in a certain time length was derived by adding the increased length of growing black hair in the six locations and dividing by 6. After calculation, that is, growth length (mm) divided by the time length (day), the growth rate of the repigmented hair shaft from days 164 (week 24) to 204 (week 30), from days 204 (week 30) to 241 (week 35) and from days 241 (week 35) to 281 (week 41) after the first injection of dupilumab were 0.32 mm/day, 0.41 mm/day and 0.4 mm/day, respectively, all values being closer to the normal hair growth rate of 0.411 mm ± 0.053 mm/day. 4
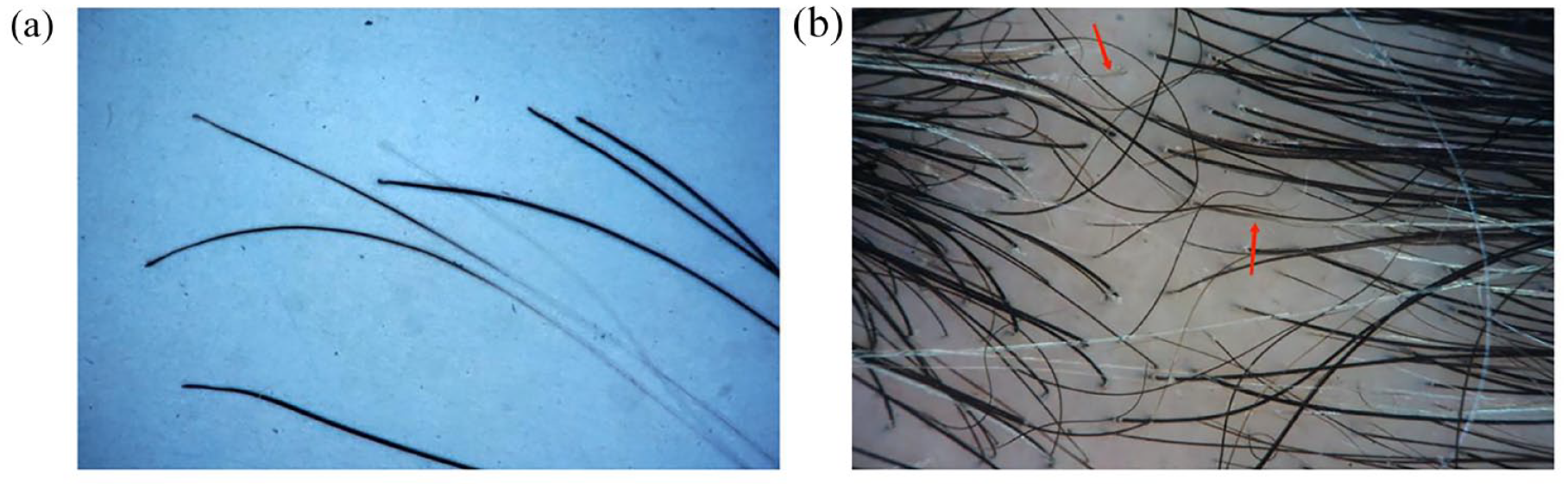
Gross and dermoscopic view of hair repigmentation after six injections at week 24 of dupilumab treatment. (a) Photograph of the shed hair with repigmentation at the distal end. (b) Dermoscopic view of hair repigmentation (red arrow) on the scalp.

Percentage of black and white hairs across the scalp during dupilumab treatment. During dupilumab therapy, the proportion of white hair continuously decreased and that of repigmented black hair increased, showing a significant negative correlation between them (r = −1, p = 0.0004).
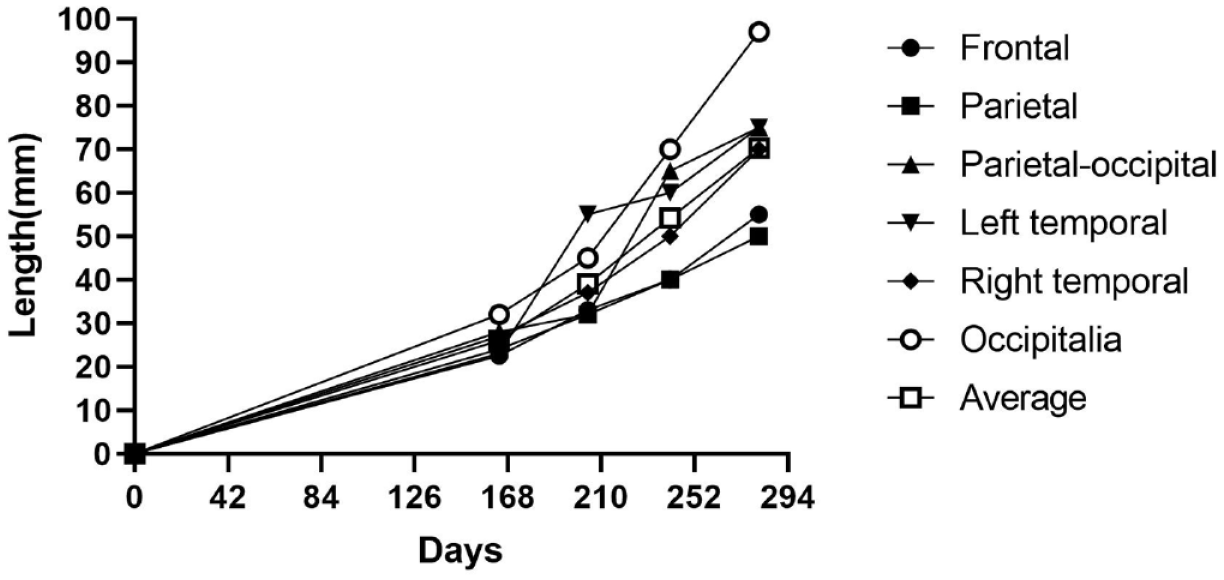
Increasing length of the pigmented hair shaft segment at different locations on the scalp after dupilumab administration. The average repigmentation rates on the whole scalp were 0.32 mm/day, 0.41 mm/day and 0.4 mm/day, respectively, from days 164 (week 24) to 204 (week 30), from days 204 (week 30) to 241 (week 35) and from days 241 (week 35) to 281 (week 41) after the first injection of dupilumab, which were all similar to the normal hair growth rate of 0.411 mm ± 0.053 mm/day.
After 28 weeks of treatment with dupilumab, titres of serum tIgE and sIgE to dust mite decreased to 429.8 IU/mL and 62.9 IU/mL (grade 5), respectively. Both percentage and absolute value of eosinophils also decreased, which were at 0.073 and 0.42×109/L, respectively. All the above indexes showed a normal range except for the eosinophil percentage. The tIgE and sIgE were still much higher than the normal range.
However, the patient discontinued dupilumab for financial reasons after 7 months of treatment but was maintained on topical 0.05% halometasone cream as a topical occlusion. Four months later, she started to lose the black terminal hair completely and had only sparse white short hair and vellus hair, with a SALT score of 80, and she was lost to follow-up.
Discussion
Dupilumab is a fully humanized monoclonal antibody that targets the alpha subunit of the IL-4 receptor, which inhibits the downstream signalling of IL-4 and IL-13. 5 Accumulating evidence suggests that dupilumab induces hair regrowth in patients with AA.6–8 Yet, a few other studies have demonstrated the onset of AA in patients treated with dupilumab for other diseases. 9 Thus, IL-4 and/or IL-13 may play an essential role in the pathogenesis of at least part of patients with AA. In our AA case, we found that dupilumab not only induced hair regrowth but also restored the colour of white terminal hair. To the best of our knowledge, no previous studies have linked hair depigmentation with Th2 immunity in AA before dupilumab treatment for AA management.
Numerous factors are involved in melanogenesis, but the specific process of hair repigmentation in the recovery phase of AA is not fully revealed. 10 The term ‘poliosis’ in AA was used by Sleiman Rima in describing the regrowth of white hair in patients with AA. 11 Migratory poliosis may represent a forme fruste of AA. 12 The clinical mosaic changes in hair colour in patients with AA reflect the activity of the alopecia condition. 13 A previous study showed that hypertension was significantly associated with poliosis in AA, but the specific underlying mechanism remains unclear. 14 Although at this stage, the correlation of melanogenesis with the AA pathogenesis, especially regarding T cell-mediated (auto)immunity, is largely unclear, studies from other researchers may shed light on this topic. One report suggested that hair follicle melanocytes may be the immune trigger point in AA for the following reasons: (1) Melanocyte metabolites could be antigenic and serve as the primary cause of autoimmune attacks. (2) Melanogenesis-related peptides have long been thought to be autoantigens in the CD8+ T cell-dependent autoimmune mechanism of AA. (3) The self-deficiency of hair follicle melanocytes may induce immune attacks and lead to AA. 15 As antigens are exposed and presented by antigen presenting cells, they migrate to peripheral lymph nodes and activate CD8+ cytotoxic T lymphocytes and CD4+ T cells. Subsequently, cytokines activate B lymphocytes with antibody synthesis. Attacks on melanocytes may lead to the breakdown of the immune privileges of the hair follicles. Afterwards, the autoimmune response is amplified, leading to the destruction of hair follicles. The hair follicles enter the telogen phase to avoid irreversible damage. 15 Bertolini et al. presented direct evidence depicting T cells attacking melanocytes in hair follicles. 16 In our case, both black and white vellus hair regrew after the first 3 months of topical halometasone cream therapy, but all black hairs were lost and the white terminal hair remained alongside the subsequent 7 months of 0.05% topical halometasone cream therapy. This phenomenon also provides evidence that melanocytes can be a possible target in AA pathogenesis.
During dupilumab treatment, the proportions of white hair and repigmented black hair were recorded many times. In this study, we precisely recorded that the percentage of repigmented hair shaft reached up to 90, and her hair fully recovered after seven injections at week 28. This is mainly attributed to the repigmentation of white hair into black hair and the regeneration of black vellus hair. Among the seven locations on the scalp, the proportion of hair repigmentation in the posterior occipitalia was the lowest, suggesting the uneven distribution of inflammation and recovery of repigmentation in different scalp parts. The growth rates of the repigmented hair shaft in different locations and time points were all similar to the normal hair growth rate of 0.411 mm ± 0.053 mm/day. 4 This result suggests that the recovery of melanocytes may occur without interference with the hair follicular cycle and the growth of the hair shaft. In a previous study, we described the sequential cyclic changes in hair roots of shed hair in the course of diffuse AA, with anagen in the early phase and telogen in the later phase. 17 The hair cycling is disturbed by disease progression of AA, but not in the recovery phase that repigmentation can occur de novo without disturbance in hair cycling.
One may wonder why dupilumab can facilitate pigmentation in this patient with AA and poliosis. This is because melanocytes strongly express IL-4Rα, confirmed by dual staining with a melanocyte-specific marker. 18 Melanogenesis of normal human melanocytes can be inhibited by IL-4 and IL-13 through the JAK2–STAT6 signalling pathway.19,20 In our case, white hair persisted even with topical steroid administration, which suggests that hair repigmentation in part of patients with AA is beyond the inflammation inhibition scope of steroids. Therefore, we speculate that repigmentation of white hair in patients with AA can be achieved by dupilumab binding to the alpha subunit of IL-4R, thus preventing interference with melanogenesis by IL-4 and IL-13. Therefore, we infer that IL-4 and IL-13 may be the key factors that interfere with hair pigmentation in the girl in the present case. This suggests that persistent regrowth of white hair may be a biomarker indicating the immune mechanism of AA biased towards Th2 immunity. However, whether the same depigmentation process occurs in all patients with AA who have regrowth of white hair remains unclear, as systemic steroids usually resolve the problem in most patients with AA. Further research work is needed to unravel the underlying mechanism.
Conclusion
This case study presents an AA case wherein dupilumab treatment-induced hair regrowth, together with repigmentation of regrown white terminal hair de novo without disturbing the anagen phase of hair follicles. Our findings suggest that IL-4 and/or IL-13 may be involved in the damage process of hair follicle melanocytes in AA. Therefore, hair follicle melanocytes in AA may be a potential target of type II immune-related factors. The persistent regrowth of white hair in AA may be a clinical biomarker of type II immune dominance and thus help clinicians in making optimum choices in AA management.
Supplemental Material
sj-docx-1-taj-10.1177_20406223231191049 – Supplemental material for Hair repigmentation and regrowth in a dupilumab-treated paediatric patient with alopecia areata and atopic dermatitis: a case report
Supplemental material, sj-docx-1-taj-10.1177_20406223231191049 for Hair repigmentation and regrowth in a dupilumab-treated paediatric patient with alopecia areata and atopic dermatitis: a case report by Xin Yan, Munire Tayier, Sin Tong Cheang, Zhongmin Liao, Yi Dong, Yifeng Yang, Yanting Ye and Xingqi Zhang in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.