
Abstract
Background:
Which noninvasive brain stimulation (NIBS) treatment – transcranial direct current stimulation (tDCS) or transcranial magnetic stimulation (TMS) – is more beneficial for stroke patients’ cognitive rehabilitation is still up for debate.
Objectives:
Our goal is to provide an overview of the research on the effectiveness and safety of various NIBS protocols.
Design:
Systematic review and network meta-analysis (NMA) of randomized controlled trials (RCTs).
Methods:
This NMA compared any active NIBS versus sham stimulation in adult stroke survivors to enhance cognitive function, with a focus on global cognitive function (GCF), attention, memory, and executive function (EF) using the databases MEDLINE, Embase, Cochrane Library, Web of Science, and ClinicalTrials.gov. The NMA statistical approach was built on a frequency framework. The effect size was estimated by the standardized mean difference (SMD) and a 95% confidence interval (CI). We compiled a relative ranking of the competing interventions based on their surface under the cumulative ranking curve (SUCRA).
Results:
NMA showed that high-frequency repeated TMS (HF-rTMS) improved GCF compared with sham stimulation (SMD = 1.95; 95% CI: 0.47–3.43), while dual-tDCS improved memory performance versus sham stimulation significantly (SMD = 6.38; 95% CI: 3.51–9.25). However, various NIBS stimulation protocols revealed no significant impact on enhancing attention, executive function, or activities of daily living. There was no significant difference between the active stimulation protocols for TMS and tDCS and sham stimulation in terms of safety. Subgroup analysis demonstrated an effect favoring activation site of the left dorsolateral prefrontal cortex (DLPFC) (SUCRA = 89.1) for enhancing GCF and bilateral DLPFC (SUCRA = 99.9) stimulation for enhancing memory performance.
Conclusion:
The HF-rTMS over the left DLPFC appears to be the most promising NIBS therapeutic option for improving global cognitive performance after stroke, according to a comparison of numerous NIBS protocols. Furthermore, for patients with post-stroke memory impairment, dual-tDCS over bilateral DLPFC may be more advantageous than other NIBS protocols. Both tDCS and TMS are reasonably safe.
Registration:
PROSPERO ID: CRD42022304865
Keywords
Introduction
Over two-thirds of stroke survivors experience cognitive impairment or decline after their stroke,1,2 which makes it challenging for them to carry out their daily activities, 3 and which may be an indication of a poor prognosis with worse rehabilitation outcomes, 4 the onset of dementia, 5 and higher mortality. 6 Rehabilitation of stroke survivors has been a prominent research focus for academics and medical professionals as the occurrence of stroke has risen over the past 20 years.
As a system, attention, memory, executive function (EF), visuospatial ability, and language all act as part of cognition, which is not a single concept. 7 Many cognitive domains are affected by cognitive impairment following a stroke, although attention, 8 memory, 9 and EF 10 are some of the more prevalent ones. And these multidimensional cognitive deficits are likely to persist into the subacute or even chronic phase after stroke onset; 11%–31% of patients still have memory impairment 1 year after stroke,11,12 and 66% of stroke victims continue to experience EF decompensation in varied degrees. 13 On the other hand, roughly 30% of stroke survivors who experience attentional abnormalities end up developing dementia. 8 These cognitive problems also result in significant functional limitations, such as hampered rehabilitation efforts, a diminished ability to return to work, and a need for additional support. 14
Unfortunately, there are still very few cognitive therapies available for stroke patients, and the evidence is still insufficient. The effectiveness of several non-pharmacological rehabilitation techniques, such as cognitive training, 15 brain stimulation, 16 virtual reality training, 17 psychological interventions, 18 and many more, are still debatable but are thought to improve cognitive function in stroke survivors by promoting neuroplasticity.
Noninvasive brain stimulation (NIBS) technology, such as repeated transcranial magnetic stimulation (rTMS), theta-burst stimulation (TBS), and transcranial direct current stimulation (tDCS), which can induce change in excitability of the underlying brain cortex in a noninvasive fashion and potentially induce long-lasting neuroplastic changes by either magnetic or electric fields, has gradually become more prevalent in stroke rehabilitation in recent years.19–22 Briefly, TMS acts differently by generating a time-varying magnetic field perpendicular to the stimulation coil, which then induces a current in the superficial cerebral cortex nearly parallel to the coil, by affecting the excitability of neurons. Different stimulation frequencies have different effects on cortical activity, with high-frequency (> 1 Hz) stimulation (HF-rTMS) promoting local neuronal excitability, while low-frequency (⩽ 1 Hz) stimulation (LF-rTMS) shows inhibitory effects. 23 The TBS is a novel rTMS consisting of three pulse bursts at 50 Hz. It is divided into two forms, continuous TBS (cTBS) and intermittent TBS (iTBS), which play inhibitory and facilitatory roles in local cortical excitability, respectively. 24 On the other hand, tDCS is a weak, constant, low-intensity direct current (current intensity of 0.5–2 mA) applied to the cerebral cortex through two electrodes, anode and/or cathode, placed on the scalp, which, through subthreshold stimulation, changes the difference between the internal and external potential of the neuronal membrane of the brain and regulates the threshold of the action potential, thus affecting the excitability of neurons in the stimulated area. 5 According to the selection and placement of electrodes, they can be divided into anodal tDCS (a-tDCS), cathodal tDCS (c-tDCS), and dual tDCS (both anodal and cathodal tDCS).
In the present review, we will concentrate primarily on the aspect of cognition impairment from the perspective of the therapeutic efficacy of NIBS with various post-stroke dysfunctions. Some findings have been drawn from meta-analyses about the cognitive function of language25–28 and unilateral neglect,27–30 despite the lack of and conflicting evidence on attention, memory, and EF. The current meta-analysis for NIBS showed that most studies concluded that TMS had significant effects on attention, memory, working memory, global cognition,23,31 and activities of daily living 32 (ADL) in post-stroke patients, while the effect of different frequencies of treatment options did not differ significantly, 33 and HF-rTMS had significant improvements in global cognition on left dorsolateral prefrontal cortex (DLPFC). 32 The findings of tDCS research are disputed, with some advocating the treatment regardless of disease type for cognitive recovery in neurological disorders. 23 Some suggest an acute facilitative effect on repairing attentional impairment, but no improvement in general cognition or working memory. 27 Another report claims that tDCS improves attention and general cognition after stroke, but not memory. 34 But the effect of NIBS stimulation treatment on EF after stroke is limited.
Rationale
There is so far conflicting evidence from systematic reviews of randomized controlled trials (RCTs) on the effectiveness of different NIBS approaches for improving different domains of cognitive function after stroke. New RCTs on TMS and tDCS13,24,35,36,37 were not included in the prior meta-analysis. To acquire integrated results, it is required to expand these investigations. Besides, it is common that one study involves only electrical or magnetic stimulation, which has different costs and operational conveniences. And the same study frequently uses only one or two treatment protocols that may differ in terms of stimulation target, frequency or electrode selection, timing, intensity, and so on, while thus, combining TMS and tDCS therapies in one trial is often unnecessary. The lack of head-to-head comparative trials makes it difficult to compare the effectiveness of different NIBS protocols using conventional meta-analysis.
Network meta-analysis (NMA) combines head-to-head and indirect evidence from randomized trials.38–40 By utilizing the strength of indirect evidence, NMA guarantees all treatment comparisons, allowing the assessment and rating of comparative effects not expressly evaluated in randomized clinical trials.41,42
Objective
We aim to summarize the evidence network of RCTs of various NIBS protocols, including rTMS (HF-rTMS, LF-rTMS), TBS (iTBS, cTBS), and tDCS (a-tDCS, c-tDCS, dual-tDCS), and stimulation site, on cognitive rehabilitation, particularly for attention, memory, and EF in patients after stroke, as well as ADL and safety, to provide recommendations for clinical treatment decisions.
Methods
Protocol and registration
We prepared this protocol following the recommendations of Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guidance 43 (Supplemental File 1), which has been registered in the PROSPERO database under the ID CRD42022304865.
Eligibility criteria
Participant
Studies on adults (over 18 years old) meeting the diagnostic criteria for stroke through head computed tomography or magnetic resonance imaging with cognitive impairment after a stroke were considered. Cognitive impairment includes attention, memory, and EF, tested by mini-mental status examination (MMSE), Montreal cognitive assessment (MoCA), or other domain-specific cognitive tests. There was no limitation on stroke type and stage. Studies with no more than five individuals were excluded.
Interventions and comparators
We chose groups comparing NIBS, including HF-rTMS, LF-rTMS, iTBS, cTBS, a-tDCS, c-tDCS, or dual-tDCS, with the control group eligible for inclusion. In the control group, sham stimulation with or without conventional/computerized cognitive treatment was acceptable. We excluded studies by no more than five sessions of NIBS for meta-analysis.
Outcomes
We set the primary outcome as cognitive function evaluated before and after neurostimulation therapy in the short term. Primary outcome indicators focused on scale scores assessing global cognitive function (GCF), attention, memory, and EF.
The ability to perform ADL was one of the secondary outcomes, measured by scale scores assessing ADL. Another secondary outcome was safety, measured by the number of dropouts and adverse events.
Studies
We included all genuine parallel or cross-over trials RCTs for review. Articles reporting protocols, in-progress trials, retrospective studies, or case reports were excluded. Studies reporting sufficient information to compute effect size statistics (i.e. mean and standard deviations or standard errors, or median and ranges or interquartile ranges, exact F-, p-, t-, or z-values], published in an international peer-reviewed journal until February 10, 2022, in only English language were considered.
Information sources
We searched the following databases for relevant English language literature: PubMed (MEDLINE), Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), and Web of Science from their inception to February 2022. For the ongoing trials register, we also searched the US National Institutes of Health Ongoing Trials Register ClinicalTrials.gov (www.ClinicalTrials.gov/). We will also explore the reference lists of included trials, systematic reviews, and meta-analyses identified during the screening process to identify other eligible trials. Gray literature, such as conference proceedings, will also be searched.
Search
Supplemental File 2 contains the MEDLINE search technique. Other databases also can use this search approach.
Study selection
One reviewer (WL) screened titles and abstracts for irrelevant research. Two writers (YW and JR) examined all remaining full-text studies. Disagreements were discussed with the third author (JC) and resolved through consensus. Figure 1(a) depicts the flowchart structure.

(a) Flow chart of literature screening. (b) Risk of bias graph.
Data collection process
YW and JR extracted trial and summary result data independently. If data were unavailable, we emailed the corresponding author to request the information; if the author did not reply, we contacted him again after 2 weeks and asked twice more.
Data items
We independently evaluated the following items utilizing checklists: (1) methods of random sequence generation, (2) methods of allocation concealment, (3) blinding of outcome assessors, participants and personnel, (4) use of an intention-to-treat analysis, (5) adverse effects and dropouts, (6) participants (number, sex, age, stroke type, days after stroke onset to study entry, intervention, protocol of stimulation, site of stimulation, etc.), (7) comparison (details of protocol in control groups, and (8) outcome data [MMSE, MoCA for GCF, Stroop test (ST), trail making test (TMT), digital span (DS), visual/auditory continuous performance test (VCPT/ACPT) for attention function, visual/verbal learning test-delayed recall (ViLT/VeLT) and Rivermead behavior memory test (RBMT) for memory function, digital symbol test (DST) and tower of London (TOL) for EF, and functional independence measure (FIM) or Barthel index (BI) for ADL].
We gathered data from ‘Results’ sections and tables or estimated them from figures and appendices using GetData Graph Digitizer 2.26 software (http://www.getdata-graph-digitizer.com/download.php). Mean and standard deviation (SD) changes revealed each neurostimulation therapy’s effectiveness. The mean change was calculated as the arithmetic difference between baseline and poststimulation values. When SD was unavailable for absolute baseline and poststimulation values, we used the correlation method. 44 We estimated the variance following what Hozo et al. 45 reported if the data were displayed by median and range. We contacted the corresponding author of the original text if the outcome of the study detail were unclear.
Geometry of the network
The network’s geometry defines direct comparisons’ relationship and precision. We compared rTMS (HF-rTMS, LF-TMS), TBS (iTBS, cTBS), and tDCS (a-tDCS, c-tDCS, dual-tDCS) with sham stimulation. The nodes were linked by a line when the treatments were directly comparable. The width of each line is proportional to the number of RCTs, and the size of each node is proportional to the number of patients (sample size). The colors of the edges indicate the risk of bias for this comparison (green = low, yellow = unclear, and red = high risk of bias).
Risk of bias within individual studies
The Cochrane Handbook 5.1.0 risk of bias table was used to evaluate the quality of each study, which included seven domains of bias: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. 46 The Cochrane Handbook 5.1.0 classifies each evaluation scenario as high, medium, or low risk. Figure 1(b) shows the study outcomes.
Summary measures
We calculated the standardized mean difference (SMD) and 95% confidence interval (CI) for studies that examined the same underlying construct employing various outcome measures. Odds ratio (OR) and 95% CIs were used to estimate dropouts and adverse events. We generated contrast-based forest plots for comparison. I2 more than 50% was considered significant heterogeneity. 46
We compiled a relative ranking of the competing interventions based on their surface under the cumulative ranking line (SUCRA). 47 Higher SUCRA means greater treatment results. RevMan 5.4.1 performed the conventional meta-analysis. We draw network evidence relationship diagrams, NMA forest diagrams, funnel diagrams, Egger test, sensitivity test, and the corresponding statistics 48 by STATA 14.2 (Stata Corporation, Lakeway, Texas, USA).
Planned method of analysis
The statistical method of an NMA is based on a frequency framework. All the outcome indicators use the random-effects model, 48 which follows the graph-theoretical methodology and permits multi-arm trials. 49
Assessment of inconsistency
There is no general inconsistency if p > 0.05 when testing global consistency. Local inconsistencies between direct and indirect evidence were checked via node splitting. 50 We evaluated local inconsistencies by calculating each network closed loop’s inconsistency factors (IFs) and 95% CIs. Direct and indirect evidence were consistent if the 95% CI’s bottom limit was 0 or near 0.
Risk of bias across studies
Publication bias was assessed with a funnel plot and Egger’s test. 51 We conducted a sensitivity analysis to exclude low-quality studies.
Quality of evidence
The overall quality of the results in this paper was assessed using a method that extends the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) system 52 to NMAs. We used directly comparable quality ratings to establish evidence certainty (confidence in the evidence/quality of the evidence). 53 Limitations in study design, inconsistency, indirectness, imprecision, and publication bias were scored. 52 Evidence can be high, moderate, low, or very low). 54 Evidence profiles were obtained using the GRADEpro GDT (https://gdt.gradepro.org/app/). 55
Additional analyses
We also included the stimulation site in our pre-specified subgroup analysis as a potential effect-influencing factor.
Results
Study selection
We identified 792 studies from electronic databases, and 522 articles were screened by title and abstract after removing duplicates. A total of 63 full-text articles were potentially eligible for inclusion in the review. We excluded 36 studies for the following reasons: irrelevant study design (case report, self-controlled study, and not placebo stimulation of intervention), the same sample, irrelevant patients or outcomes, and not NIBS for intervention over the brain – the remaining 27 studies with 1,041 participants in a qualitative analysis RCTs. Three studies56–58 with no more than five sessions of stimulation were removed. We also excluded three trials for data unextractable59–61 and one 62 without details about tDCS protocol, to which we contacted the corresponding authors without reply. The quantitative meta-analysis included 20 trials13,24,35–37,63–77 with 840 participants (see Figure 1(a), Table 1).
Characteristics of the included studies.

AMT, active motor threshold; a-tDCS, anode-transcranial direct current stimulation; BI, bilateral; C, control group; CSA, contralateral supraorbital area; cTBS, continuous theta burst stimulation; c-tDCS, cathode-transcranial direct current stimulation; DLPFC, dorsolateral prefrontal cortex; FT, fronto-temporal; HC, healthy control; I, intervention; IFG, inferior frontal gyrus; Ip, ipsilesional; IQR, interquartile range; ISA, ipsilesional supraorbital area; iTBS, intermittent theta burst stimulation; M1, primary motor cortex; MT, motor threshold; NI, non-ipsilesional; RT, rehabilitation therapy; rTMS, repetitive transcranial magnetic stimulation; SD, standard deviation; STG, superior temporal gyrus; tDCS, transcranial direct current stimulation; TMS, transcranial magnetic stimulation; TS, total session of stimulation.
① Global cognitive function, ② attention, ③ memory, ④ executive function, ⑤ activities of daily living.
Study characteristics
Nineteen of 20 studies (95%) were RCTs, while one (5%) was a randomized cross-over. 67 Two tDCS,64,65 and three TMS24,70,76 had three arms, and one tDCS study 68 had four arms. The sample sizes of the included studies ranged from 14 to 100. Participants’ ages ranged from 42.5 to 70.3 years. Since stroke onset, the average time was 19.13 days to 3.97 years. Eighty-five patients treated with active anode-tDCS in four studies,64–66,68 90 patients with dual-tDCS in four studies,13,35,63,67 40 patients with cathode-tDCS in two studies,36,68 90 patients with HF-rTMS in six studies,69–72,74,76 118 patients with LF-rTMS in six studies,24,37,73,75–77 15 patients with iTBS in one study, 70 30 patients with cTBS, and 30 patients with LF-rTMS plus cTBS all in one study. 24 The median number of stimulation sessions was 15. Table 1 summarizes the trials’ features.
Network meta-analysis
Figure 2 shows the network structure for GCF and memory evaluation. Supplemental Figure 1 shows the network structure for the rest of the main and secondary outcomes. League tables (Table 2 and Supplemental Table 1) exhibit the results of the NMA.

Network diagrams of NIBS versus Sham stimulation in patients with stroke for global cognitive function (a) and memory (b).
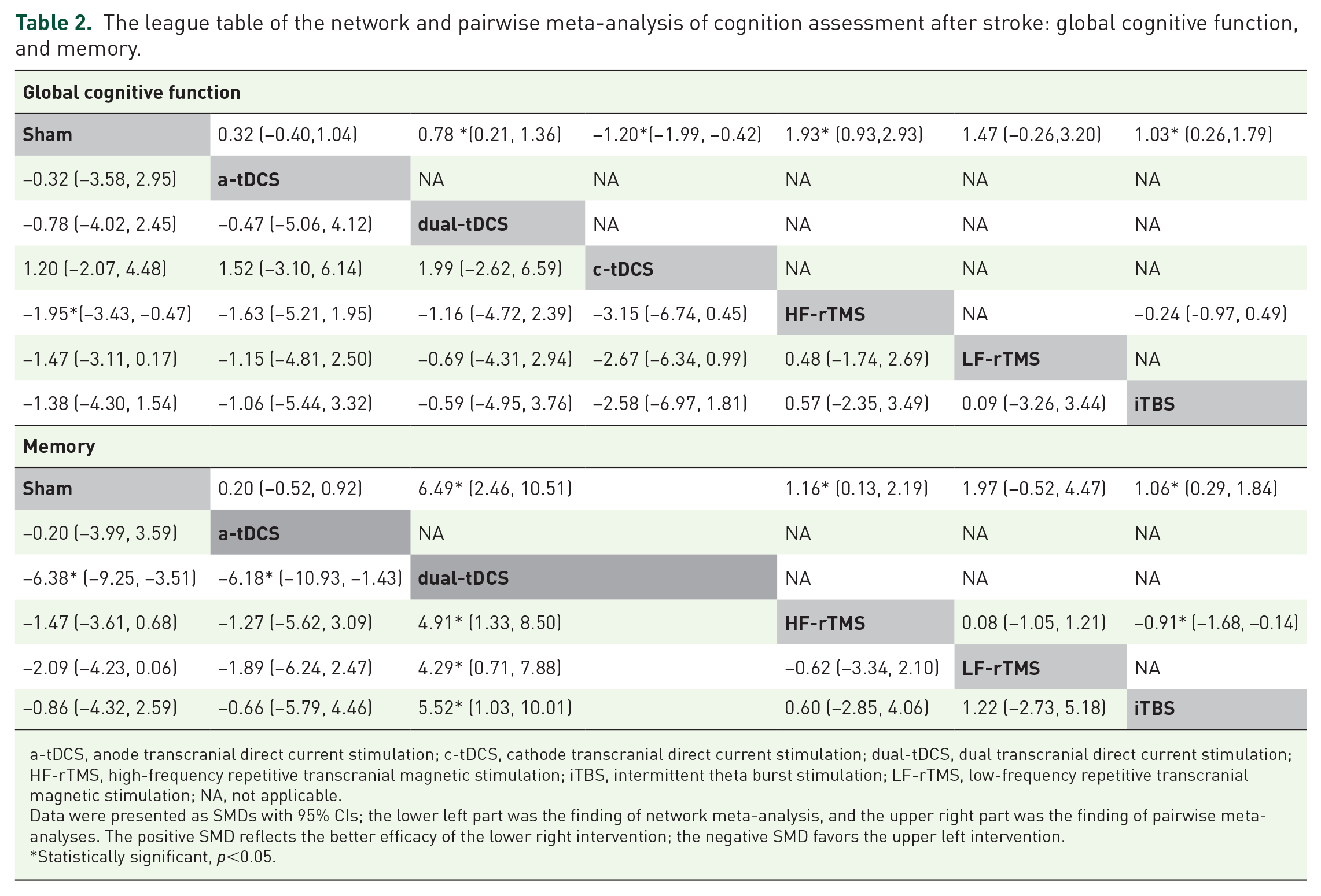
The league table of the network and pairwise meta-analysis of cognition assessment after stroke: global cognitive function, and memory.
a-tDCS, anode transcranial direct current stimulation; c-tDCS, cathode transcranial direct current stimulation; dual-tDCS, dual transcranial direct current stimulation; HF-rTMS, high-frequency repetitive transcranial magnetic stimulation; iTBS, intermittent theta burst stimulation; LF-rTMS, low-frequency repetitive transcranial magnetic stimulation; NA, not applicable.
Data were presented as SMDs with 95% CIs; the lower left part was the finding of network meta-analysis, and the upper right part was the finding of pairwise meta-analyses. The positive SMD reflects the better efficacy of the lower right intervention; the negative SMD favors the upper left intervention.
Statistically significant, p<0.05.
Summary of network geometry and Synthesis of results
Global cognitive function
Twelve studies13,24,36,64,69–75,77 (460 participants) involving seven treatment options were employed to evaluate GCF. Pairwise meta-analysis between NIBS options and sham stimulation revealed that dual-tDCS, HF-rTMS, and iTBS were significantly more effective than sham stimulation (SMD = 0.78; 95% CI: 0.21–1.36, N (number of studies) = 1, total sample size = 50, p = 0.008; SMD = 1.93; 95% CI: 0.93–2.93, N = 5, total sample size = 171, p = 0.0002, I2 = 85%; SMD = 1.03; 95% CI: 0.26–1.79, N = 1, total sample size = 30, p = 0.009, respectively. See Table 2 and Supplemental Figure 2A). Based on NMA, only HF-rTMS significantly enhanced the impact in comparison with sham stimulation (SMD = 1.95; 95% CI: 0.47–3.43, p < 0.05). None of the other treatment comparisons revealed a statistically significant difference (Table 2 and Supplemental Figure 3A).
Attention
Fourteen studies13,24,35,63–68,70–72,76,77 (558 patients) involving seven treatment options reported scales representing attention function were compared directly and indirectly. Direct evidence indicated that all tDCS and HF-rTMS were significantly more effective than sham (a-tDCS: SMD = 2.44; 95% CI: 0.14–4.73, N = 4, total sample size = 121, p = 0.04, I2 = 95%; dual-tDCS: SMD = 2.36; 95% CI: 0.65–4.07, N = 4, total sample size = 178, p = 0.007, I2 = 95%; c-tDCS: SMD = 2.56; 95% CI: 1.80–3.32, N = 1, total sample size = 50, p < 0.00001; HF-rTMS: SMD = 1.62; 95% CI: 0.19–3.05, N = 4, total sample size = 133, p = 0.03, I2 = 91%). And a-tDCS showed significantly more effective compared with c-tDCS (SMD = 1.59; 95% CI: 0.94–2.23, N = 1, total sample size = 50, p < 0.00001). HF-rTMS was significantly more effective than iTBS (SMD = 0.96; 95% CI: 0.19–1.74, N = 1, total sample size = 29, p = 0.01. See Supplemental Table 1A and Supplemental Figure 2B). However, we found no significant effect of NIBS alternatives on attention function measured by NMA (Supplemental Table 1A and Supplemental Figure 3B).
Memory
Eight RCTs35,37,63–65,70,72,73 (335 participants) on memory comprised six NIBS alternatives. The pairwise meta-analysis suggested a significant difference between dual-tDCS, HF-rTMS, iTBS, and sham stimulation (dual-tDCS: SMD = 6.49; 95% CI: 2.46–10.51, N = 2, total sample size = 100, p = 0.002, I2 = 92%; HF-rTMS: SMD = 1.16; 95% CI: 0.13–2.19, N = 3, total sample size = 75, p = 0.03, I2 = 74%; iTBS: SMD = 1.06; 95% CI: 0.29–1.84, N = 1, total sample size = 30, p = 0.007). And HF-rTMS was significantly more effective than iTBS (SMD = 0.91; 95% CI: 0.14–1.68, N = 1, total sample size = 29, p = 0.02. See Table 2 and Supplemental Figure 2C).
In NMA, dual-tDCS is significantly more effective than sham (SMD = 6.38; 95% CI: 3.51–9.25, p < 0.05), a-tDCS (SMD = 6.18; 95% CI: 1.43–10.93, p < 0.05), HF-rTMS (SMD = 4.91; 95% CI: 1.33–8.50, p < 0.05), LF-rTMS (SMD = 4.29; 95% CI: 0.71–7.88, p < 0.05), and iTBS (SMD = 5.52; 95% CI: 1.03–10.01, p < 0.05), but not for other options compared directly and indirectly (Table 2 and Supplemental Figure 3C).
Executive Function
Five trials13,35,63,65,71 with 226 participants used NIBS (four stimulation choices) to improve EF. Dual-tDCS and LF-rTMS showed a substantial effect over sham (dual-tDCS: SMD = 3.97; 95% CI: 1.12–6.83, N = 3, total sample size = 150, p = 0.006, I2 = 97%; LF-rTMS: SMD = 1.34; 95% CI: 0.04–2.65, N = 1, total sample size = 12, p = 0.04. Supplemental Table 1B and Supplemental Figure 2D). NMA results showed no difference between NIBS treatment comparisons (see Supplemental Table 1B and Supplemental Figure 3D).
Secondary outcomes
Activities of daily living
Eleven RCTs13,24,35–37,63–65,71,72,75 with 515 participants and eight treatment alternatives were included for the secondary outcome of ADL. The pairwise meta-analysis suggested a significant difference between dual-tDCS and sham stimulation (SMD = 2.36; 95% CI: 0.05–4.68, N = 3, total sample size = 150, p = 0.05, I2 = 97%). cTBS showed a substantial effect over LF-rTMS (SMD = 1.74; 95% CI: 1.14–2.34, N = 1, total sample size = 60, p < 0.00001). LF-rTMS combined with cTBS options was more significant than either LF-rTMS or cTBS (versus LF-rTMS: SMD = 1.37; 95% CI: 0.81–1.94, N = 1, total sample size = 60, p < 0.00001; versus cTBS: SMD = 3.30; 95% CI: 2.51–4.10, N = 1, total sample size = 60, p < 0.00001. See Supplemental Table 1C and Supplemental Figure 2E). But NIBS options have no significant efficiency for improving ADL by NMA (Supplemental Table 1C and Supplemental Figure 3E).
Adverse effects
Six of 16 tDCS trials mentioned adverse or side effects, and in two studies13,56 mentioned mild side effects in active and sham groups. Liu et al. 13 reported that in the course of tDCS treatment, only six subjects experienced mild headaches and discomfort at a low discomfort rate. These side effects were relieved by relaxation. While in Jo’s 56 clinical trial, there were some adverse effects during tDCS that disappeared after a few seconds. Transient aching or burning sensations were reported in six cases, and transient skin redness at the electrode contact site was reported in three cases. Other four studies36,59,67,68 reported no adverse effects or dropout.
Nine of 13 TMS studies mentioned adverse or side effects; four69,73,74,77 reported mild to moderate side effects. There were seven patients in one of the four studies experienced transient dizziness or headache in the rTMS group, and two patients complained of light dizziness in the control group. 69 Another study reported one patient experienced a transient headache and another experienced dizziness in the rTMS group, and one patient experienced a headache in the sham group. 73 Jorge et al. 74 mentioned the mild level of side effects in the patients, including transient headaches (six patients) that were relieved with low doses of acetaminophen, local discomfort at the site of the stimulation usually produced by the tightness of the stimulation cap (five patients), and an exacerbation of initial insomnia observed in one patient. Finally, Fregni et al. 77 found that in the active group, only one patient reported a mild headache (contralateral to the side of TMS application) and one patient reported an increase in anxiety. In the sham rTMS group, one patient reported an increase in tiredness and one patient reported a mild headache. The rest of the five RCTs61,70, 71 ,75,76 reported no adverse effects. These articles did not observe severe side effect, such as seizes. The findings revealed that there was no discernible difference between tDCS and TMS in the frequency of adverse effects by NMA. (see Supplemental Table 1D and Supplemental Figure 2F).
SUCRA
According to the results of SUCRA (Table 3), HF-rTMS (SUCRA = 80.4) may be the best way to improve GCF. Table 3 showed that dual-tDCS may be the most effective intervention to improve attention (SUCRA = 70.9), memory (SUCRA = 99.5), EF (SUCRA = 75.0), and ADL scores (SUCRA = 73.4). Apart from sham stimulation (SUCRA = 78.3), tDCS (SUCRA = 37.2) may be slightly safer for patients than TMS (SUCRA = 34.5).
Rankings by SUCRA of different NIBS for improving cognitive function after stroke.

ADL, ability of daily living; a-tDCS, anode transcranial direct current stimulation; cTBS, continuous theta burst stimulation; c-tDCS, cathode transcranial direct current stimulation; EF, executive function; GCF, global cognitive function; HF-rTMS, high-frequency repetitive transcranial magnetic stimulation; iTBS, intermittent theta burst stimulation; LF-rTMS, low-frequency repetitive transcranial magnetic stimulation; NIBS, noninvasive brain stimulation; rTMS, repetitive transcranial magnetic stimulation; SUCRA, surface under the cumulative ranking line; tDCS, transcranial direct current stimulation.
Presents the first-ranking.
Presents the second-ranking.
Risk of bias assessment
Figure 1(b) shows the bias summary and graph. Eleven RCTs13,35,36,66–72,75 were graded as having a low risk of bias in a random sequence using the random number table approach. Nine trials13,35,36,66–68,70–72 had a low risk of bias in allocation concealment. Three studies13,63,75 were rated the high risk of performance bias for a single-blinded design; two of them13,75 mentioned the assessor-blind method, and the other one did not describe the blinding object. 63 Four trials24,37,65,73 without mentioning the blinding way were high-risk bias, with one 24 describing the study hypothesis blinded to the patients in the ‘Methods’ section. The remaining 13 RCTs35,36,64,66–72,74,76,77 were double-blinded designs. Most studies with an adequate description for incomplete results were rated as low risk of attrition bias, except for one. 24 No RCTs had reporting bias.
Exploration for inconsistency
We did not observe any significant inconsistency between direct and indirect comparisons. Formal testing found no statistically significant design inconsistency in GCF (χ2 = 0.16; p = 0.6938), attention (χ2 = 0.87; p = 0.9287), memory (χ2 = 0.98; p = 0.8068), EF (χ2 = 0.23; p = 0.6352), or ADL (χ2 = 0.56; p = 0.7547) and no local inconsistency.
Risk of bias across studies
Egger’s test found publication bias in attention (p = 0.016) but not in GCF (p = 0.261), memory (p = 0.132), EF (p = 0.108), or ADL (p = 0.153). Supplemental Figures 4–8 show funnel plot analysis and Egger’s test of included studies. The network map’s line colors could indicate the bias across different NIBS (Figure 2 and Supplemental Figure 1). According to the GRADE system, GCF and memory outcomes were classified as moderate-quality evidence, while attention, EF, and ADL outcomes were low-quality evidence (Supplemental Table 2).
Results of additional analyses
We did sensitivity analysis by deleting one RCT each time. The results (Supplemental Figures 4–8) showed no significant change compared with those before the investigation, indicating that the meta-analysis results were relatively robust.
We detected subgroup network analysis of GCF and memory scores according to the stimulation site. The left DLPFC (L-DLPFC) showed more effectiveness than the sham site (SMD = 1.77; 95% CI: 0.88–2.66, p < 0.05) and non-ipsilesional primary motor cortex (NI-M1) (SMD = 2.06; 95% CI: 0.53–3.60, p < 0.05) for GCF recovery. In terms of memory restoration, bilateral DLPFC is significantly more effective than sham (SMD = 8.65; 95% CI: 6.15–11.15, p < 0.05), L-DLPFC (SMD = 7.71; 95% CI: 5.11–10.32, p < 0.05), right DLPFC (R-DLPFC) (SMD = 7.35; 95% CI: 4.42–10.27, p < 0.05), bilateral M1 (SMD = 4.11; 95% CI: 1.10–7.13, p < 0.05), left frontotemporal cortex (L-FT) (SMD = 8.44; 95% CI: 5.50–11.37, p < 0.05), and right FT (R-FT) (SMD = 8.53; 95% CI: 5.60–11.47, p < 0.05). Bilateral M1 is significantly superior to sham (SMD = 4.54; 95% CI: 2.85–6.22, p < 0.05), L-DLPFC (SMD = 3.60; 95% CI: 1.75–5.45, p < 0.05), R-DLPFC (SMD = 3.23; 95% CI: 0.96–5.50, p < 0.05), L-FT (SMD = 4.32; 95% CI: 2.03–6.61, p < 0.05), and R-FT (SMD = 4.42; 95% CI: 2.13–6.71, p < 0.05). A comparison of the ranking of treatment sites revealed that stimulation over left DLPFC (SUCRA = 89.1) contributed the most to the improvement of GCF. On the other hand, stimulation over bilateral DLPFC (SUCRA = 99.9) contributed the most to improving memory function. Supplemental Figure 9 and Supplemental Table 3 showed our subgroup analysis results.
Discussion
Summary of evidence
This NMA demonstrated the possibility of obtaining evidence that HF-rTMS improves GCF in stroke patients compared with sham stimulation. In contrast to other NIBS protocols, dual-tDCS improved memory performance in stroke patients. However, various NIBS stimulation protocols show no significant impact on enhancing attention, memory, or executive function. Also, of the many NIBS protocols, HF-rTMS may be the most effective therapy for enhancing GCF; dual-tDCS may mostly increase attention, memory function, EF, and ADL. The NIBS examination of the safety of TMS and tDCS active stimulation protocols and sham stimulation revealed no significant difference. Moreover, tDCS may offer a higher level of patient safety. Our subgroup analysis demonstrated an effect favoring activation of the left DLPFC for enhancing GCF and bilateral DLPFC stimulation for enhancing memory performance.
As far as we know, there have only been a handful of papers comparing different TMS and tDCS protocols in stroke patients for cognition rehabilitation. A comparison of the efficacy of two NIBS protocols in patients with post-stroke dysphagia was observed.21,78 Following a stroke, patients with motor or speech impairments have been studied for various TMS protocols,79,80 and tDCS protocols.25,81
We believe our NMA offers fresh and significant insights into the relative efficacy of various NIBS therapy approaches. It provides evidence for selecting TMS or tDCS and comparing NIBS options for stroke survivors with cognitive dysfunction.
Our NMA results are partially compatible with a previous evaluation of the impact of NIBS on cognitive performance, especially on attention and memory deficits following stroke.27,31–33 For the main outcomes, rTMS improved GCF and memory in stroke patients,31–33 whereas tDCS does not.27,31 In the assessment of attention performance, all the meta-analyses of NIBS showed positive results,27,31–33 except the tDCS part in the review of Hara et al. 31 Due to the methodological restrictions of conventional meta-analysis, the authors of these reviews could only conduct pairwise comparisons. Furthermore, the authors analyzed a single group consisting of several rTMS or tDCS stimulation options. While low-frequency (1 Hz) transcranial magnetic stimulation seemed to exhibit a similar effect with a high-frequency (10 Hz) treatment for improving GCF and memory. 33 This might explain the uniformity of the combined results of different rTMS protocols. However, no researchers have performed a subgroup analysis of different tDCS options, so that, the combined effect of tDCS is more disagreement and needs further study and analysis. In addition, few papers were included in some of these meta-analyses, particularly for tDCS, for which only two literature mergers were conducted. 31 We discovered that one of the literatures 59 contained data that could not be retrieved directly: pre- and post-treatment ratios. Although it did not cause significant heterogeneity, it might still have a specific influence on the results.
In the secondary outcome evaluation, only the pairwise meta-analysis suggested a significant improvement for ADL by the dual-tDCS option, with no favorable effect by NMA. One NMA of tDCS 81 on motor function in stroke patients indicated that cathodal-tDCS enhanced ADL relative to sham stimulation and were superior to other treatments. Nonetheless, we discovered that all tDCS stimulation sites in the reviewed literature were affected, the non-affected, or the bilateral primary motor cortex, which may account for the discrepancy between our findings. Another two meta-analyses showed improvement by TMS treatment on ADL for stroke patients.32,33 However, the main outcomes reflecting ADL in these two reviews were both modified Barthel index (MBI), while our study set a combination of MBI and FIM scores as the target outcomes. Another reason for the different results from our study may lie in the different included literature. Xu et al. 33 included only three Chinese studies, but we did not take Chinese literature into account due to the consideration of the overall quality of the literature.
In terms of safety studies, we were in general agreement with the results of previous studies. The authors found no major adverse effects in an NMA 78 investigating noninvasive treatments for post-stroke dysphagia; Another NMA 21 reported that one rTMS study 82 and one tDCS study 83 said dizziness, headache, or nosebleed after the intervention. However, neither of these reviews compared rTMS and tDCS, probably due to the small number of articles. In our study, 12.5% (2/16) of tDCS articles reported side effects in both real and sham groups, with 25% (4/16) mentioning no adverse effect after tDCS intervention; 30.8% (4/13) of TMS studies reported adverse reactions in both the true and sham stimulation groups, while 38.5% (5/13) found no side effects. NMA ranked tDCS higher than TMS, although neither treatment was significantly different from sham stimulation. Mild to moderate adverse effects were reported and resolved quickly. Therefore, we have grounds to believe that these two NIBS approaches are reasonably safe.
Another challenge for therapists is selecting the stimulation site. The majority of research focused on the area of the DLPFC: 8/15 of tDCS studies selected excitatory stimulation for the DLPFC (four on L-DLPFC, one on R-DLPFC, and three on bilateral DLPFC). Eight of 12 TMS studies chose the DLPFC for stimulation site (seven on L-DLPFC and one on R-DLPFC). Although our study did identify a benefit of the left DLPFC region over other regions, functional imaging confirmation is still required to enhance the study’s objectivity. When just one target could be selected, all TMS studies used single-head stimulation; hence, the left DLPFC may be the preferred alternative. Dual-tDCS protocols with the anode over the left DLPFC and the cathode over the right DLPFC are favored and may be the first choice for enhancing memory function.
It was indicated that DLPFC was an important site in cognitive function. Some studies have shown that DLPFC is related to cognitive function mainly for processing speed, selective attention, working memory, and episodic memory.69–72,84–87 Besides, DLPFC plays an important part in the central executive network (CEN), which is responsible for high-level cognitive functions, notably the control of attention and working memory. 88 A meta-analysis has shown that HF-rTMS stimulation of DLPFC could improve cognitive function for healthy people, patients with Alzheimer’s disease, depression, executive dysfunction, memory complaints, and Parkinson’s disease. 89 The mechanism that produces these effects may be based on the theory of interhemispheric inhibition, where excitation of the left DLPFC (and/or inhibition of the right DLPFC) serves to modulate the function of the cognitively relevant cortex, and important brain networks, which consequently promotes the recovery of cognitive function. 90
However, it is currently unclear if DLPFC should be used as a stimulation location for all patients, regardless of stroke type, stroke origin, or damage site, despite functional neuroimaging studies suggesting DLPFC plays a crucial role in the neural circuitry of cognitive function and it has been shown that therapeutic interventions, which aim to interfere with improper cortical activity, may address pathological connections not only at the DLPFC but also among distant brain regions.91,92 In our findings, the DLPFC is not the only beneficial site. A treatment plan delivered bilaterally to the M1 region is effective in improving memory function in stroke patients. Inadequate studies included in our analysis, notably the lack of studies using stimulation sites other than the DLPFC, also contributed to the outcome. Furthermore, the original study did not perform a stratified analysis of the different stroke locations or stroke types, which suggests that future studies might be able to concentrate on these areas.
Our results for primary and secondary indicators imply a high degree of heterogeneity, presumably because we aggregated the impacts of different scales reflecting similar functions, intervention parameters (number of stimuli, current or magnetic stimulation intensity, etc.), and populations. A large number of outcome variables and a small sample size might cause publication bias in attention outcomes. More than half of EF and ADL studies did not address random sequence generation or allocation concealment; the research was less rigorous in design and less descriptive in the report.
Limitations
Our study has several limitations. First, NIBS (particularly c-tDCS and cTBS) to improve cognitive function after stroke lacked high-quality RCTs, and even fewer trials examined stroke patients’ memory and EF, thus the certainty of the evidence is reduced. Our study on the subgroup of protocols and stimulation sites is limited by the absence of related RCTs in comparison to published meta-analyses. However, this constraint points the way for future research. And due to the small number of included studies and the several ways of cognitive function evaluation, the method we pooled the data may have resulted in a large degree of heterogeneity, which compromised the robustness of the conclusions. Some of the included literature incorporated various rehabilitation training, such as visual reaction (VR), computer-assisted cognitive training (CCT), and so on, and the kind and duration of stroke varied, leading to considerable heterogeneity. A lack of relevant gray research may prejudice study selection. Half of the trials had questionable allocation concealment bias, reducing RCT quality.
Second, although we did not detect inconsistencies in the primary and secondary outcomes, this does not mean any inconsistencies occurred. 41 This is partly because most of the network diagrams are not closed loop, which leads to the fact that our analyses are not strictly NMA or multiple treatment comparisons (MTCs), but belongs partly to the NMA genus of adjusted indirect treatment comparison (ITC). 93
Finally, we only evaluated the immediate effects after NIBS treatment, and some articles followed up on the long-term effects, which deserve further concentration.
Conclusion
Our NMA of RCTs indicates that NIBS positively affects GCF and memory performance after stroke, with no apparent side effects. When NIBS is utilized to enhance GCF, HF-rTMS, particularly over the left DLPFC, maybe the appropriate therapeutic option. Dual-tDCS, over bilateral DLPFC, may improve memory function after stroke, which is superior to other NIBS options. No difference regarding safety (in terms of dropouts and adverse events) was seen between different types of NIBS.
However, the effect of NIBS on attention, EF, and ADL performance was insignificant, while the impact of c-tDCS and cTBS protocols was even weaker. New RCTs of interventions of high quality are required to increase the exploration of the efficacy of different NIBS intervention modalities, particularly tDCS and TBS protocols, for different dimensions of cognitive function to establish their evidence of efficacy with greater reliability. In the future, we advise clinical therapists to use left DLPFC site HF-rTMS and bilateral DLPFC dual-tDCS as supplementary treatments for cognitive impairment and memory deficits in stroke rehabilitation.
Supplemental Material
sj-docx-19-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-docx-19-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-20-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-docx-20-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-21-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-docx-21-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-22-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-docx-22-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-docx-23-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-docx-23-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-1-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-1-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-10-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-10-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-11-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-11-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-12-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-12-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-13-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-13-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-14-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-14-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-2-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-2-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-3-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-3-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-4-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-4-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-5-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-5-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-6-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-6-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-7-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-7-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-8-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-8-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-jpg-9-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-jpg-9-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-png-15-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-png-15-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-png-16-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-png-16-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-png-17-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-png-17-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-png-18-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-png-18-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Supplemental Material
sj-png-24-taj-10.1177_20406223231168754 – Supplemental material for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials
Supplemental material, sj-png-24-taj-10.1177_20406223231168754 for Comparative efficacy of different noninvasive brain stimulation therapies for recovery of global cognitive function, attention, memory, and executive function after stroke: a network meta-analysis of randomized controlled trials by Yao Wang, Wan Liu, Jiu Chen, Jianling Bai, Hao Yu, Hongxia Ma, Jiang Rao and Guangxu Xu in Therapeutic Advances in Chronic Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.